Article Text

Abstract
Although radioactivity is released routinely at every stage of nuclear power generation, the regulation of these releases has never taken into account those potentially most sensitive—women, especially when pregnant, and children. From uranium mining and milling, to fuel manufacture, electricity generation and radioactive waste management, children in frontline and Indigenous communities can be disproportionately harmed due to often increased sensitivity of developing systems to toxic exposures, the lack of resources and racial and class discrimination. The reasons for the greater susceptibility of women and children to harm from radiation exposure is not fully understood. Regulatory practices, particularly in the establishment of protective exposure standards, have failed to take this difference into account. Anecdotal evidence within communities around nuclear facilities suggests an association between radiation exposure and increases in birth defects, miscarriages and childhood cancers. A significant number of academic studies tend to ascribe causality to other factors related to diet and lifestyle and dismiss these health indicators as statistically insignificant. In the case of a major release of radiation due to a serious nuclear accident, children are again on the frontlines, with a noted susceptibility to thyroid cancer, which has been found in significant numbers among children exposed both by the 1986 Chornobyl nuclear accident in Ukraine and the 2011 Fukushima-Daiichi nuclear disaster in Japan. The response among authorities in Japan is to blame increased testing or to reduce testing. More independent studies are needed focused on children, especially those in vulnerable frontline and Indigenous communities. In conducting such studies, greater consideration must be applied to culturally significant traditions and habits in these communities.
- Epidemiology
- Ethics
- Genetics
- Toxicology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Radioactivity is released at every stage of nuclear power production, from uranium mining to electricity generation to radioactive waste production. In some of these phases, toxic heavy metals are also released into the environment.
Children, women and particularly pregnant women living near nuclear production facilities appear to be at disproportionately higher risk of harm from exposure to these releases. Children in poorer often Non-White and Indigenous communities with fewer resources and reduced access to healthcare are even more vulnerable—an impact compounded by discrimination, socioeconomic and cultural factors.
Nevertheless, pregnancy, children and women are underprotected by current regulatory standards that are based on ‘allowable’ or ‘permissible’ doses for a ‘Reference Man’. Early in the nuclear weapons era, a ‘permissible dose’ was more aptly recognised as an ‘acceptable injury limit,’ but that language has since been sanitised.1 Permissible does not mean safe. Reference Man is defined as ‘…a nuclear industry worker 20–30 years of age, [who] weighs 70 kg (154 pounds), is 170 cm (67 inches) tall…is a Caucasian and is a Western European or North American in habitat and custom’.2
Very early research conducted in the USA in 1945 and 1946 indicated higher susceptibility of pregnancy to radiation exposure. Pregnant dogs injected with radiostrontium had defects in their offspring and yet, complete results of these studies were not made public until 1969.3
By 1960 however, U.S. experts were clearly aware that research indicated higher susceptibility of children, when the Federal Radiation Council (FRC) (established in 1959 by President Eisenhower) briefly considered a definition for ‘Standard Child’—which they subsequently abandoned in favour of maintaining a Standard Man definition,1 later renamed Reference Man. The 1960 report also recognised hormones as a radiation ‘co-carcinogen’, which evokes later research indicating that radiation impacts the oestrogenic pathway, although the mechanism is not understood and has been poorly investigated.4
And while the current U.S. Environmental Protection Agency (EPA) toxic exposure guidance recognises an enhanced early lifecycle susceptibility to a number of mutagens,5 recommending a risk factor increase of 10 after birth and before the age of two for some of these toxics,6 radiation exposure standards are still based on Reference Man.
Differing impacts based on gender occur for a range of chemicals and various exposure scenarios. In some cases, males are more susceptible than females, while the reverse is also seen.7 For ionising radiation in particular, data from the survivors of the atomic bombings in Japan show ‘women from the same age-at-exposure cohort (26–30 years) suffered 50% more cancer…compared to the males’.8 The latest data from the atomic bombing survivor cohorts in Japan associate radiation exposure in utero with solid cancer mortality for adult females, but not males.9
Since female cumulative baseline rates for most cancer types are lower than male,10 11 exposure to radiation may be erasing a woman’s potential natural cancer resistance, while also increasing her risk relative to a man’s. However, not enough research has been done in this area to be sure.
