Article Text

Abstract
Background Management of acute pain should commence at the earliest opportunity, as it has many short-term and long-term consequences. A research priority of Paediatric Emergency Research in the UK and Ireland (PERUKI) was to examine paediatric pain practices.
Objective To describe the outcomes for paediatric pain management of minor injuries presenting to emergency departments (EDs) across PERUKI.
Methods A retrospective service evaluation was performed over a 7-day period in late 2016/early 2017 across PERUKI sites, and analysis performed using an adapted Donabedian framework. Patients under 16 years presenting with minor trauma were eligible, and data were collected on prehospital management, pain assessment, analgesia administered and injury diagnosed.
Results Thirty-one sites submitted data on 3888 patients. There were 111 missed cases (missed rate 3.6%). The most common injuries were sprains, lacerations, contusions/abrasions and fractures. Documentation of receiving analgesia before arrival in ED occurred in 21% of patients (n=818). A pain assessment was documented in 57.5% of patients (n=2235) during their ED visit, and 3.5% of patients had their pain reassessed (n=138). Of the patients who presented in severe pain (pain score 7–10 or rated severe), 11% were reassessed. Site variability of initial pain assessment ranged from 1.4% to 100% (median 62%). The characteristics of the top quartile performing centres against the bottom quartile performing centres based on completion rate of initial pain scores were identified.
Conclusion Pain assessment was documented in under 60% of children with minor injury, re-assessment of pain was almost completely absent, data and outcomes were missing in a substantial volume of patients, indicating that pain management and the associated outcomes have not been adequately addressed and prioritised within existing network structures and processes.
- Pain
- Analgesia
- Pharmacology
- Therapeutics
- Nursing Care
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Oligoanalgesia and failure to reassess pain scores have been repeatedly demonstrated in the acute paediatric pain management in emergency departments in national audits.
What this study adds?
The existing processes resulted in pain assessment in <60% of children, almost completely non-existent pain re-assessments and missing pain outcomes in patients with minor injury.
Outcomes related to paediatric pain are highly variable across sites. More research is required to determine the core structures and processes to overcome the suboptimal outcomes for paediatric pain management.
INTRODUCTION
‘It is unacceptable to be ignorant of anyone’s pain in the 21st century, particularly those who are vulnerable’.1 Inadequate management of acute pain has many consequences and it should be managed at the earliest opportunity,2 3 yet despite availability of consensus standards4 and guidelines5–7 on childhood pain, its management remains suboptimal. A UK study from emergency departments (EDs) revealed pain management was not well aligned with the core priorities of the ED and not perceived to be a key organisational priority for which staff were held accountable.8
Despite the Royal College of Emergency Medicine (RCEM) identifying pain management as the most popular indicator of ED quality of care in 2002,9 an ongoing significant gap has been identified between standards and clinical practice. One recent RCEM audit revealed substandard performance across fundamental, developmental and aspirational standards for paediatric pain management related to limb fractures.10
Paediatric Emergency Research in the UK and Ireland (PERUKI) identified pain practice as a priority research domain.11 Donabedian created a conceptual model that provides a framework for examining health services and evaluating quality of healthcare which has been used in several domains of healthcare to drive improvement.12 Health services research utilising the Donabedian conceptual framework (structure, process and outcome) is widely applied in evaluating quality of care.12 13 Healthcare pain outcomes cannot be understood in isolation, as they are a product of health system-related structures and processes which include the prehospital care, resources (guidelines, staffing, tools, medicines etc) and processes at each department from reception to discharge.14 The structures related to paediatric pain are the physical and organisational characteristics where healthcare occurs and the processes are the actual steps involved in optimal analgesic practices (recognition of pain, assessment, intervention, reassessment and maintenance of pain relief). A previous PERUKI study identified high variation of pain management structures in the network.15 The foundation for improving quality of paediatric pain management should include the identification of gaps in our knowledge on pain related processes and outcomes.
The aim of this study is to describe the network’s processes and resultant ‘real-world’ pain outcomes for children and young people with all minor injuries in our EDs, to inform baseline network characteristics and identify gaps with a view to identifying further areas for improvements.
Methods
Study design and setting
This retrospective service evaluation occurred across PERUKI,16 a research collaborative in both urban and rural settings. The sites in the network invited to participate in the study (n=34) were based in England 76%, Ireland 12%, Scotland 6%, Wales 3% and Northern Ireland 3%. The hospital characteristics of these sites were tertiary centres 23 (67.6%) or district general hospitals 11 (32.4%). The annual paediatric attendance ranged from 11 500 to 65 000. Eighteen sites (52.9%) were trauma centres, 11 (32.4%) were trauma units and 5 (14.7%) were neither. Participating sites identified a site lead for this study, who was responsible for completing all elements.
