Article Text

Abstract
Background A possible association between child abuse and neglect (CAN) and functional constipation (FC) has been described in adults, however, limited data are available in children. Our objective was to determine the prevalence of suspected CAN in children with FC as compared with their healthy peers.
Methods A case–control study was carried out in children aged 3–10 years. Children with FC were recruited at a tertiary outpatient clinic, and healthy controls were recruited at schools. Parents were asked to fill out questionnaires about the history and behaviour of their child, children were inquired using a semistructured interview about experienced traumatic events and sexual knowledge. The interview was scored by two independent observers. The prevalence of suspected CAN was determined according to the questionnaires and interview.
Results In total, 228 children with FC and 153 healthy controls were included. Both groups were age and gender comparable (50% females, median age 6 years (not significant)). No significant difference in the prevalence of suspected CAN was found between children with FC and healthy controls (23.3% vs 30.1%, 95% CI 0.44 to 1.12, p=0.14), including a suspicion of sexual, emotional and physical abuse.
Conclusion Suspected CAN was detected in both children with FC as in healthy controls. The possible association between CAN and FC in children could not be confirmed.
- child abuse
- gastroenterology
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
A possible association between child abuse and neglect and functional constipation has been described in adults, however, limited data are available in children.
Diagnosing child abuse in young children is extremely challenging, it is often not recognised.
What this study adds?
We found no significant difference regarding the prevalence of suspected child abuse and neglect in young children with functional constipation as compared with healthy controls.
Introduction
Functional constipation (FC) is a common and distressing health condition, affecting around 10% of children worldwide.1 Multiple studies have shown that stressful life events, such as bullying, separation of parents or illness of a family member are associated with functional defecation problems such as FC and faecal incontinence in children.2 3
In adults suffering from functional defecation disorders, such as slow-transit constipation and pelvic floor dyssynergia, a possible association with child abuse has been described.4–10 In addition, abused adult patients reported more severe symptoms of constipation,7 decreased quality of life7 and more frequent use of surgical strategies8 as compared with patients with no history of child abuse. Early detection of abuse is therefore important in the workup of both paediatric and adult patients with FC. This is supported by the current paediatric and adult guidelines, advising to ask for a possible history of abuse in all patients with FC.11 12
Child abuse and neglect (CAN) as defined by WHO includes ‘all types of physical and/or emotional ill treatment, sexual abuse, neglect, negligence and commercial or other exploitation, which results in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power’.13 Different subtypes of CAN have been recognised and include sexual abuse, physical and emotional abuse, and physical and emotional neglect.
The diagnosis of CAN remains challenging, since there is no gold standard and feelings of shame, guilt and blame play an important role in the disclosure of abuse.14 In children, the diagnosis of abuse is even more difficult because of verbal limitations15 and the often absence or non-specificity of physical and psychological symptoms related to CAN.16 17 Several screening tools have therefore been proposed for the paediatric assessment of CAN, using specific signs such as abnormal (sexual) behaviour,18 age-inappropriate (sexual) knowledge15 and abnormalities found on physical examination to detect patients with suspected CAN.
Several pathophysiological mechanisms in adults have been proposed to underlie the association between CAN and FC. Exposure to abuse may result in emotional distress, which in turn, through the brain-gut axis, may lead to visceral hypersensitivity and somatisation generating gastrointestinal symptoms.10 19 In addition, trauma to the anorectal area or abdomen related to abuse may result in withholding behaviour and pelvic floor dysfunction.10 However, the current evidence in adults is also criticised due to methodological shortcomings such as small study populations, the lack of control groups and recall bias.20
Only a few small cohort studies described a possible association between CAN and gastrointestinal symptoms in children, such as FC,21 faecal incontinence22 23 and abdominal pain.24–26 Unfortunately, to date, there is a lack of well-designed studies investigating the prevalence of CAN in children presenting with functional defecation disorders.
Therefore, our objective was to determine the prevalence of suspected CAN in a large cohort of children with FC as compared with their healthy peers using specific signs of CAN.
