Article Text

Abstract
Background Recent longitudinal studies suggest stable cognitive development in preterm children, although with great individual variation. This prospective neurocognitive follow-up study of extremely low birthweight (ELBW, <1000 g) children aimed to characterise groups with different developmental trajectories from preschool to preteen age.
Methods ELBW children (n=115) born in Finland in 1996–1997 participated in cognitive assessments at a median age of 5.0 years and 11.3 years. A standardised test of intelligence (Wechsler Preschool and Primary Scale of Intelligence–Revised or Wechsler Intelligence Scale for Children–third edition) was administered at both ages.
Results Three ELBW groups with different developmental trajectories over time were identified with latent class growth analysis. Children with average (Full-Scale IQ (FSIQ): 85–115) and below average (FSIQ: <85) intelligence at 5 years of age had significant decreases in intelligence scores by 11 years of age (–11.7 points and –14.9 points, respectively, both p<0.001), while those with above average intelligence (FSIQ: >115) showed stable development (–3.2 points, p=0.250). Multiple linear regression showed that neonatal complications (intraventricular haemorrhage grade 3–4 and blood culture positive sepsis) and maternal education significantly predicted lower intelligence at the second assessment (F(3,106)=7.27, p<0.001, adjusted R2=0.147).
Conclusions ELBW children represent a heterogeneous patient population in which groups with different cognitive trajectories can be detected. Deterioration may occur particularly in children with initial average or below average cognitive performance at 5 years of age, with neonatal complications and lower maternal education presenting as risk factors. Catch-up in cognitive functions seems more uncommon in the ELBW population, which should be noted in clinical work.
- Neonatology
- Psychology
- Neurology
Data availability statement
No data are available. Due to ethical reasons and the nature of this study, supporting data are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Extremely low birthweight children have on group level low average intelligence, but less is known about their developmental trajectories over time.
While contradictory research results suggest that their development is stable or may deteriorate, some children may experience developmental gains.
What this study adds?
Using latent class growth analysis, subgroups of extremely low birthweight children with different developmental trajectories from preschool to preteen years were identified.
Deterioration in intelligence scores occurred particularly in children with initial average or below average intelligence.
Long-term follow-up with individualised supportive intervention is warranted, despite average intelligence before school age.
Introduction
Extremely low birthweight (ELBW, <1000 g) children and very preterm (VPT; gestational age (GA): <32 weeks) children score significantly lower on assessments of intellectual functions compared with full-term born peers, performing on group level in the low average range.1–3 In two meta-analyses, the difference in mean IQ between preterm and full-term children at school age was 11.9–12.9 points,4 5 and if born before GA 28 weeks 13.9 points.4
It is unclear whether ELBW children catch up with their term-born peers over time. In children born extremely preterm, significantly lower motor, language and cognitive skills persisted between 1 year and 3 years of age.6 The lag in fine and gross motor skills grew over time compared with term-born peers, while language and cognitive functions were more stable. At school age, the majority of longitudinal studies in very low birthweight (VLBW, <1500 g) children and VPT children have shown stability in IQ scores over time with a persistent developmental lag on group level throughout school years, into adolescence7–9 and early adulthood.10 11 However, even deteriorating IQ has been reported between assessments at 7–8 years and 14–15 years of age.12 13 In one study on VPT children, cognitive gains, such as improvements in receptive vocabulary and IQ, occurred between 3 years and 8 years,14 but only gains in receptive vocabulary remained significant in assessments between 8 years and 12 years of age.7
As patterns of development show individual variation, a new research approach is to move from cohort-level analyses to identifying groups of preterm children with different developmental patterns within the cohort. In two studies, a group of VLBW children with average IQ at 5–8 years of age had a stable developmental path or even made some gains until 16–18 years of age, while another group with initially poor scores had stable or even deteriorating IQ. Although catch-up in development was generally not seen, in both studies a proportion of VLBW children made significant gains in IQ.7 9 The absence of neurological or sensory impairment, severe brain injury and perinatal complications as well as higher maternal education and better socioeconomic status were protective factors for long-term development.7–9
This study aimed to identify groups with different cognitive trajectories between preschool and preteen years in a national cohort of ELBW children. Predictors of developmental risk over time were analysed to identify children in need of intensified support and long-term follow-up.