Data pertaining to the assessment and management of pain were identified and abstracted from the clinical charts of all children who presented over a 1-week period with minor injuries for any seven consecutive days from 28 November 2016 to 16 January 2017. Study case report forms were retrospectively completed from routinely collected clinical data. Data included demographic details, injury characteristics, disposition and related processes and outcomes during the attendance. The case report form and the accompanying guidance notes are available as online supplemental appendix 1. In parallel to the patient level data being collected a site survey was conducted.15
Supplemental material
Eligibility criteria
All children aged from birth to 15 years (prior to their 16th birthday), presenting with minor trauma, were eligible. Exclusion criteria were (1) trauma team activation, (2) major trauma (injury severity score >15),17 (3) left before completion of treatment or (4) missing injury details.
Data collection, analysis and statistical analysis
Injury classification criteria were provided. The optimal method for identifying eligible children at each site was delegated to the site lead. Charts of potentially eligible participants were reviewed, and eligibility confirmed. Data were collected in Excel, irrevocably anonymised, and transmitted securely to the central study team. The pain score/rating performed used a validated pain scale and the time of assessment was recorded for each pain assessment. Medications administered including time, dosage, route and if given based on patient group directive were recorded. We applied an adapted paediatric pain Donabedian framework12 to the structures, processes and outcomes involved in paediatric pain management in the emergency setting (framework available as online supplemental appendix 2).
Supplemental material
Data were analysed using Statistical Package for Social Sciences (SPSS, V.21.0 for Windows). Data are presented as categorical and continuous variables, and descriptive and comparative analyses were performed. Results are expressed as frequency (percent) or medians with IQR. The pain score per cent details the number of patients who had a pain score recorded over the total number of patients expressed as a percent. Analysis was performed using Pearson χ2 and Mood’s median test as appropriate. Alpha level was set at 0.05.
Patient and public involvement
One of the top factors affecting parental ED satisfaction is pain management18 which was also a research priority of PERUKI11 which guided the design. Routinely collected patient data was retrospectively collected and consent was not deemed necessary for the anonymised data. Collective results are presented which is detailed with site characteristics.
Results
Site responses
Data were completed by 31 sites from the 34 who were invited to submit data. Twenty-one sites (67.7%) were tertiary centres and 10 (32.3%) were district general hospitals; 11 (35.5%) were mixed adult/paediatric hospitals with a separate paediatric ED, 10 (32.3%) were mixed adult/paediatric hospitals with a combined paediatric ED, and the remaining 10 (32.3%) were paediatric hospitals. Seventeen sites (54.8%) were trauma centres, 10 (32.3%) were trauma units and 4 (12.9%) were neither (table 1). The annual paediatric attendance ranged from 11 500 to 65 000 (median 30000, IQR 24 500–38500).
Site characteristics and rates of documentation of prehospital analgesia, pain score and repeat pain score
Data were submitted for 3888 patients, with a range across sites from 11 to 292 (median 104, IQR 80–159.5). Data were collected for 7 days in 30/31 sites (97%). The remaining site collected for 4 days (omitted 43 patients), and one site which collected data for 7 days included only 60% of eligible patients (51 patients omitted). Clinical records were not located for 17 cases. The total number of missed eligible patients was 111, giving a missed rate of 3.6% (n=111/3999). The individual site rates of prehospital analgesia, and performance of initial and subsequent pain scoring are described in table 1.
Patient and injury characteristics
The primary injury characteristics of included patients are shown in table 2.
Primary injury type (n=3888)
The proportions of injury type varied by age band—for example, sprains were more common in older age groups (6 years and older), lacerations were most common in 2–5 years old, and injuries such as head injuries and burns/scalds showed a more even distribution across age groups. Full details are available as online supplemental appendix 3.
Supplemental material
Mode of transport
Most patients (3578, 92%) self-presented or were brought by carers, with 170 (4.4%) conveyed by ambulance, 47 (1.2%) were transferred from other ED’s and 9 (0.2%) came from GP/walk-in centre. This was unknown/not documented in 84 patients (2.2%). Prehospital analgesia was given to 818 (21%) of patients, this was highest in patients transferred from other EDs 53.2% (n=25), and children brought by ambulance 51.4% (n=89). The proportion was lower in children who self-presented at 18.9% (n=674).