Current U.S. regulations allow a radiation dose to the public (100 mrem per year) which poses a lifetime cancer risk to the Reference Man model of 1 person in 143. This is despite the EPA’s acceptable risk range for lifetime cancer risk from toxics being 1 person in 1 million to 1 person in 10 000.12 As noted by the EPA, this gives radiation a ‘privileged pollutant’ status.13 Additionally, biokinetic models for radioisotopes are not sex-specific. A male model is still used for females. The models are also not fully age-dependent.14 Radiation damage models also fail to account for a whole host of childhood and pregnancy damage.1
There are known ‘windows of susceptibility’ in a lifetime, ‘includ[ing] periods of active cell differentiation and growth in the womb and in early childhood as well as adolescence, when the brain is continuing to develop’ during which ‘[c]hemicals can act like hormones and drugs to disrupt the control of development and function at very low doses…[i]n some cases, a susceptibility to disease also can persist long after the initial insult or exposure has ended’.15
Women and children in underserved communities are at still greater risk because of unique exposure pathways and systemic inequities. Traditional lifestyle and cultural patterns can also lead to increases in exposure. In the case of some Native Americans, exposure to toxics and radiation has been multigenerational, enduring over a period of 150 years.16
In an exploration of the studies, we find a notable lack of in-depth, independent research looking specifically at children as well as the wider population in Indigenous or minority communities. Uncertainties caused by this lack of study are used by officials to underprotect those most at risk.
We also find a marked contrast between the conclusions of some of the studies and the anecdotal evidence on the ground.
Most of the primary research that has focused on the susceptibilities of women and children has consistently indicated disproportionate impacts, even among those possibly exposed to lower radiation doses. Impacts can include increases in childhood cancers, particularly leukaemia and central nervous system cancers,17 neurological disorders, respiratory difficulties, cardiovascular dysfunction, immune dysfunction, perinatal mortality18 and birth defects.19 20 Rapid cell division is among the development processes thought to account for some of this susceptibility.
However, many studies are unable to link these adverse outcomes to radioactivity because the studies’ authors tend to use several faulty assumptions:
‘doses will be too low to create an effect’—a beginning assumption ensuring poor hypothesis formation and study design.21 Therefore, when an effect is found, radioactivity has been predetermined not to have an association with the effect. This exclusion often leads to an inability to find an alternate associated disease agent;
‘small negative findings matter’—In fact, what matters are positive findings or very large negative findings;22
‘statistical non-significance means a lack of association between radiation exposure and disease’ — a usage a number of scientists in various disciplines now call ‘ludicrous’23;
‘potential bias or confounding factors are reasons to dismiss low dose studies’—In fact, when assessing low dose impacts, researchers should take care not to dismiss studies with these issues and researchers should minimise use of quality score ranking.24
Consequently, we examine and reference studies even if they contain such faulty assumptions because they still indicate increases in certain diseases, such as some leukaemias, known to be caused by radiation exposure. Additionally, few alternative explanations were offered in the conclusions of these studies, meaning radiation exposure might still have been the cause.
Uranium mining and racial discrimination
Uranium mining contributes significantly to the wide dispersal of radioactive waste streams into the air, water and soil. Uranium mining also leaves behind a massive debris field of discarded radioactive residues, rocks and heavy metals, known as tailings.
Heavy metals are also released by uranium mining and these can be as toxic, if not more so, than the radioactive elements. The 1960 FRC report recognised radiation as a cocarcinogen with hormones and viruses and chemicals, indicating synergistic impacts that have rarely been investigated. One study looking at medical impacts of the 1986 Chornobyl nuclear power plant disaster in Ukraine found that multiple congenital malformations were much higher in areas of combined contamination, suggesting an additive and potentially synergistic effect between radioactive and chemical pollutants.20
In the USA, Native American communities have constituted the majority of the uranium mining workforce. In the American Southwest, Navajo Nation community members have experienced increases in a number of diseases,25 26 and lingering internal contamination from uranium mine waste among neonates and children.27 28 Native Americans also present with chronic ailments—such as kidney disease and hypertension—linked with living near and contact with uranium mine waste.