Methods
A case–control study was carried out between April 2014 and March 2019 including children with FC (index group) and healthy children without gastrointestinal complaints (control group).
Study population
Children aged 3–10 years presenting at our specialised outpatient clinic with FC according to the Rome III criteria27 were included in the index group. Children with signs of organic or surgical causes of their symptoms were excluded.
For the healthy control group, children aged 3–10 years without gastrointestinal symptoms or any other functional or chronic disease were eligible for inclusion and recruited at randomly selected elementary schools throughout the Netherlands. Parents of children were asked about the medical history, current gastrointestinal symptoms and medication use of their child, and children in the control group were excluded if they had any sign of an organic or functional (somatic) disorder.
In both the index and control group, children were excluded if they or their parents had too little knowledge of the Dutch language or if they suffered from a known intellectual disability.
Recruitment and study procedure
An overview of the study recruitment and procedure is depicted in figure 1. For the index group, all parents of newly referred children as patients with FC received an information letter about the study. After their first appointment at the outpatient clinic, parents were verbally informed by the local investigator. After their consent, the physician filled out a questionnaire estimating the risk for CAN using the Child Abuse Risk Evaluation—Dutch version (CARE-NL, and recorded the findings during the physical examination of the child. Next, after the clinic visit, a semi-structured interview (described below) with the child took place at the outpatient clinic by a trained member of the research team. During this interview, the parents were not present in the room. The interview was recorded on video and scored by the interviewer. At a later time point, the videorecorded interview was scored a second time by an independent member of the research team, who was not involved in the preparation of the manuscript. Parents were asked to fill out questionnaires about their child in a separate room.

Overview of study design. *TSCC and RCADS if ≥8 years old. CARE-NL, Child Abuse Risk Evaluation—Dutch version; CSBI, Child Sexual Abuse Inventory; FAP, functional abdominal pain; FC, functional constipation; LEC, Life Events Checklist; RCADS(-P), Revised Child Anxiety and Depression Scale-Parent Version; SKPI, Sexual Knowledge Picture Instrument; TSCC, Trauma Symptom Checklist for Children; TSCYC, Trauma Symptom Checklist for Young Children.
Parents of healthy controls received an information letter about the study in the school newsletter or at school meetings. When interested in participating, parents were asked to send an email to the local investigator. The child was interviewed at school in the same way as the patients were interviewed in the index groups. However, no physical examination was performed as this was considered as too much of a burden in an otherwise healthy child. Parents were asked to fill out the same questionnaires at home.
Questionnaires and interview
The parental questionnaires and interview with children was used to assess the prevalence of suspected CAN. Parents filled out a demographic questionnaire on a possible history of trauma of their child, and the Child Sexual Behaviour Inventory (CSBI-3),28 measuring children’s inappropriate sexual behaviour as a marker for sexual abuse.18 Children were interviewed using the Life Events Checklist (LEC),29 on traumatic events, and the Sexual Knowledge Picture Instrument (SKPI),30 a child-friendly picture book to assess young children’s sexual knowledge. Abnormal reaction to the SKPI included an abnormal non-verbal reaction to the images or age-inappropriate sexual knowledge, which can be indicators of sexual abuse.15
The Revised Child Anxiety and Depression Scale-Parent Version (RCADS/RCADS-P)31 and Trauma Symptom Checklist for Young Children (TSCYC/Trauma Symptom Checklist for Children (TSCC))32 were used to determine psychological symptoms in children with suspected CAN. A demographic questionnaire was filled out by parents to obtain information on social factors and parental characteristics of the child. Detailed description of the questionnaires is available in online supplemental appendix 1.
Supplemental material
Prevalence of suspected can
The prevalence of suspected sexual abuse, physical abuse, neglect and total prevalence of suspected CAN (all subtypes combined) was calculated. Suspected sexual abuse was determined according to one of the following abnormal results; a parent reported child’s history of sexual abuse, a clinical CSBI, an abnormal reaction to the SKPI as scored by two independent observers and/or a child report of sexual abuse on the LEC questionnaire. The prevalence of suspected physical abuse and emotional abuse or neglect was determined according to the following abnormal results; a parent reported child’s history of abuse and/or child report of physical abuse, emotional abuse or neglect on the LEC questionnaire.