Time from injury to ED presentation varied, with 48% (n=1866) registering within 4 hours of injury, 10.3% (n=400) between 4–12 hours, 9.4% (n=366) between 12 and 24 hours, and 14.2% (n=554) after more than 24 hours.
Prehospital analgesia
Documentation of prearrival analgesia showed analgesia was administered to 818 patients (21%), 1831 patients (47.1%) had no analgesia, and 1239 (31.9%) did not have this information documented. There was a statistical relationship between mode of transport and if prehospital analgesia was given (p<0.0001). The rate of prehospital analgesia administration was greater for patients who arrived by ambulance or who were transferred from another ED 51.8% (95% CI 45.2% to 58.4%), than patients who presented by all other methods 19.2% (95% CI 17.9% to 20.5%) (p<0.001).
Pain assessment(s)
For 2235 patients (57.5%), a pain assessment was documented at some point during their ED attendance. This varied with a range of 1.4% to 100% (median 62%, IQR 37.4%–83%) across sites (table 2). Of those with a documented pain assessment, 138 (6.2%) had a repeat pain assessment. The most frequently documented pain score was 0 (no pain), occurring in 41% of cases (table 3). A repeat assessment of pain was more likely to occur in patients with higher initial pain scores, or those who received analgesia in the ED (available in online supplemental appendix 4)
Supplemental material
Initial pain score/assessment when performed (n=2235), and analgesia administration according to pain score
In the five sites which have local policy/guidelines on all aspects of pain assessment and management as described previously,16 the mean per cent of patients with pain scores recorded was 42.9% (95% CI 39.1% to 46.7%). This compared with the six sites where there were no local guideline documents where the mean rate of patients with pain scores recorded was 47.3% (95% CI 43.9% to 50.6%).
The time frame for performing repeat pain assessments was not uniformly carried out in all centres. The median time interval between pain assessments in 122 episodes of pain reassessment was 68.5 min (IQR 37.25–110.75 min) with a range from 4 minutes to 254 minutes. In 29 instances where the pain was reassessed the interval was unknown as the time of one of the pain assessments was not documented. The length of stay in the ED was recorded in 94.8% of presentations (n=3648). The median length for the minor injury management was 113 min (IQR 72–167 min).
Analgesia administration
An offer of analgesia was documented in 1812 patients (46.6%), of whom 1533 (84.6%) were administered analgesia. In just under half, it was not known whether analgesia had been administered (19.7%) or why it had not been given (27.4%). Table 4 shows the breakdown of administered analgesic agents.
Analgesic agents administered to patients during their ED attendance (n=1991)
Of the 1991 analgesic agents administered, 1067 were given based on patient group directions (53.6%). Eighty-six patients (2.2%) (for 90 prescriptions) received an opiate, and one patient received intravenous ketamine. Twenty patients (0.5%) required procedural sedation during their attendance.
Analgesia administration stratified by baseline pain score
For patients with a pain score, the cumulative percentage of analgesia administration varied by pain score and time (figure 1). The higher the pain score, the greater the proportion that received analgesia (52.8% with mild pain, compared with 86.3% with severe pain).
