Article Text

Abstract
Paediatric emergency department (PED) attendances reduced worldwide during the COVID-19 pandemic (2020) but anecdotally babies under 30 days (BUD) appeared less affected. We collated monthly PED attendances (16 years and under) across four hospitals (three district general hospitals and a tertiary specialist PED) in England, UK from January 2017 to December 2020. Gross PED attendances dropped by 34% in 2020 (n=98 256) compared to 2019 (n=148 640). However, cumulative BUD attendances dropped by only 6% in 2020 (n=3922) compared to 2019 (n=4162). Monthly site-specific attendances showed marginal variation. PED attendances broadly decreased in 2020 with less of an impact on BUD.
- COVID-19
- data collection
- health services research
- neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
In 2020 paediatric emergency department (PED) attendances worldwide dropped markedly in parallel with the onset of the COVID-19 pandemic.1–3 This led to investigation of changes in the acuity of children presenting3 and concerns of potential delayed diagnosis4 or referral.5
In the UK rapid reconfiguration of services occurred in early 2020 across the breadth of healthcare (primary, secondary and tertiary care) as well as within community services and wider formal/informal support networks. Assorted national/local lockdowns and limitations on social contact were implemented which affected PED presentations but anecdotally the authors noted attendances for babies were not affected to the same extent. We sought to describe this cohort more fully.
Our four institutions comprise three (Frimley Park Hospital, Watford General Hospital and Wexham Park Hospital) large district general hospitals (DGH) with co-located PEDs and Leicester Children’s Hospital, a regional children’s hospital that provides secondary and tertiary care via a dedicated PED. Data were collated at an aggregated level (ie, age ranges) through each hospital’s business intelligence team. No patient-level data were obtained and formal ethics permission was not sought as this project was defined as a service evaluation as per National Institute for Health Research guidance.