Additionally, comparing uranium mining health data from one race to another should be done with caution as ‘[t]he increased toxicity [of mining exposure] to Native miners underscores the potential for unique sensitivities to toxicants within the Native community as compared with all races results, questioning the derivation of standards on the basis of data collected from other populations’.28
It is also worth noting that some Native American communities are living with a 150-year health legacy of potential exposure to radioactive and heavy metal mine waste. Research on humans,20 and additional studies on radioactivity and animals,29 30 indicate that legacy exposures such as these result in a cumulative impact over generations and can leave descendants of a community more susceptible to damage from future exposures than their parents were.31
An examination of Navajo babies born between 1964 and 1981 showed that congenital anomalies, developmental disorders and other adverse birth outcomes were associated with the mother living near uranium mines and wastes.32 The results of this study, published in 1992, were not followed up until 2010 with the establishment of the Navajo Birth Cohort study, a community-based and community-driven initiative that examines the impact of chronic exposure to mine wastes on birth outcomes.28
Historic and recent official research has, on the whole, been systemically racist by failing to account for culturally-specific exposure scenarios to Navajo. These include frequent contact with contaminated lands, waters and, in some cases, a nearly 100% reliance on locally grown and sourced foods,28 ,33 as well as failure to consider doses to Navajo Nation community members from the Trinity explosion—the first detonation of an atomic device.34 Some research teams have attempted to address systemic racism by partnering with local community members and integrating local knowledge.33
In Jadugoda, India, where six uranium mines operate, the first opening in 1957, those affected are Indigenous peoples from the Santhal, Munda and Ho tribes. A local organisation, Jharkhandi Organisation Against Radiation, has been documenting strange health anomalies in the community for years, including deformities and birth defects.
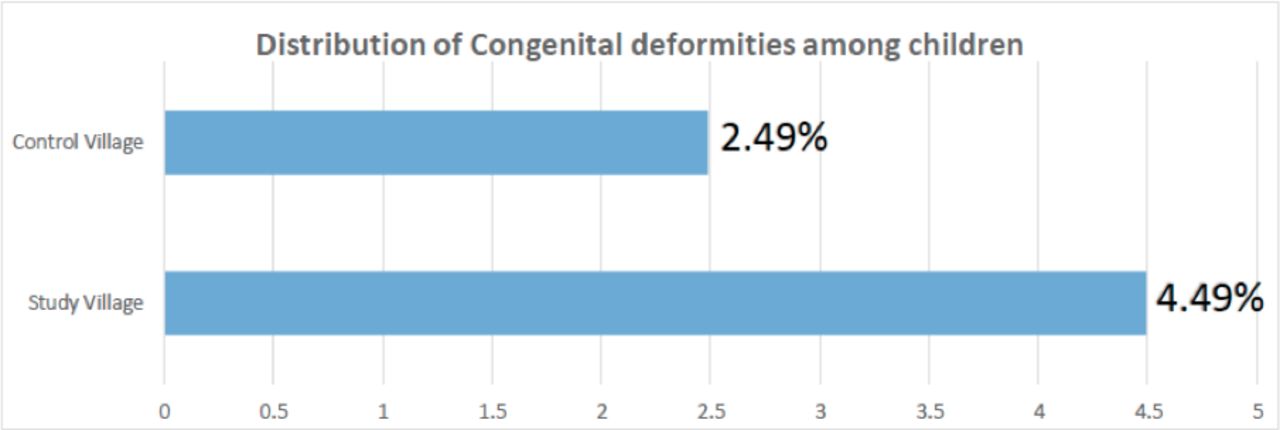
Their observations were supported by an independent study of the Jadugoda community, conducted in 2007 by Indian Doctors for Peace and Development, which found that the offspring of mothers living near uranium mining operations showed a significant increase in congenital deformities (4.49% vs 2.49%) (figure 1).