Patients and methods
Study group
This study is part of the FinELBW study, including survivors from a national cohort of children in Finland born alive during a 2-year study period (1996–1997) with a birth weight of 500–1000 g and GA ≥22 weeks. Of the included 351 infants, 206 were alive at 5 years of age. Of these, nine children were severely disabled and unable to attend assessment. Furthermore, 25 families declined participation. Of the 172 children participating in the intellectual assessment at 5 years of age, 115 (67%) participated in the follow-up at 11 years of age. At the 11-year time point, 8 children were excluded due to severe impairment, 20 families could not be reached and 29 families declined participation. The study population and cognitive follow-up results have been described previously at 2 years, 5 years and 11 years.15–17
Patient and public involvement
Patients were not involved in the study design.
Assessments
Intellectual capacity was assessed with the Wechsler Preschool and Primary Scale of Intelligence–Revised (WPPSI-R) at a median age of 5.0 years (IQR: 5.0–5.2 years) and the Wechsler Intelligence Scale for Children–third edition at 11.3 years (IQR: 11.2–11.9 years).18 19 For longitudinal analyses, the subtests Information and Vocabulary were compiled into the estimated Verbal IQ (VIQ) and Block Design and Picture Completion into the estimated Performance IQ (PIQ). The estimated VIQ and PIQ were used for longitudinal comparisons to ensure compatibility (same subtests used). However, the Full-Scale IQ (FSIQ) used for categorical measurements of change, comprised the full version. FSIQ at 5 years included additionally the subtests Comprehension, Arithmetic (VIQ) and Object Assembly (PIQ) and FSIQ at 11 years included Similarities (VIQ) and Coding (PIQ). IQ has a mean of 100 (SD: 15), higher scores indicate better performance.
A psychologist or a trained undergraduate student in psychology (different at time points 1 and 2) assessed the children at the closest of the 5 university hospitals in Finland. Medical data on all ELBW infants were collected prospectively into a research register maintained by the Finnish National Research and Development Center for Welfare and Health.
Statistical analyses
Background variables of the participating children and children lost to follow-up were compared with independent samples t-test and exact χ2 test. To identify different developmental trajectories, latent class growth analysis (LCGA) was performed based on estimated VIQ and PIQ at 5 years and 11 years. The LCGA analyses were conducted with Mplus,20 and the model fit was assessed by the Akaike information criterion, Bayesian information criterion (BIC), sample-size adjusted BIC and entropy. Model fit was also assessed by comparing the Vuong-Lo-Mendell-Rubin likelihood ratio test.
Changes in intelligence scores between the groups identified in the LCGA were analysed with a repeated-measures Analysis of Covariance with estimated PIQ and VIQ scores at 5 years and 11 years as the within-subjects factors. The analysis was controlled for sex and maternal education (four levels: comprehensive school, vocational school, matriculation examination or higher education). A separate repeated-measures Analysis of Variance was then undertaken for a subgroup with GA <27 weeks. Because birth weight was used as an inclusion criterion in this study, there was an increasing ratio of fetal growth restriction in infants born in GA ≥27 weeks. Since recent studies have used GA as a cut-off for prematurity, this follow-up analysis is more comparable to recent studies. No significant effect of maternal education or sex was observed in the subgroup analysis. Due to the relatively small sample size, in the final subgroup analysis, maternal education and sex were not controlled for. For the univariate analyses, p values were corrected using the Bonferroni correction. Age-standardised test scores were used.