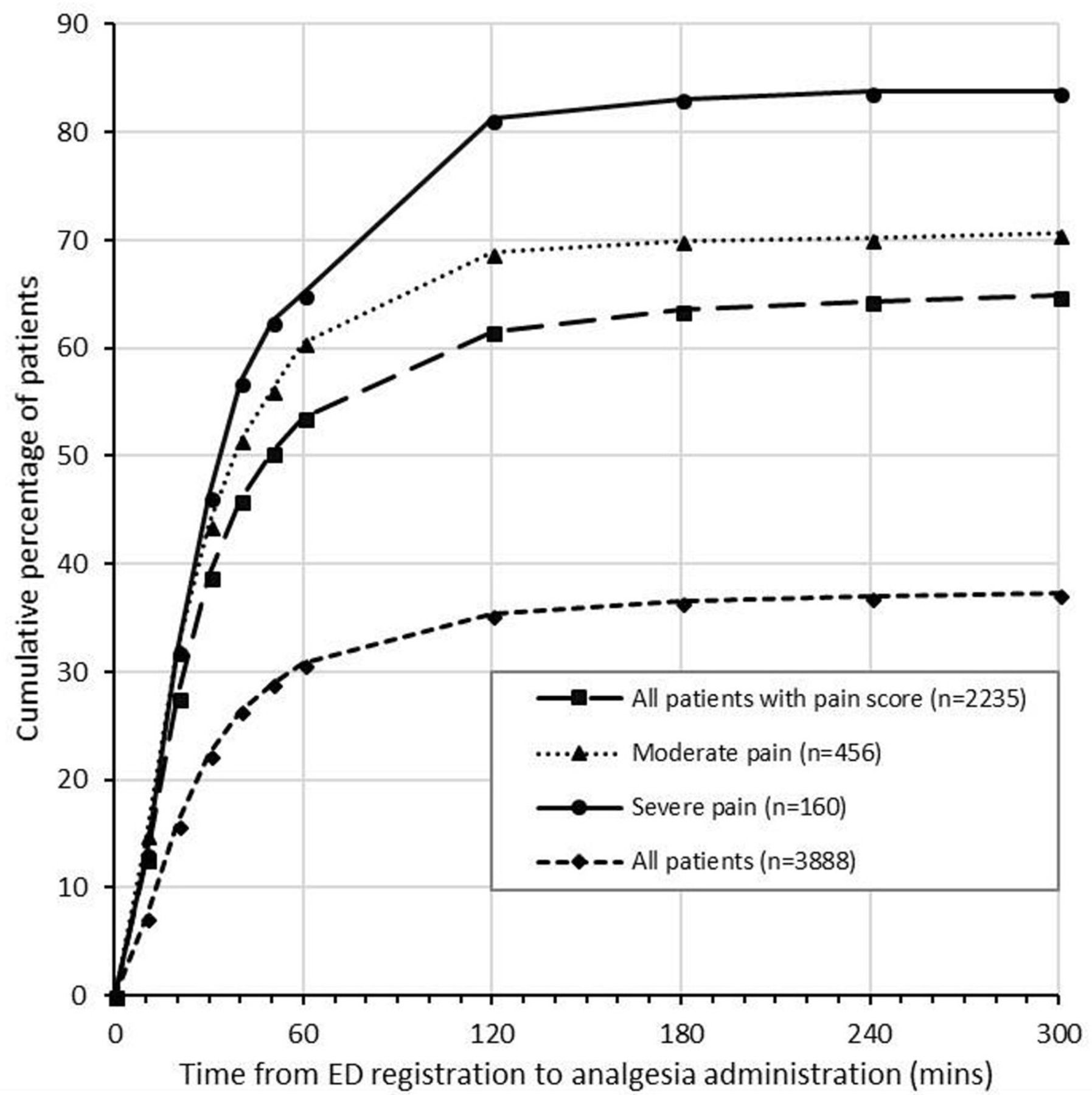
{kind=link}
Relationship between analgesia administration and time in all patients and patients with moderate and severe pain. ED, emergency department.
Time to first analgesia, including subgroup analyses of those with moderate (n=456) and severe (n=160) pain is shown in figure 1. Only 197 (32%) of the 456 patients with moderate or severe pain received analgesia within 20 min of arrival. Seventeen patients (10.6%) received an opiate as per RCEM guidelines.10
Discussion
We have reported the outcomes of paediatric pain management across the PERUKI network. A pain assessment was documented in under 60% of children with minor injury, re-assessment of pain was almost completely absent, and outcomes were missing in a substantial volume of patients, indicating that pain management and the associated outcomes have not been adequately addressed and prioritised within existing network structures and processes.
For a patient, nothing is as important as finding relief for severe pain,1 and tools exist for measuring (and guiding management of) this pain regardless of age.5 Rates of initial pain assessment ranged widely, half of those presenting in severe pain received intravenous/intranasal opioid, nitrous or ketamine, and only 11% had their pain formally reassessed. Repeat pain scoring occurred more frequently in patients with more severe initial pain and in those who received analgesia, but overall rates were low. This suggests a lack of uniform assertive ED pain management across the network, with the source issue likely to be related to knowledge translation and culture.2 6 A previous PERUKI study identified that training was included in induction/orientation in 24 sites (63%), professional development in 16 sites (42%), and pain/analgesia competencies were mandatory in 15 sites (39%),15 implying that pain education is a low priority for over 50% of responding institutions.