Abnormal findings were discussed with a blinded member of our specialised CAN team (SB-K). In case of a strong presumption of CAN and concerns for safety, findings were discussed with the parents and children were referred to our specialised multidisciplinary outpatient clinic (including a specialised paediatrician, child psychologist and social worker) according to the protocol of our hospital.
Study outcomes
Primary outcome was the prevalence of suspected CAN in children with FC as compared with healthy controls. In addition, we aimed to determine clinical characteristics of children with suspected CAN and to determine psychological symptoms in children with suspected CAN.
Statistical analysis
Due to the explorative character of this study and lack of well-designed comparable studies in children, it was not possible to predict the frequency of suspected CAN. Therefore, we were unable to make exact power calculations. The exact prevalence of CAN in young children is unknown. The sample size was therefore calculated based on interim analysis (calculating a prevalence of CAN of 15.7% in children with FC) using nQuery Advisor (Statistical Solutions, Cork, Ireland) as we hypothesised that the prevalence of symptoms of CAN in the index group was twice as high as compared with healthy children. For 80% power to detect an OR of 2.17, 300 children were needed in each group.
Data were stored anonymously in SPSS V.25 (IBM). Statistical significance was accepted at p<0.05. The study groups were compared by using one-way analysis of variance and independent t-test for continuous variables. Analysis of dichotomous variables were performed using χ2 tests or Fisher’s exact tests. Previously reported child and parental risk factors for CAN9 (including age and gender of children, parental education level and mental health problems, parental history of abuse and parental substance abuse) were included.
Patient and public involvement
