Article Text

Abstract
Objectives To report the findings of a case-series of 10 children suffering with intractable epilepsies in the UK to determine the feasibility for using whole-plant cannabis medicines to treat seizures in children.
Setting This study was conducted retrospectively through collecting clinical data from caretakers and clinicians on study outcome variables. Participants were recruited through the MedCann Support and End our Pain charity groups which are patient representative groups that support children who are using medical cannabis to treat their epilepsies. Medicines were prescribed to patients by clinicians in both National Health Service and private medical practices. Follow-up calls were conducted throughout the period January 2021 to May 2021 to keep data recorded up to date.
Participants Ten children, 18 years old or under, with intractable epilepsies were recruited from two charities. There were no limitations on diagnosis, sex or ethnic origin.
Interventions Participants were treated with a range of whole-plant medical cannabis oils. Individual dosing regimens were determined by clinicians.
Primary outcome measure The primary outcome measure was seizure frequency.
Results Seizure frequency across all 10 participants reduced by 86% with no significant adverse events. Participants reduced use of antiepileptic drugs from an average of seven to one following treatment with medical cannabis. We also noted significant financial costs of £874 per month to obtain these medicines through private prescriptions.
Conclusions This study establishes the feasibility of whole-plant medical cannabis as an effective and well-tolerated medicine for reducing seizure frequency in children suffering with intractable epilepsies. These findings justify the potential value of further research into the reported therapeutic benefit of whole-plant medicinal cannabis products.
- neurology
- pharmacology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Since the 1800s there has been significant anecdotal evidence of the value of medicinal cannabis in treating childhood epilepsies
There have been four successful randomised controlled trials showing the therapeutic efficacy of cannabidiol for the treatment of Lennox-Gastaut, Dravet’s and Tuberous sclerosis syndrome.
There is limited scientific evidence available that has investigated whole-plant cannabis medicines containing Tetrahydocannabinol (THC) in paediatric epilepsies.
What this study adds?
The reduction of seizures demonstrates the feasibility for this form of treatment in patients with paediatric intractable epilepsies.
The potential value of further research into the reported therapeutic benefit of whole-plant medicinal cannabis products.
Introduction
Though used for millennia in eastern medicine, the advent of medical cannabis as a therapeutic tool to treat seizures in the west was first noted in 1843 by an Irish physician, Dr O’Shaughnessy. He observed that cannabis tinctures resolved seizures in a febrile infant, thus claiming that medicine had found an anticonvulsant of the highest order.1 In 1971, both recreational and medical cannabis were made illegal in the UK under the Misuse of Drugs Act 1971 and so cannabis research largely ceased. Led by parents whose children had responded well to whole-plant medical cannabis extracts but who had failed on conventional antiepileptic drugs (AEDs) and purified cannabidiol (CBD) (Epidyolex), medical cannabis was re-initiated as a medicine in the British pharmacopeia in 2018.
Cannabis-based medical products (CBMPs) comprise a broad range of medicines. They can be plant-based or synthetic and vary from purified single compounds (often THC or CBD) to complex mixtures of hundreds of molecules, in multiple formulations (oils, solutions, sublingual sprays, tablets and capsules), with multiple delivery mechanisms (oral, nasal, rectal and inhalation).2
Of the products licensed in the UK, Epidyolex (licensed for the treatment of epilepsy) is an isolate, Sativex (recommended for spasticity associated with multiple sclerosis) comprises a 1:1 CBD:THC isolate ratio, and nabilone (eg, used to treat nausea and vomiting due to cancer chemotherapy) is a THC analogue.