One-third of the patients did not have documentation regarding prehospital analgesia, a rate mirrored in a recent RCEM audit.10 Rates of analgesia administration prior to ED arrival are likely to be genuinely suboptimal, with only one-fifth of patients being treated before arrival in this study. This is particularly the case when children self-present or are brought by parents/carers. A whole system approach for public health strategies to educate and empower parents about their role in appropriate analgesia administration may therefore be beneficial.19 However, further research is required to understand the reasons why rates of analgesia administration is so low in this situation is essential, in order to inform the development of any such resources. In cases where the patient had been previously seen by a healthcare provider (general practitioner, ambulance, walk-in centre or transferred from another ED) the rate of analgesia was 51.5% (n=111/229), in keeping with previous studies in prehospital paediatric analgesia in the UK20 and higher than 26% previously noted in Ireland.21 There is a necessity to further investigate the system wide lack of documentation of prehospital analgesia in 31.9% of cases with severe/moderate pain. The health system network wide strategy must consider pain outcomes when pain management inside and outside the hospital (including at home, by prehospital emergency services and referring institutions) has been sufficiently demonstrated.
Local structures and processes must also be centred on achieving optimal pain outcomes. A recent systematic review which aimed to identify existing quality indicators for assessment and treatment of pain in EDs identified three structure related indicators.22 Our adapted framework included 10 structures, 8 processes and 4 outcomes related to paediatric pain management (online supplemental appendix 2). There is a need for a clear health system network wide strategy, with a person-centred focus, which details out both the structures and processes needed to achieve optimal outcomes.1 Therefore, we recommend further stakeholder consensus on the core structures and processes across the network to best achieve optimal outcomes and this would provide the basis of future improvement.
RCEM has introduced a national quality improvement project for 2021/2022 on ‘Pain in Children’ with data entry commencing October 2021 with the project anticipated to last for a year.23 The results of this project including the benefits and the sustainability of improvements are awaited. We advocate is the introduction of national measures for pain assessment and management similar to the previous national improvements implemented in sepsis management. This would allow comparison between sites and could supports improvements in the quality of services motivated by fiscal incentives. Another avenue which we feel warrants further exploration involves giving ownership of pain reporting and control to families.
We have identified fundamental gaps in structures and processes that have resulted in the suboptimal outcomes. A strength of this study is that we have paired this study to the related structures .15 This study included patients aged from birth to 15 years (prior to their 16th birthday), with a range of nociceptive injuries, allowing for generalisable conclusions about pain practices for almost 4000 paediatric ED patient episodes related to minor injury.
Limitations
The most significant limitation is that this was a retrospective analysis of clinical notes, rather than prospective data capture. This data collection method represents the ‘real world’ collection of data points (or lack thereof) representing the patient journey and would be less prone to the Hawthorne effect. The retrospective nature of the study meant that not all elements of the adapted framework could be analysed and the adapted framework (online supplemental appendix 2) requires further validation. For certain data parameters, there was a relatively large proportion of ‘unknown’ responses, due to lack of documentation by existing structures and processes. It is recognised from clinical audit that documentation, or lack thereof, may not capture actual practice, therefore some results may underestimate or overestimate performance at our EDs. The absence of data is itself a critical finding and a key recommendation for improvement. For example, patients with moderate or severe pain analysis might not include patients who may have received prehospital analgesia shortly before arrival as this was not documented in 31.9% of cases. The retrospective methodology employed also meant that we were limited to assessing analgesia that was documented in chart prescriptions and would not capture analgesia which was offered but was declined. Non-pharmacological methods, such as ice packs, splints and slings, are important modes of pain relief, but lack of routine documentation of these practices meant that we were unable to assess their use across sites. A future prospective study is needed to gain more granular detail into structures, processes and outcomes relating to pain management across the PERUKI network.
The service evaluation was conducted for a single week in the winter, and we have not assessed any seasonal variation in pain processes at times when there are changes in total attendances and changes in relative proportions of injuries compared with illness.
Our approach allowed us to gain an understanding of key variations of the pain assessment and management in sites across the PERUKI network. This study did not obtain information on the clinical record systems used and the qualifications of staff. We did not evaluate patient, parental or healthcare worker satisfaction, which are all key outcome measures. This limits the ability to fully evaluate the outcomes of paediatric pain management across the PERUKI network. However, this outcome was not feasible owing to its retrospective design.
Conclusions
To advance improvements in paediatric pain management more research is required to determine the core structures and processes that contribute to optimal outcomes. We recommend that the effectiveness and feasibility of each recommendation is considered. Structures and processes across the network do not support optimal outcomes.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Full ethical approval was deemed not to be required for this service evaluation, following assessment against the Health Research Authority framework by the Research and Innovation department in the lead site (Birmingham Children’s Hospital).