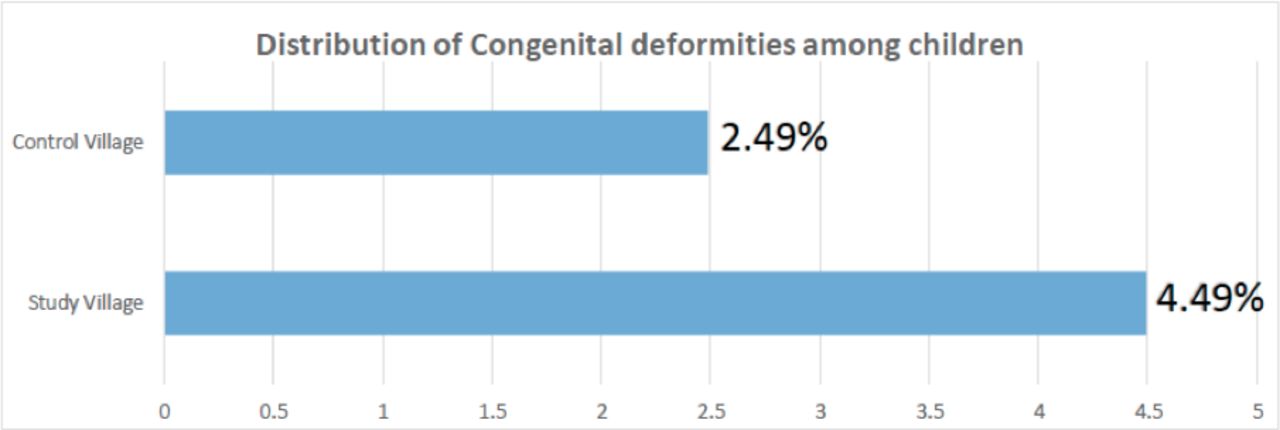
Congenital deformities among babies from mothers who lived near the Jadugoda uranium mining operations.
In addition to deformities, deaths were higher. Among mothers who lost their children after birth, 9.25% of mothers in the study villages reported congenital deformities as the cause of death of their children as compared with only 1.70% of mothers in the reference villages.
The authors concluded that the finding of the study confirms the hypotheses that the health of Indigenous people around uranium mining is more vulnerable to certain health problems.35
However, other studies contradict these conclusions. A 2013 study,36 concluded that the water was safe for people to drink. And, a study by scientists from India’s Bhabha Atomic Research Centre37 came to a similar conclusion. However, these studies are deficient in many ways, limiting their research to dose reconstruction rather than health outcomes and failing to consider inhalation or ingestion of radionuclides, other than from drinking water. Furthermore, the association with the Atomic Research Centre raises questions about conflict of interest.
People living in the town of Arlit in Niger, and those working in the huge majority French-owned uranium mine nearby, are exposed on a daily basis to levels of radioactivity higher than those found in the Chornobyl exclusion zone. Independent studies in Arlit,38 beginning in 2003, found radioactively contaminated metals discarded from the mine routinely used in households, where children were exposed.
An independent study commissioned by the European Parliament and published in 2010, looked at health and environmental legacy conditions around uranium mines in both Gabon and Niger and found, in the case of Niger, that waste dumps and related processing facilities posed a severe environmental and health hazard to the local population. It also found evidence of radioactive contamination of local water supplies, and contaminated dust, and that contaminated construction materials had been sold in markets and used to build dwellings in local towns.39 However, despite observations of the risks from multiple scientific sources, there is a paucity of actual health studies. The health outcomes are largely recorded anecdotally, by activists on the ground such as the Arlit-based NGO, Aghirin’ Man.40
In Australia, uranium contaminates drinking water around uranium mine sites at rates far higher than recommended. Aboriginal communities, most likely to inhabit land around these facilities, suffer from increases in cancers and stillbirths according to the findings described below.
A 2019 Australian government study found increases in low birth weight, fetal death and cancers, but a ‘lack of evidence’ that radiation was the cause, suggesting that alcohol and tobacco use, and a high-fat diet, could explain the increase in diseases.41 Radiation, which could have been a responsible agent, was eliminated because the researchers considered that the doses were too low to explain the remaining disease increases not attributable to non-radiation exposure factors. This was despite the known connection between radiation exposure and low birth weight and cancers. This conclusion left the community with unexplained disease increases, a pattern seen all too often in radiation health studies.
In her analysis, Rosalie Schultz states that ‘We owe it to Aboriginal people living near mines to understand and overcome what’s making them sick’,42 and further points out that ‘Development of the Ranger mine entailed nullification of veto rights, disempowering Aboriginal communities and threatening their livelihoods. With mining came royalty money, expensive commodities, money‐hunger and alcohol’.
These examples serve to highlight the tension between the often strong anecdotal evidence and the common failure to attribute the causal factor to a potential exposure source already linked to the outcome of interest in other populations.