Table 1 shows varied rises in PED attendances from 2017 to 2019, with a marked change in 2020 with 34% fewer PED attendances (16 years and under) across the four departments (98 256 attendances 2020 vs 148 640 attendances 2019). This reduction in attendances closely correlates with other UK studies looking at this period showing a 30% reduction in attendances.1 3
Yearly paediatric emergency department attendances 2017–2020 as total number and babies 30 days and under (BUD)
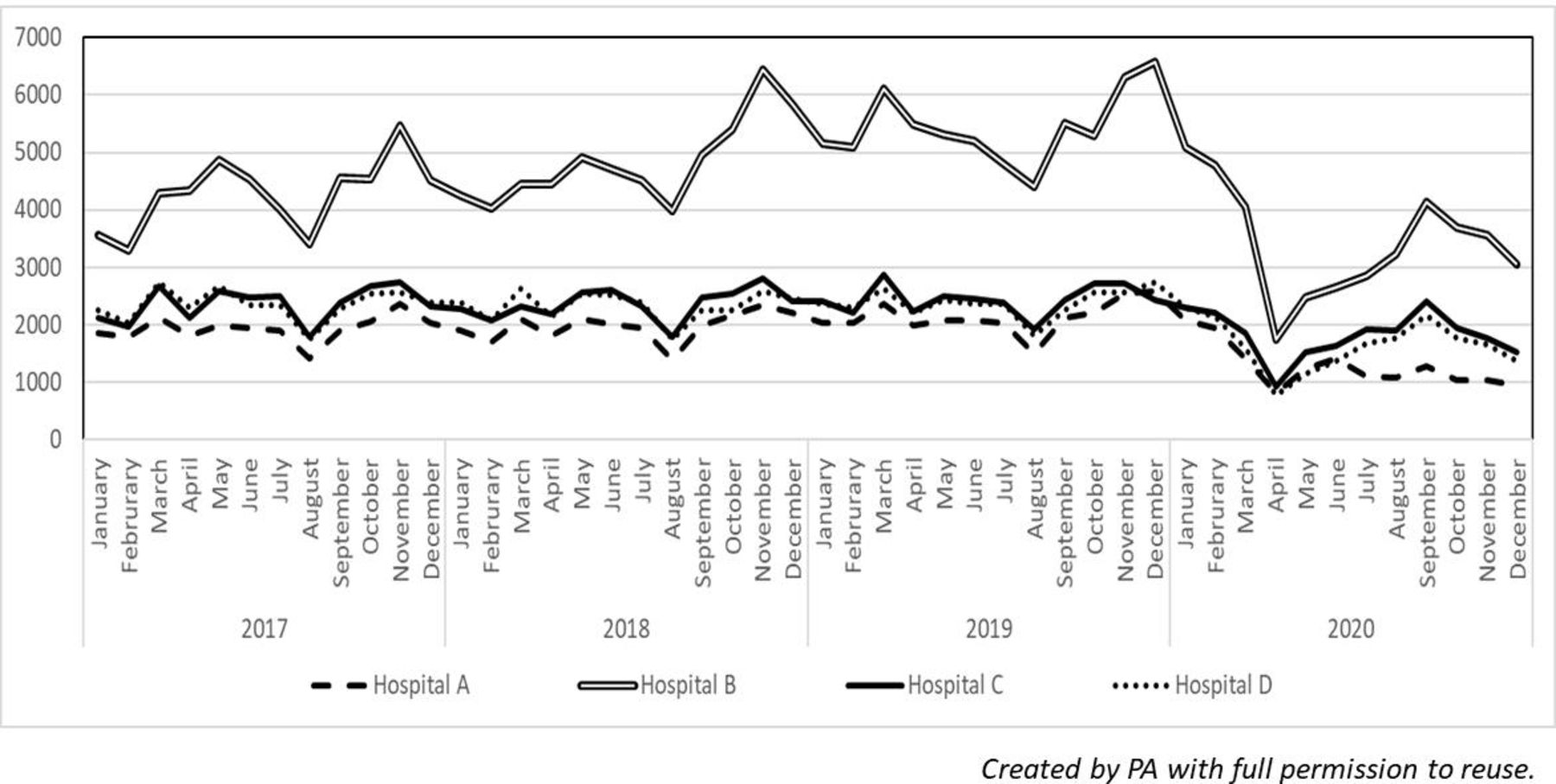
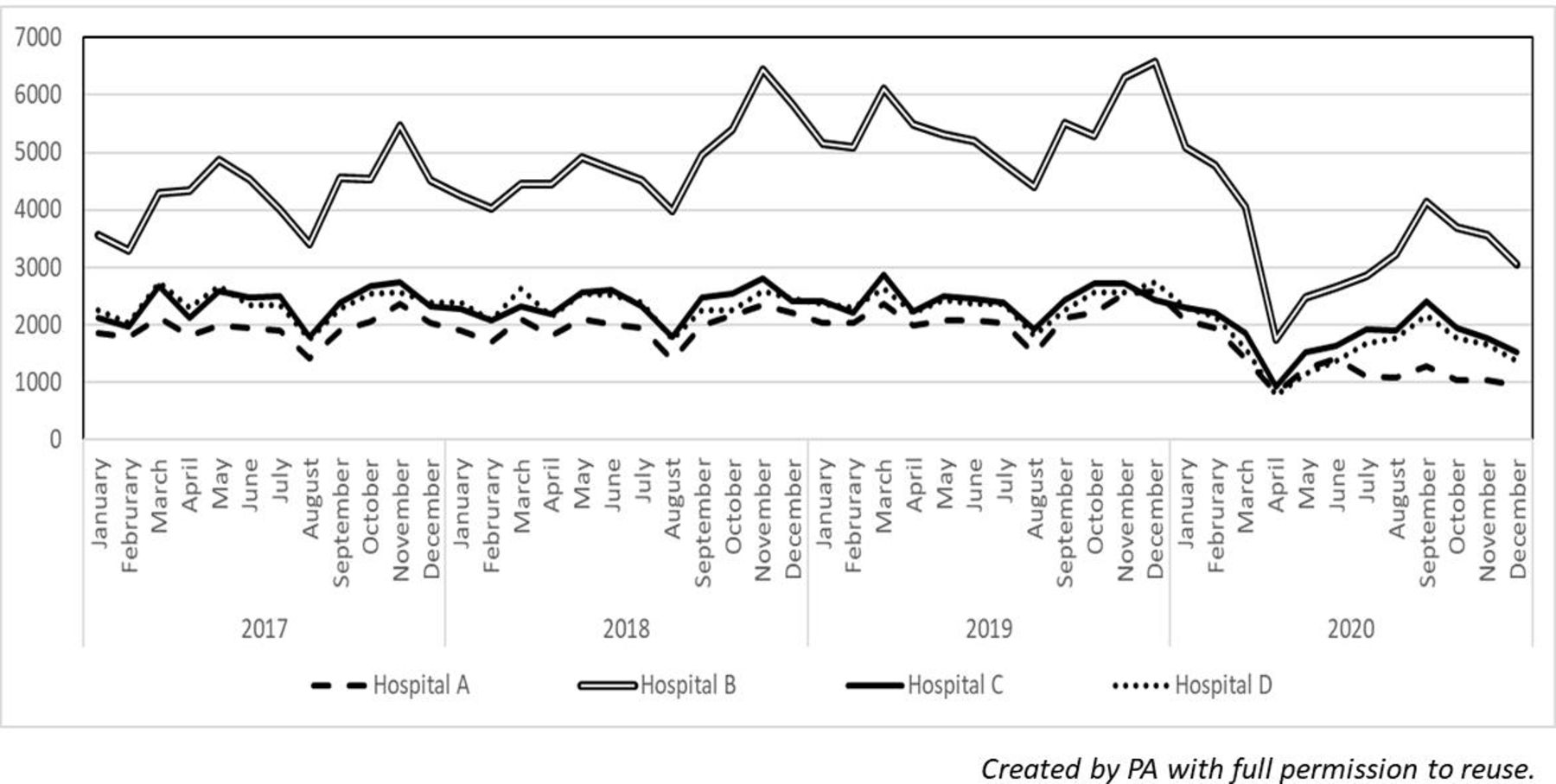
The most noticeable change in attendances (figure 1) occurred March–April 2020 with a 68%–59% reduction in April 2020, compared with April 2019, across all sites (online supplemental table 1). This coincided with the first restrictions on social contact and national lockdown. Attendances show a relative increase May 2020 onwards, although hospital A showed more of a plateau June–December 2020 compared with the other three hospitals.
Supplemental material
{kind=link}
Total monthly paediatric emergency department attendances per site (2017–2020).
In babies 30 days and under (BUD) and in contrast to the 34% reduction in overall PED attendances there was a 6% reduction (table 1) in attendances in 2020 (3922) across all PED’s compared to 2019 (4162) with site-based variation (online supplemental table 2).
Supplemental material
Our data suggest that although PED attendances broadly decreased in 2020 this drop does not appear to have been consistent and with less of an impact on BUD. A recent paper6 from Italy suggests under-28-day-old babies increased in attendances March–April 2020 compared with 2019 mostly due to feeding related issues. Our data support the notion of a separate driver for BUD attendances.