Acknowledgments
The following acted as site leads for this study and were responsible for data collection: M Anderson, Great North Children’s Hospital, Newcastle; A Appelboam, Royal Devon and Exeter Hospital, Exeter; M J Barrett, Children’s Health Ireland at Crumlin, Dublin; T Bolger, Children’s Health Ireland at Tallaght, Dublin; A Boyle, Addenbrooke’s Hospital, Cambridge; F Cleugh, St Mary’s Hospital, London; A Cowton, County Durham & Darlington NHS Foundation Trust; C Deasy, Cork University Hospital, Cork; J Evans, Sheffield Children’s NHS Foundation Trust, Sheffield; S Gardner, Ormskirk & District General Hospital, Ormskirk; C Gough, Nottingham Children’s Hospital, Nottingham; D Hall, Evelina Hospital, London; S Hall, Queen Elizabeth Hospital, Woolwich; S Hartshorn, Birmingham Children’s Hospital, Birmingham; H Jarman, St George’s Hospital, London; G Johnson, Royal Derby Hospital, Derby; J Maney, Royal Belfast Hospital for Sick Children, Belfast; S Messahel, Alder Hey Hospital, Liverpool; S Prudhoe, City Hospitals Sunderland Foundation Trust, Sunderland; M Nyirenda, Lewisham and Greenwich NHS Trust, London; G Patton, Royal Aberdeen Children’s Hospital, Aberdeen; K Potier, Royal Manchester Children’s Hospital, Manchester; Z Roberts, Children’s Hospital for Wales, Cardiff; D Roland, University Hospitals Leicester NHS Trust, Leicester; F Sa'adedin, King’s College Hospital, London; A Scott, James Cook University Hospital, Middlesbrough; A Smith, Bristol Royal Hospital for Children, Bristol; J Smith, Derriford Hospital, Plymouth; E Walton, Royal Alexandra Children’s Hospital, Brighton; A Wedgewood, Royal United Hospital, Bath; S Wong, Royal Free London NHS Foundation Trust, London; We would also like to thank Aidan Beegan, Biostatistician at the National Children’s Research Centre for his statistical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @stuarthartshorn, @mdlyttle
Collaborators PERUKI site leads for the study: M Anderson, Great North Children’s Hospital, Newcastle; A Appelboam, Royal Devon and Exeter Hospital, Exeter; M J Barrett, Children’s Health Ireland at Crumlin, Dublin; T Bolger, Children’s Health Ireland at Tallaght, Dublin; A Boyle, Addenbrooke’s Hospital, Cambridge; F Cleugh, St Mary’s Hospital, London; A Cowton, County Durham & Darlington NHS Foundation Trust; C Deasy, Cork University Hospital, Cork; J Evans, Sheffield Children’s NHS Foundation Trust, Sheffield; S Gardner, Ormskirk & District General Hospital, Ormskirk; C Gough, Nottingham Children’s Hospital, Nottingham; D Hall, Evelina Hospital, London; S Hall, Queen Elizabeth Hospital, Woolwich; S Hartshorn, Birmingham Children’s Hospital, Birmingham; H Jarman, St George’s Hospital, London; G Johnson, Royal Derby Hospital, Derby; J Maney, Royal Belfast Hospital for Sick Children, Belfast; S Messahel, Alder Hey Hospital, Liverpool; S Prudhoe, City Hospitals Sunderland Foundation Trust, Sunderland; M Nyirenda, Lewisham and Greenwich NHS Trust, London; G Patton, Royal Aberdeen Children’s Hospital, Aberdeen; K Potier, Royal Manchester Children’s Hospital, Manchester; Z Roberts, Children’s Hospital for Wales, Cardiff; D Roland, University Hospitals Leicester NHS Trust, Leicester; F Sa'adedin, King’s College Hospital, London; A Scott, James Cook University Hospital, Middlesbrough; A Smith, Bristol Royal Hospital for Children, Bristol; J Smith, Derriford Hospital, Plymouth; E Walton, Royal Alexandra Children’s Hospital, Brighton; A Wedgewood, Royal United Hospital, Bath; S Wong, Royal Free London NHS Foundation Trust, London
Contributors SH, MB, SD and ML contributed to the study design. SH and SD were involved in the data analysis. All authors contributed to the study implementation/data acquisition, manuscript preparation and revisions. SH is the guarantor for the study content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.