Routine radioactive releases from nuclear power plants
Nuclear power plants routinely release radioactivity as part of daily operation. In 2008, a landmark case-control study was published in Germany,43 known as the KiKK study.
It revealed an unsettling 1.6-fold increase in all cancers and a 2.2-fold increase in leukaemias among children under 5 years old living within 5 km of operating nuclear power plants.
In general, the incidences were higher the closer the children lived to the nuclear plant. The KiKK findings were backed up by other studies44 and a meta-analysis.45
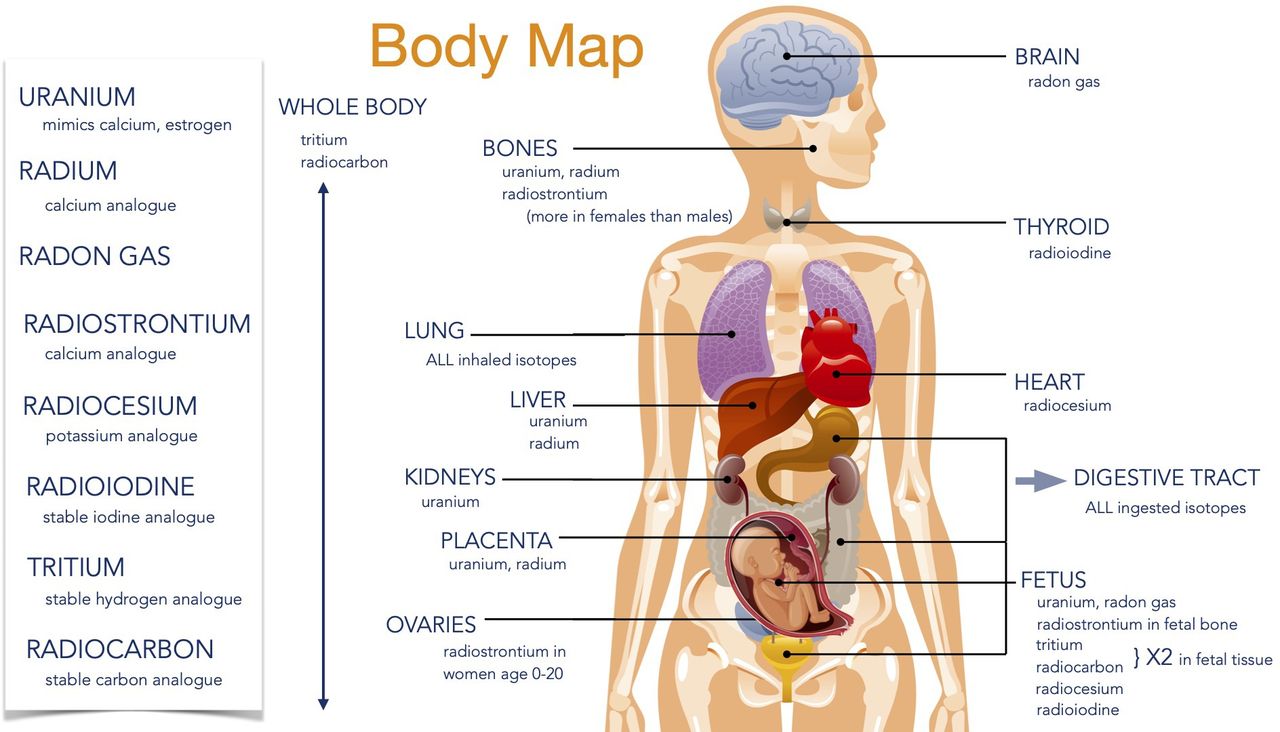
However, the authors concluded that their findings were ‘unexplainable’ because the doses were assumed to be too low to cause cancer. But UK radiation researcher, Dr. Ian Fairlie, hypothesises that sudden large spikes in radiation releases during reactor refuelling resulted in higher doses. These could account for higher rates of leukaemia among children.46 Fairlie further posits that the observed high rates of infant leukaemias may be a teratogenic effect from radionuclides, particularly tritium, incorporated during pregnancy (figure 2).47
{kind=link}
{kind=link}
Selected radioisotopes: where they travel and primarily collect in the body.