A combination of both THC and CBD from whole plant extracts were found to be superior to CBD alone in children suffering from various forms of epilepsy.3
Despite the change in legal status of medical cannabis, most of these children have not benefited as to date there has been only three National Health Service (NHS) CBMPs prescriptions made in total and only two in children.4 Many patients are thus forced to resort to private treatment which costs up to £2000 per month.3
Reasons for this resistance are multifactorial.5 6 One of the most argued by clinicians who might be prescribers is the lack of evidence for efficacy of medical cannabis. By this they usually mean that there are no randomised controlled trials (RCTs) that prove efficacy and without these they are not prepared to prescribe. To a lesser extent this has also limited National Institute for Clinical and Healthcare Excellence (NICE) support.7 It is generally accepted that RCTs though powerful are not the only means to generate evidence for the value of treatments. The previous head of NICE and the Medicines Healthcare Regulatory Agency (MHRA) Sir Michael Rawlins in his 2008 Royal College of Physicians Harveian lecture argued that there are many other ways of collecting useful clinical evidence highlighting:
‘Randomised controlled trials, long regarded at the ‘gold standard’ of evidence, have been put on an undeserved pedestal. Their appearance at the top of ‘hierarchies’ of evidence is inappropriate; and hierarchies, themselves, are illusory tools for assessing evidence. They should be replaced by a diversity of approaches that involve analysing the totality of the evidence-base’.8
In a recent position statement, NICE declared their willingness to acknowledge additional data sources including ‘real world’ data and ‘relevant data collected outside of the context of traditional trials’.9 One of these other sources of data, real-world evidence, comes from patient case-series with before and after outcome measures. These are particularly useful for conditions where RCTs are unlikely or impossible to perform in examples of rare and idiopathic conditions and especially in paediatric medicine. For this reason, we have conducted an outcome assessment of the use of medical cannabis in 10 children with severe treatment-resistant epilepsy who have all failed on multiple traditional AEDs and many of whom have failed on the licensed CBD preparation Epidyolex. Epidyolex is a licensed, pharmaceutical grade, purified CBD medicinal product that is produced by GW Pharma. It is the first and only approved prescription CBD. It is approved to treat seizures associated with Lennox-Gastaut syndrome (LGS), Dravet syndrome or tuberous sclerosis complex (TSC) in patients 1 year of age and over.
Our previous study, an open label retrospective study of the impact of medical cannabis in 10 patients found whole plant extracts to be superior to CBD isolate and a mean 80% reduction in seizure frequency in a range of intractable childhood epilepsies where standard treatment had failed.3 A subsequent qualitative follow-up study highlighted the various benefits patients and their families experienced as a result of treatment with CBMPs.2
Methods
Study design
We recruited participants through two charities, MedCann Support and End Our Pain, which represent children who are using medical cannabis to treat their intractable epilepsies. At the time of the study there were a total of 40 participants across both charities that were using whole-plant medical cannabis products to treat their epilepsies. The study team liaised with these charities to disseminate the research proposal and participant information sheets to potential participants via the charities email database and social media pages. A total of 26 participants subsequently provided consent for involvement in the study and provided data on study outcome measures (see online supplemental appendix). Ten of these have been previously reported.3 Of the remaining 16 participants, only 10 participants are involved in this current study. The attrition of six participants was due to missing data (n=5) and being over the age of 18 (n=1). Participants’ data were collected from their parents or carers via telephone or video conference calls for the period January 2021 to May 2021.
Supplemental material
Study outcomes
The primary study outcome was to assess the percentage change in monthly seizure frequency in participants following initiation of medical cannabis. The secondary study outcomes were to assess the impact of medical cannabis on changes in AED use, to report the concentrations and doses of medical cannabis used by these patients and to document the costs incurred from attaining these prescriptions.
Patient and public involvement
Participants, parents and clinicians helped to design the variables and information collected in the study. Working closely with patient groups will ensure the results are disseminated to relevant stakeholders, including patient representative groups and clinical governance bodies.
Participants
We engaged carers of patients, following their consent to engage in the study, to provide information on patients age, diagnoses, current AEDs, previous AEDs, previous CBMPs, current CBMPs, monthly seizure frequency pre-initiation and post-initiation of CBMPs, dose of THC and CBD and cost of CBMPs. Data were confirmed with clinician reports where available.
Study medication
All participants received whole plant extract CBMPs either through private prescription or through the NHS. The CBMPs used included Bedrolite (<1% THC and 9% CBD), Bedica (14% THC and <1% CBD), Celixir 20 (<1% THC and 20% CBD), Sweet Pink CBD (<1% THC and 10.6% CBD) and Althea 100 (<1% THC and 10% CBD). The prescription of these medicines were initiated by clinicians and all participants continued to use these medicines at the last follow-up call. Individual dosing regimens are described in table 1.