Patients were involved in the design and conduct of this research. Choice of outcome measures and methods of recruitment were informed by discussions with parents of patients based on previous studies of our research group.15–17 Once the trial has been published, participants will be informed of the results through a newsletter.
Results
Study population
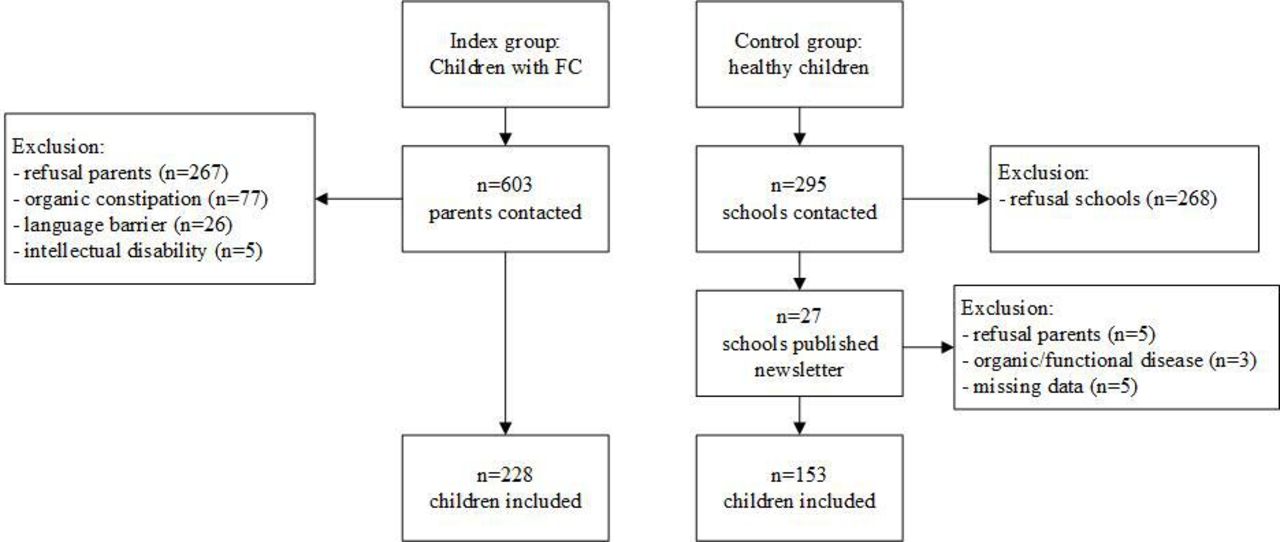
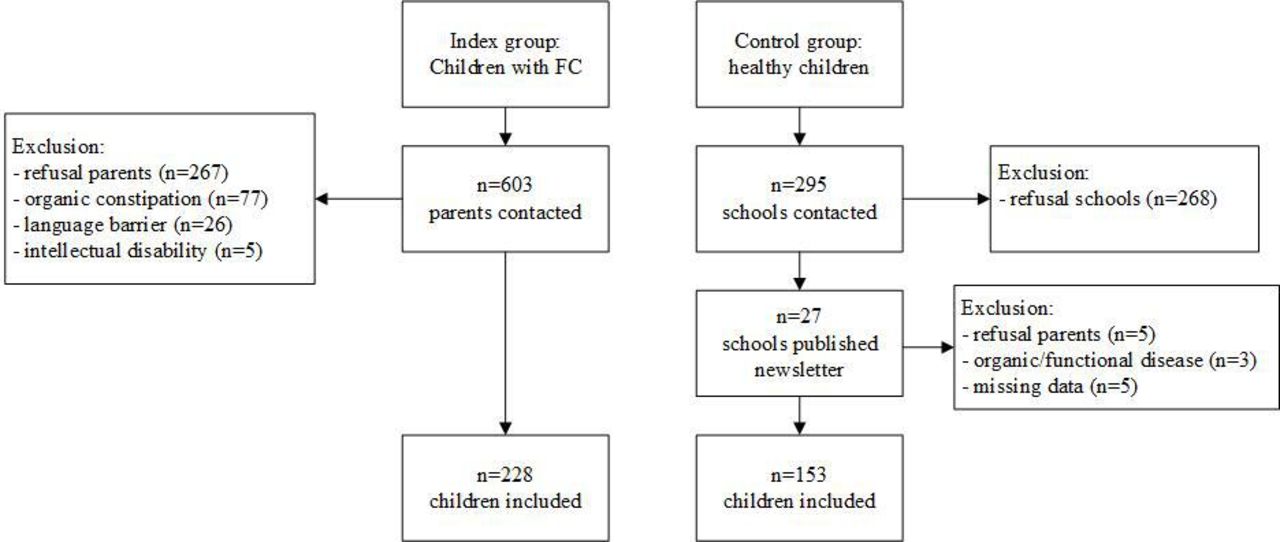
In total, 228 children were diagnosed with FC and included in the index group (figure 2).
{kind=link}
{kind=link}
Inclusion of index and control group. FC, functional constipation.
Reasons to decline participation were mostly practical (eg, no time) or concerns about the implications for the child. For the healthy control group, we randomly selected 295 elementary schools throughout different regions of the Netherlands, out of which 27 schools agreed to publish the study in their newsletter. The majority of schools reported to be already enrolled in other research projects or had hesitations concerning the research topic. In total, 153 parents of healthy children responded and children were included in the control group.
Of the included children, 50.1% were girls and the median age was 6 years (table 1). According to the CARE-NL questionnaire, significant differences with respect to education level and social history between parents of children with FC and parents of healthy controls were found (table 1).
Demographic characteristics
Prevalence of suspected CAN
We calculated the prevalence of suspected different subtypes of CAN (table 2). When combining all subtypes of CAN, no significant difference was found in the prevalence of suspected CAN between children with FC and healthy controls (23.3% vs 30.1%, 95% CI 0.44 to 1.12). Out of the 99 children with a suspicion of CAN, 17 children with FC and 12 healthy controls were referred to our specialised multidisciplinary outpatient clinic for further follow-up.