Other studies of natural and manmade background radiation associate childhood cancers with doses that are much lower than these spikes, but delivered continuously.17 48 Taken together, these studies indicate that unique sensitivity to adverse effects of radiation exposure exists during pregnancy.
Catastrophic radioactive waste releases
There have been at least three catastrophic releases of radioactivity from civilian nuclear reactors due to meltdowns: the 1979 Three Mile Island (TMI) disaster in the USA; the 1986 Chornobyl disaster in Ukraine and the 2011 Fukushima, Japan nuclear disaster.
During the TMI crisis, there were 24 spontaneous abortions or stillbirths among pregnant women who were living within five miles of the nuclear facility and in their first 4 months of pregnancy. The expected number should be closer to 12. The researchers of a study examining this posit that this may be due to stress (measured by number of evacuation days), but live births had equivalent evacuation days to abortions or stillbirths.49
Radiation from the TMI catastrophe was also associated with childhood leukaemia, although the study found only a small number of cases. Interestingly, the study authors note an association with radiation exposure and all childhood cancers was also present before the catastrophe, although with wide confidence intervals. The authors recognise this increase, particularly leukaemia, as compatible with increases reported near some other nuclear installations, but eliminated radiation as a likely cause because the exposures were low.50 Yet, the authors cite seven additional studies that found this effect. An alternative explanation has yet to be revealed even as more recent studies have indicated increases of childhood leukaemias around operating nuclear facilities and in levels of higher background radiation (see above).
Outcomes in the Former Soviet States (FSS) from initial exposure to Chornobyl radioactive fallout include thyroid cancers (predominantly among those exposed during childhood) and significant increases in leukaemia among children who were in utero or who were under 6 years of age at the time of the Chornobyl catastrophe.51 Also found were increases in radiation-induced organic mental disorders.52
Among those continuing to live in Chornobyl-contaminated areas in the FSS, we see increases in cardiovascular disorders,53 54 decreased lung function,55 56 defects of the lens of the eye57 and significantly increased rates of conjoined twins, teratomas, neural tube defects, microcephaly and microphthalmia.19 Further, research indicates significantly higher birth defects—some de novo—in the Chornobyl-contaminated Bryansk region. Projections indicate that certain birth defects will increase in the next few years.20
The Chornobyl disaster produced a phenomenon known as ‘Chornobyl heart’, where children were born with multiple heart defects—now being observed among children exposed as a result of the Fukushima catastrophe.58 Some of these impacts occur at low, chronic doses.
Outside of the FSS, children born in regions of Sweden with higher Chornobyl fallout performed worse in secondary school—particularly in maths—and had more behavioural problems.59 Similarly, in Norway, in utero exposure to Chornobyl radiation is associated with significantly lower verbal IQ, verbal working memory and executive functioning.60 61
In Central Europe, studies observed a statistically significant increase in childhood leukaemias.62 Perinatal mortality increased in European and FSS countries after the Chornobyl catastrophe, and increases in trisomy 21 were found in Berlin and Belarus in 1987/1988. The cases coincided with exposure to Chornobyl fallout.63 64
Perinatal mortality rates increased significantly in Fukushima and six neighbouring prefectures after the Fukushima nuclear disaster began, although researchers debate the magnitude of the increase and further study is needed to associate increases with radiation from the catastrophe.65 66
After Fukushima, the International Commission on Radiological Protection made public its report encouraging the growing and eating of contaminated food to protect economic interests, while they also made recommendations for how much radiation people should be exposed to.67 Yet, their models do not fully account for being a child, female or pregnant.
Thyroid cancers among those exposed to Fukushima radiation as children have increased 20 times the expected rate, with about 80% metastasizing68—indicating increased severity of the cancer and suggesting screening and surgery was necessary.
Despite this, SHAMISEN, a project funded by the European Commission, has recommended against systematic thyroid screening after nuclear catastrophes, claiming over-diagnosis and psychosocial impact can result.69
Although it is correct that in some countries apparently high levels of undiagnosed thyroid anomalies exist without clinical symptoms, banning thyroid screening altogether after nuclear disasters such as Fukushima denies those exposed the essential medical treatment that could catch aggressive cancers early.
The suggestion that medical examinations are psychologically scarring has sometimes been proffered as a justification for avoiding looking for health impacts from radiation exposure after a nuclear accident.70 Fewer tests have led to fewer findings in some of the more recent studies.