Demographic and clinical data from 10 patients enrolled in the study
Statistical analysis
Descriptive analysis on group percentage change in seizure outcome is provided. Other variables including mean AED use preinitiation and postinitiation of CBMP and mean cost are also described. No significance testing was performed due to no predefined terminal period for data collection.
Results
Clinical and demographic details
A total of 10 patients were included in the current study. The mean age of participants was 6.2 years old (range 1–13). All clinical and demographic details can be viewed in table 1.
Epileptic aetiologies
The patients presented with a range of epileptic aetiologies including predefined syndromes, rare genetic disorders and undiagnosed epileptic encephalopathies. Two patients presented with genetic aetiologies (PCDH19 mutation, chromosome deletion), one with Dravets syndrome, one with Doose syndrome, two with CDKL5 deficiency disorder, one with West syndrome, one with Rett Syndrome, one with Aicardi syndrome and one with undiagnosed refractory epilepsy.
Comorbid diagnosis
Three of the participants presented with multiple comorbid diagnoses. The most reported being infantile spasms (N=2), learning disabilities (N=1) and global developmental delay (N=1).
Medication
Patients reported a mean of 7 (±4.58) AEDs prior to initiation of CBMPs which reduced to a mean of 1 (±1.23) per patient with 7 patients managing to completely wean off all AEDs. The most common secondary intervention in the cohort was a ketogenic diet (N=4) prior to initiation of CBMP which was not effective in any patient and was subsequently discontinued. One patient had a current vagal nerve stimulation implant.
Two patients using Epidyolex had failed to respond to this NICE recommended CBMP for treatment resistant epilepsy.
One patient saw a significant worsening of symptoms including an increase in seizure frequency when switching from Bedrolite and Bedica products to other whole-plant CBMPs. The other three patients that changed CBMPs from Bedrolite and Bedica to other products noted burden of cost as the primary reason for switching product, though all these patients reported the efficacy of Bedrolite and Bedica in reducing seizure frequency.
Seizure frequency
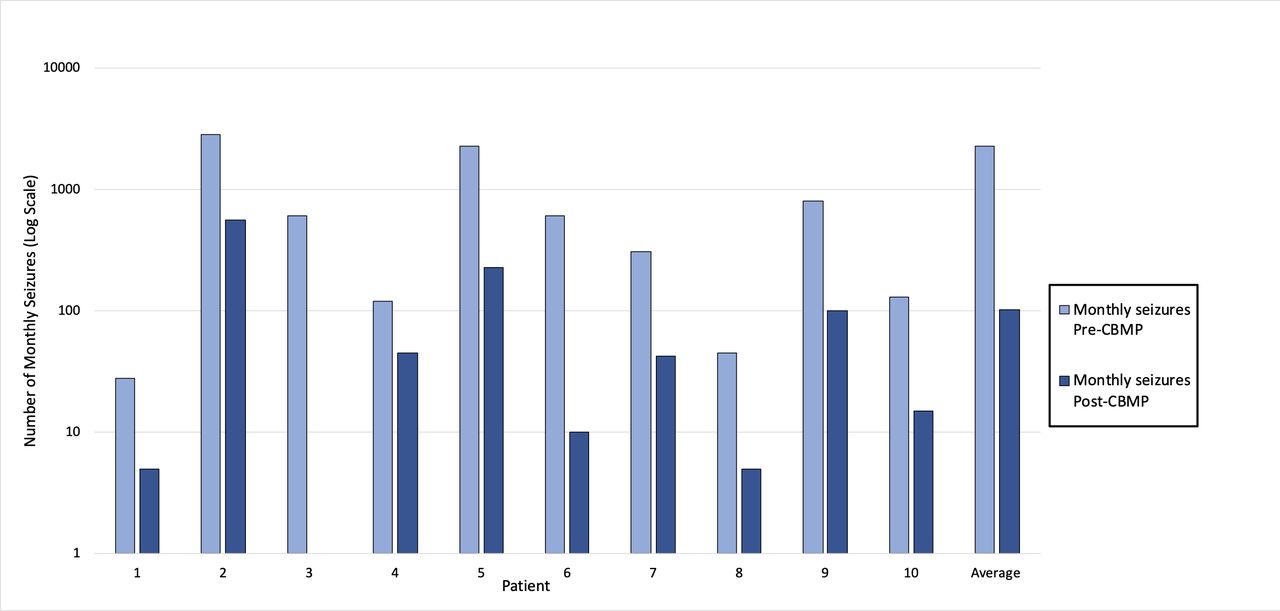
Figure 1 shows the findings from the 10 participants enrolled in this case-series. Here we show individual and mean changes in seizure frequency preinitiation and postinitiation of CBMP (note log 10 scale).