With the rapid reconfiguration of services and limitations on social contact as COVID-19 affected the UK, the impact of these changes on family’s decision making is still unclear. Formal healthcare support (eg, health visitors, primary care, hospital outpatients) reportedly increased over 2020 coupled with permitted ‘social/care bubbles’. However, informal (eg, support groups) and face-to-face medical contact was limited for the majority of 2020 and PED may have been the only service available to families for face-to-face contact.
Our results may not be generalisable as data were taken from only four hospitals, three of whom have similar yearly attendance numbers (table 1). However, historic monthly attendance patterns (figure 1) are broadly comparable between sites which suggests it is likely reflective of other UK hospitals and is further supported by a recent paper7 from Bristol Royal Hospital for Children on neonatal ED attendances 2016–2020.
Our data may highlight variation in local non-ED based service provision (eg, maternity, health visitors and primary care) or referral pathways. Hospitals A, C and D are all DGH’s with similar yearly PED attendance numbers. However, hospital A has a higher BUD PED attendance baseline compared with hospitals C and D.
This data is important when planning service provision for future pandemics and whether children and infants (especially those less than 30 days) should have different health policy interventions.
Ethics statements
Patient consent for publication
Acknowledgments
Fran Franks and Kate Pampin-Cao for their support and feedback on the manuscript.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PA is the overall guarantor who planned, conducted and reported the study. SW, DR, RGB and GM all planned and reported the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests I have previously collaborated with Dr Roland on other projects. Nil other competing interests declared.
Patient and public involvement statement There was no patient or public involvement in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.