Some advocates of reduced screening point to studies from South Korea that blame an ‘epidemic’ of thyroid cancers on increased screening. But data from Japan should not be compared with data from the South Korean study because the latter study excluded participants younger than 20 years, with only 2% in the 20–29 age range.71 Conversely, the Fukushima health management survey (FHMS) is examining those who were under 18 years of age at exposure.72
Researchers also claim that any increasing thyroid cancer incidence rates in Japan are not due to radiation exposure because the age pattern of thyroid cancers arising in Japan after Fukushima differs from that arising after Chornobyl in the former USSR countries.73
Five years after the Chornobyl disaster began, Belarus data indeed show a large increase in thyroid cancer diagnoses in those aged 0–4 at time of exposure (AE),74 unlike the Fukushima data. However, the pattern in Ukraine and Russia is similar to the Fukushima data, which show increasing disease among younger age groups as more years pass. Ukraine and Russia, as with the Fukushima data, only demonstrated a high thyroid cancer incidence in age group 0–4 AE beginning 12 years after the disaster,75 with this increase beginning in Ukraine about 8 years later.76 This effect is indicated despite smaller overall subject participation numbers in the FMU study (40% decrease since the programme began), possibly due in part to pressure to opt out of FHMS thyroid screening.77
Comparisons between the Chornobyl data sets (which differ even between the FSS) and Fukushima data should consider, in particular, the various exposure rates. For instance, the health data indicate that rates differed substantially between Belarus (high rates) and Ukraine and Russia (lower rates).
In addition, research found an excess of thyroid cancer that is unlikely to be explained by an increase in screening.78 This conclusion is supported by a study published very recently that linked external radiation doses linearly to increases in thyroid cancers.75 Coupled with these dose findings, thyroid cancer metastasis, aggressive growth and recurrence, it seems enhanced screenings are entirely appropriate as many of these cancers are clinically relevant.79
Reprocessing: the dirty end of the nuclear fuel chain
Reprocessing—the cutting up of irradiated reactor fuel rods in a chemical bath to extract plutonium and fissile uranium—involves the annual discharge of tens of millions of gallons of radioactively contaminated liquids and the release of radioactive gases such as krypton, xenon and carbon-14.80
A 1990 UK study of the Sellafield reprocessing facility found higher incidences of leukaemia, particularly non-Hodgkin’s lymphoma, among children near the site.81 It concluded that this might be associated with the fathers working at the plant and external doses of whole body penetrating radiation before conception. This would explain statistically the observed geographical excess. The study suggested that one effect of ionising radiation on the fathers could in turn be leukaemogenic in their offspring.
There have been challenges to this hypothesis and also challenges to those studies that contradict his paper. Gardner’s most notable opponent was the epidemiologist, Doll,82 who testified on behalf of Sellafield owners, British Nuclear Fuels, Limited, in a 1994 court case won by BNFL challenging Gardner’s paternal occupational exposure conclusion.
Kinlen, since the early 1990s the lead proponent of population mixing and a viral cause,83 continues to uphold this theory, as do others, including Draper et al,84 who viewed the observed associations as potentially chance findings or possibly other infectious sources. Kinlen, however, concedes that such a virus has not been specifically identified.
Other research has rejected the Kinlen hypothesis, including an investigation by Dickinson et al,85 who concluded that ‘Children of radiation workers had a higher risk of leukaemia/non-Hodgkin’s lymphoma than other children [rate ratio (RR)=1.9, 95% confidence interval (CI) 1.0 to 3.1, p=0.05]’. The researchers used a cohort rather than a case-control design, with wider temporal and geographic boundaries, and confirmed the statistical association between father’s preconceptional irradiation and child’s risk of leukaemia/non-Hodgkin’s lymphoma, and concluded that paternal preconceptional irradiation could be a possible risk factor for leukaemia and/or non-Hodgkin’s lymphoma, and that such outcomes might be found beyond the local worker town of Seascale.
Law et al, also dismissed the population mixing hypothesis.86 His work discovered increased risks of acute lymphoblastic leukaemias in areas with few outsiders or migrants as well as for non-Hodgkin’s lymphoma in areas with low numbers of child migrants. Law concluded that his findings therefore do not support the Kinlen population mixing hypothesis.