{kind=link}
Monthly seizure frequency pre-CBMP and post-CBMP in 10 patients suffering with childhood-onset severe intractable epilepsies. CBMP, cannabis-based medical products.
The monthly seizure frequency reduced for all 10 patients with an overall mean of 86%.
Dose of CBMP
All patients were using whole-plant cannabis products which contain a range of terpenes, flavonoids and minor phytocannabinoids. We are currently in process of analysing the respective components of each medication in this study which we plan to report on. For this study, we are only able to report on the respective doses of THC and CBD. For THC dosage, patients consumed a mean (SD) of 5.15(±6.8) mg of THC a day and for CBD 171.8 (±153.3) mg of CBD daily.
Cost
The mean cost for participants medical cannabis prescription was £874 per month. One participant had obtained their medical cannabis prescription on the NHS.
Other symptoms
Parents and carers reported significant improvements in health and well-being of their children following initiation of whole-plant CBMPs. Particularly, these improvements were noted in sleep, eating, behaviour and cognition. We did not specifically ask for adverse effects here, but in a follow-up qualitative study (comprising a subset of eleven of these patients across the current study and our previous one2 3) parents were asked about adverse effects specifically. Only few minor adverse effects, such as tiredness before exact dosing were reported. Our patient group almost universally reported highly improved cognitive and behavioural outcomes, likely due both to reduced seizure frequency and reduced use of other AEDs.
Discussion
This study shows the effectiveness of whole-plant medical cannabis in a group of patients suffering with severe intractable childhood-onset epilepsies. The reduction in monthly seizure frequency in our group demonstrates the feasibility for this medication in such patients.
Carers reported sustained and significant improvements in behavioural, psychological and cognitive faculties associated with medical cannabis use.
Our findings are in line with several observational and controlled interventional studies that have seen significant reductions in seizure frequency following treatment with medical cannabis. Moreover, our data suggest that whole-plant medical cannabis products are superior to isolated CBD products in the patients examined. To date, double-blind placebo controlled RCT evidence is only available for isolate CBD in three rare forms of epilepsy: LGS, Dravet syndromes and TSC.10–13 One such study showed a reduction of 22.8% in seizures in children with Dravet syndrome10 while another study by the same author in LGS patients using CBD isolate reported a 42% reduction in drop seizures.11 To expand on this another study12 conducted a similar double-blind placebo controlled RCT in patients with LG and similarly reported a 44% decrease in drop seizure frequency in the CBD isolate group. A more recent interim analysis of another study13 sought to examine the effects of add-on CBD isolate to standardised treatment for seizures associated with TSC, finding a 48% reduction in seizures versus 27% for placebo. From the RCT evidence alone it is clear that CBD isolate is a safe but not especially effective intervention for seizures in LGS, Dravet and TSC.
As noted by Rawlings8 there are several limitations of RCTs in assessing evidence for novel medical interventions. For example, the strict inclusion and exclusion criteria of such studies limits the generalisability of findings. This is of particular importance in the case of paediatric-onset intractable epilepsies where the majority of epilepsies diagnosed under the age of 15 are of idiopathic origin.14 Thus, observational studies allow for a wider participation and a broader patient pool to aid in understanding the scope of medical cannabis as an intervention. We acknowledge that retrospective observational research is subject to recall, and this is an inherent limitation of such designs. Given the rarity of such patient populations with these forms of epilepsy prospective studies would be challenging and take a long time to complete.