Prevalence of suspected CAN
Next, our secondary objective was to determine clinical characteristics and psychological symptoms of children with suspected CAN. Clinical characteristics of children with suspected CAN are described in table 3. For this analysis, all children with suspected CAN were grouped together (n=99) and were compared with children without a suspicion of CAN (n=282). In children with FC, no significant difference with respect to the presence of faecal incontinence symptoms was found between children with and without suspected CAN (71.6% vs 74.3%, OR 0.9 95% CI 0.4 to 1.8, p=0.67).
Clinical characteristics of children with suspected CAN
According to the RCADS/RCADS-P and TSCYC/TSCC questionnaires, no significant differences were found in the prevalence of anxiety and depression (3 (3.0%) vs 3 (1.1%), p=0.18) and PTSD symptoms (7 (7.2%) vs 12 (4.7%), p=0.35) between children with (n=99) and without a suspicion of CAN (n=282).
Discussion
In this large case–control study including 381 children, we found a high number (26%) of children with a suspicion of CAN. No significant difference was found in the prevalence of suspected CAN in children with FC as compared with their healthy peers.
Unfortunately, paediatric data on this topic are scarce and the limited published studies mostly report on symptoms of faecal incontinence in children with a confirmed diagnosis of CAN.22 23 With this current study, we tried to determine the prevalence of suspected CAN in children with a confirmed diagnosis of FC. To our knowledge, only two other community based studies conducted in Sri Lanka and Hong Kong assessed this association.21 33 Rajindrajith et al found a significantly higher prevalence of sexual (5.8% vs 2.6%), emotional (40.9% vs 20.8%) and physical abuse (41.6% vs 23.2%) according to self-reports of adolescents with FC as compared with healthy controls.21 In contrast, Tam et al could not confirm this association.33 Since the prevalence of CAN is highly dependent on community and societal factors, and differs between low-income and high-income countries, it is hard to compare our findings with these different widespread geographical locations.13 Moreover, comparison between study results is challenging owing to the difference in instruments used to diagnose the prevalence of CAN.
We found a high prevalence of suspected CAN in our cohort; 23% and 30% of children with FC and healthy controls respectively. These numbers are conflicting with the previous Dutch NPM-2017 study, reporting a prevalence of confirmed cases of CAN of less than 3% in children.34 However, it is important to keep in mind that we could only identify children with a suspicion of CAN, and a final diagnosis by a multidisciplinary team was not made in the time span of our study. This in contrast to the NPM study, which reported on the number of confirmed cases of CAN using data from ‘Safe at Home’ organisations and professionals. This major difference in methods could justify the conflicting numbers. Nonetheless, our results are in line with the previously self-reported prevalence of CAN in Dutch school children of 26.7%.35 36
Research on the exact prevalence of CAN is challenging. Consent of parents is always required, while parents could be the perpetrators of the abuse. Furthermore, the diagnosis of CAN in young children is extremely difficult to confirm, while these young children are most at risk for CAN.13 Not only important emotional barriers in disclosing CAN are involved, especially in a research setting where subjects have not met the interviewer before. In contrast to adults, (young) children often lack the proper words and knowledge to report abuse.15 Consequently, CAN in children is often not recognised by healthcare professionals, and up to a 10-fold gap between studies based on self-report and child protection agencies is reported.37 Therefore, for this current study, we chose to use both an interview with children and parental questionnaires to diagnose a suspicion of CAN. However, a reference standard for the diagnosis of CAN in children is lacking and instruments differ widely between studies and centres. We, therefore, decided to use several instruments, suitable for a young population, in order to not miss any children with a risk for CAN. Although these instruments are already in clinical use by our specialised CAN team, the validation of the SKPI interview is still in progress.38 Moreover, a recent systematic review showed low specificity of the CSBI for diagnosing sexual abuse.39 It is therefore possible that some children were misclassified as suspected victims of CAN.