A 1993 study similarly found elevated rates of childhood leukaemia around the La Hague reprocessing site in France.87 A second paper the following year had similar findings.88
The main by-product of nuclear power: radioactive waste
The selection of a deep geological repository—the option favoured by most nuclear countries for the management of irradiated reactor fuel—involves ethical as well as scientific challenges.
In the USA, the selection of the now abandoned Yucca Mountain high-level radioactive waste repository site in Nevada violated the treaty rights of the Western Shoshone on whose tribal land it is located. It also ignored the inevitable contamination of groundwater sources beneath the mountain, which would subsequently harm tribal and agricultural populations downstream.89
The Western Shoshone are particularly acutely attuned to the risks of radiation exposure, having lived downwind of the Nevada atomic test site, making them, as Ian Zabarte, Principle Man of the Western Bands of the Shoshone Nation of Indians, describes it, ‘the most bombed nation on Earth’. Further, in addition to the harm to health, Western Shoshone culture believes that ‘rocks, water, plants and animals matter as much as people do’. Western Shoshone elder, Pauline Esteves describes it this way: ‘I believe the land and everything that lives on it are there to do good, not for radioactive materials’.
By mischaracterising the Yucca Mountain site as a remote and uninhabited desert, the U.S. government discriminated against a culture and heritage stewarded by the Western Shoshone, whose experiences dealing with radioactive exposures, like those of other Indigenous and minority communities of colour, cannot be equated to the guidelines of Reference Man.
The USA has now turned to ‘Consolidated Interim Storage’ for the ‘temporary’ accommodation of high-level radioactive reactor waste, identifying two largely Hispanic communities in Texas and New Mexico as host sites.90 The approval process, which was not voluntary, has been challenged in court. However, given their increased sensitivity, any disposal of radioactive wastes in such parking lot-style facilities will put children in the host community at heightened risk of harm.
Elsewhere, the search for a radioactive waste management plan continues, with only Finland currently building a deep geological repository. The question about harm to future generations remains unresolved, given the challenge of identifying the lethality of the repository contents to populations potentially a hundred thousand years or more into the future.
Conclusion
Despite the numerous observations globally, linking radiation exposures to increased risks for children, pregnant and non-pregnant women and the well-demonstrated sensitivity to other toxicants during these life stages, exposure standards in the USA remain based on a Reference Man—a model that does not fully account for sex and age differences.
In addition, faulty research assumptions, unique exposure pathways, systemic inequities and legacy exposures to both heavy metals and radioactivity from mining wastes add to the risks for women and children, especially those in underserved communities. Socioeconomic factors that drive higher deprivation of services in non-homogenous low-income communities of colour also put non-White children at higher risk of negative health outcomes when exposed to radioactive releases, than their White counterparts.
A first and essential step is to acknowledge the connection between radiation, heavy metal and chemical exposures from industries and the negative health impacts observed among children, so that early diagnosis and treatment can be provided. Measures should then be taken to protect communities from further exposures, including a prompt phaseout of nuclear power and its supporting industries.
Studies are also urgently needed where there are none, and the findings of independent doctors, scientists and laboratories should be given equal attention and credence as those conducted by industry or government-controlled bodies, whose vested and policy interests could compromise both their methodologies and conclusions.
Finally, in the face of uncertainty, particularly at lower and chronic radiation doses, precaution is paramount. This means listening to, and taking seriously, the evidence provided by those living close to operating or closed nuclear facilities, rather than dismissing their fears by using faulty research assumptions and uncertainties in the science to deny health impacts and prevent protective and corrective actions.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors Cindy Folkers, co-author, was the principal author of sections addressing the historical inequities in radiation damage assessments and inadequacies of current research. She was also lead author on sections regarding the impacts of uranium mines in the USA, and the health impacts of routine and catastrophic radioactive releases. She contributed to the introduction and conclusion, made editorial revisions to all sections of the article and approved the final version for publication. Linda Pentz Gunter, co-author, contributed to the research, outline and content of this article. She was lead author on the sections dealing with the impacts of non-US uranium mines, reprocessing and radioactive waste, and co-author of the introduction and conclusion. She contributed editorial revisions to all sections of the article and approved the final version for publication. The listed authors are solely responsible for the content of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.