Current NICE guidance, limiting prescribing for medical cannabis for this patient group to CBD in the form of Epidyolex, has relied on four RCTs in a limited range of diagnoses. Two of the children in our sample had failed on Epidyolex. For this reason, NICE guidance has recently been updated to clarify that this should not deter clinicians from prescribing off-license medical cannabis products such as the whole-plant cannabis medicines of which our data support for such prescribing.
Limitations
Our data has a number of limitations. First, the data collection was retrospective and based on parental recall (though these often-contained seizure diaries). Second, there was no randomisation or placebo and so there was no comparator or placebo group. Third, there may be bias in that the parents that agreed to provide the data were the ones in which the children had had the largest clinical impact from their medical cannabis. Fourthly, there was no assessment of the impact of removing the intervention to validate the enduring need for treatment. Finally, the patient number was small, but it did accord with previously reported outcomes in a previous study.3
Further research is required to elucidate the mechanisms by which the respective additive constituents of whole-plant products lead to superior clinical results. Several encouraging preclinical lines of work highlight the anticonvulsive and neuroprotective roles of several minor phytocannabinoids including CBDV, D9-THCV and CBG.15 THC exerts its anticonvulsant effects via activation of the CB1 receptor and subsequent modulation of glutamatergic excitatory activity in the brain.16 Nonetheless, the investigation of the putative anticonvulsant effects of these cannabinoids needs to be investigated in-vivo to gain a full appreciation for their therapeutic efficacy. While we note the difficulty in conducting prospective studies, these could be designed to identify children who are most likely to benefit from medical cannabis and those that are not in order to stratify treatment packages earlier during their disorders. Such a study would serve to ameliorate the current poor prognosis within this severely ill population.
Mitigating risk is the cornerstone of clinical judgement and there are some opponents of the therapeutic use of THC in children and adolescence. Concern over the deleterious effects of whole-plant medical cannabis must be compared with the known iatrogenic effects of mainline AEDs. One randomised clinical trial of phenobarbital when used chronically for seizure prophylaxis found significant impairment of developmental trajectories17 as well as a large decrease in global IQ and verbal learning.18 In another double blind RCT valproate was associated with poorer attentional performance compared with other AEDs.19
Additionally, adverse effects from AEDs are the leading cause of treatment discontinuation and after seizure frequency, the major determinant of impaired health-related quality of life in people suffering with epilepsy. Adverse events are commonly reported with AEDs with one such study reporting 1139 adverse drug reactions in 124 young people using antiepileptic drugs20 while another study reported that behavioural problems and somnolence were the most common adverse drug reactions and that AED polytherapy significantly increase the likelihood of children developing such reactions.21
We believe that our data on whole-plant medical cannabis in childhood-onset severe treatment-resistant epilepsy, provides evidence to support its introduction into the NHS within current NICE prescribing guidelines. Such a move would be hugely beneficial to the families, who in addition to having the psychological distress of looking after their chronically ill children, have also to cover the crippling financial burden of their medication.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by Imperial College Research Ethics Committee (20IC5830 ICREC Committee (01/05/2020).
Acknowledgments
We would like to acknoweldge all the families and carers that assisted us with data collection for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Rayyanzafar6
Contributors RZ, DJN and LP analysed the data. AS added sections of medical cannabis. All authors developed the initial manuscript and all authors reviewed and agreed to the final manuscript. RZ is the guarantor for this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Professor David John Nutt is Chair of the charity Drug Science, Lawrence Phillips is an expert member, Rayyan Zafar is an honorary research assistant and Dr Anne Katrin Schlag is Head of Research of the same charity. Drug Science receives an unrestricted educational grant from a consortium of medical cannabis companies to further its mission, which is the pursuit of an unbiased and scientific assessment of drugs regardless of their regulatory class.
All Drug Science committee members, including its Chair, are unpaid by Drug Science for their effort and commitment to the organisation. Dr Schlag is also a scientific advisor to the Primary Care Cannabis Network and an executive member of the Cannabis Industry Council, both of which are unpaid roles. None of the authors would benefit from the wider prescription of medical cannabis in any form.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.