Another challenging aspect of diagnosing CAN in children with FC is that symptoms might overlap. CAN may cause behavioural and psychological problems, but these disorders are also common in children with FC.40 Physical examination of children with FC, including inspection of the anorectal area and digital rectal examination, may lead to abnormal behaviour that is also seen in children after CAN. Because the interview was conducted right after the clinic visit, this could also have contributed to the high prevalence of abnormal reactions to the SKPI pictures in this group. Other important markers of sexual abuse during physical examination, such as anal fissures, are also common problems in children with constipation.41 42 Therefore, our findings on physical examination and psychological symptoms in children with FC should be interpreted with care. The use of the SKPI in children with FC should be further investigated.
In addition, the inclusion of a representative healthy control group was not easy. For ethical reasons, recruitment of the index and control group occurred in a different way. While all new patients with FC visiting the outpatient clinic were personally informed about the study, we were only allowed to recruit healthy controls via a newsletter and parents had to actively contact us in order to participate. Our results show that the topic of the study played an important role in the non-participation of many of the contacted schools and parents of both the index and control group. The recruitment is therefore at risk for selection bias, which has important consequences for our study results. Due to the low number of participating parents of healthy controls, it could be that these parents had specific reasons to respond to the research. These parents might have had existing concerns about possible psychological problems or abuse of their child, thereby contributing to the high prevalence of suspected CAN in this group. Moreover, important differences in demographic characteristics between the two study groups in terms of socioeconomic status were found. These differences could have affected our results, given that social factors including socioeconomic status are correlated with risk of CAN.13 Owing to these differences in baseline characteristics and potential selection bias of parents, we cannot draw firm conclusions on our results on parental factors (ie, domestic violence, drug and alcohol abuse) in children with suspected CAN. However, given the current ethical obligations, these challenges are unavoidable and previously described in similar research projects.43
General limitations of the study should be considered when interpreting our results. Unfortunately, we did not meet our power calculations due to slow inclusion rates. It could, therefore, be hypothesised that the study groups were too small to draw firm conclusions. However, the exact prevalence of CAN is unknown, the power calculations were based on an interim analysis, and the important differences in baseline characteristics between study groups, made us decide to preliminary terminate the study. Another limitation is that the interview and questionnaires of cases and controls were not blinded, possibly leading to bias in the interpretation of results. However, to minimise this bias, an independent second observer was appointed to independently score the interviews and only abnormal results of both the first and second observer were used to calculate the prevalence of suspected CAN.
In contrast to the adult literature, we could not confirm the association between CAN and FC. Pathophysiologic differences between adults and children with FC could also play a role. As the association between CAN and FC is mostly described in adults with slow-transit constipation and pelvic floor dyssynergia,4–10 these types of constipation are less commonly acknowledged in young children. It could also be hypothesised that constipation, as a symptom of CAN, will develop over time and the association in young children is, therefore, not present yet. Well-designed longitudinal paediatric studies, with longer follow-up, are therefore needed to confirm this hypothesis.
In conclusion, in this study, we found a high prevalence of suspected CAN, but could not confirm an association between suspected CAN and a diagnosis of FC. Our study demonstrates the many challenges, both ethical and methodological, related to research on the association between CAN and FC. Future research is needed to further unravel the possible gastrointestinal consequences after CAN in order to establish an early detection and prevention of reabuse in children. These observational studies should use a comparable recruitment procedure to include a representative patient and control group, and blinded multidisciplinary assessment to determine the prevalence of CAN.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the local Medical Ethics Committee (file no. METC 2011_059, NL35893.018.11). All parents were asked for written informed consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MHV: conceptualised the study, collected data, drafted the initial manuscript and performed initial data analyses. TFV-B: conceptualiSed the study, collected data and reviewed and revised the manuscript. SB-K: participated in the design of the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript. JHvdL: coordinated and supervised data analyses, and critically reviewed and revised the manuscript. AHT, RJLL and MAB: participated in the design of the study, supervised drafting of the manuscript and critically reviewed the manuscript for important intellectual content. MAB: responsible for the overall content as the guarantor. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.