Change in performance was further compared between 5-year FSIQ and 11-year FSIQ for the individual children. Change was defined as increase (>1 SD, ie, 15 points), stable (within 1 SD) or decrease (>15 points). Change in performance between the three groups was analysed with the exact χ2 test. At the 5-year time point, there were missing data for the WPPSI-R subtests Comprehension (n=3), Vocabulary (n=5), Arithmetic (n=13) and Picture Completion (n=2), and the IQs were based on the subtests available.
Risk factors that have previously been associated with outcome or that were theoretically of interest were included in a multiple regression analysis to find associations to FSIQ at 11 years. These included the medical risk factors GA, antenatal steroid treatment, intraventricular haemorrhage (IVH) grades 3–4, retinopathy of prematurity stages 3–4, blood culture positive sepsis, necrotising enterocolitis, oxygen dependency at the age corresponding to GA 36 weeks and multiparity,16 and the psychosocial risk factor maternal education. Because the risk factors small for GA (birth weight: <2 SD of the mean for GA based on Finnish standards) and GA were strongly correlated, they were included in separate analyses. However, the results reimaned the same. Five children had missing data on perinatal morbidities and were excluded from the regression analyses.
Statistical analyses were carried out with IBM SPSS Statistics V.27.0,21 unless otherwise specified. Tests of significance were two-tailed, and p <0.05 was considered significant. Partial eta-squared (ηp2) and R2 served as indicators of effect size. In ηp2, 0.01 represents a minimal, 0.06 a medium and ≥0.14 a large effect size.22
Results
Characteristics of the study cohort
Children who were lost to follow-up had a significantly lower FSIQ at 5 years compared with the participating children. The incidence of cerebral palsy tended to be higher in the non-participating group, but the difference was not statistically significant. The groups did not differ in other background or clinical risk factors (table 1).
Background characteristics and risk factors of the 115 ELBW children attending follow-up assessment at 11 years of age and the 57 non-participants
Developmental trajectories on group level
In the LCGA, the fits from 1-class to 9-class models were analysed (table 2). The likelihood-ratio favoured two classes and BIC three classes, but the difference was small. Since three classes had more predictive power and added information to the theoretical interpretation, it was chosen for the analyses. These three classes were named based on FSIQ results at 5 years as the below average, that is, −1 SD from the mean or FSIQ <85, (n=20, 17%), average (n=59, 51%) and above average, that is, +1 SD from the mean or FSIQ >115, groups (n=36, 31%). Mean FSIQ at 5 years was 66.8 (SD: 14.0) for the below average, 96.5 (12.5) for the average and 118.8 (10.3) for the above average group.
The fits from a 1-class model to a 9-class model in the LCGA
In intellectual reasoning between 5 years and 11 years of age, there was a significant main effect of group (F(2,110)=275.83, p<0.001, ηp2=0.834). Performance on both PIQ and VIQ was significantly different between the three groups at both time points (table 3). There was a significant effect of time (F(1,110)=7.18, p=0.008, ηp2=.061) with overall test scores deteriorating by −9.9 points (95% CI −6.6 to −13.2). However, a significant time×group interaction indicated that test scores changed differently depending on group belonging (F(2,110)=3.97, p=0.022, ηp2=.067) (figure 1). In Bonferroni corrected post-hoc analyses, the below average (mean difference: −14.9 points, p<0.001) and average (mean difference:−11.7, p<0.001) groups deteriorated significantly, while the above average group showed stable development (mean difference:−3.2, p=0.250). No significant effect of test appeared (F(1,110)=0.843, p=0.361, ηp2=0.008), indicating similar performance in PIQ and VIQ. Of the background characteristics, there was a main effect of maternal education (F(1,110)=5.87, p=0.017, ηp2=0.051), with lower education level being associated with lower test scores. No significant effect of sex was observed.
Mean values (SE) for 115 ELBW children on intelligence tests at 5 years and 11 years with F and p values from repeated measures Analysis of Covariance with Bonferroni corrected post-hoc tests adjusted for sex and maternal education level
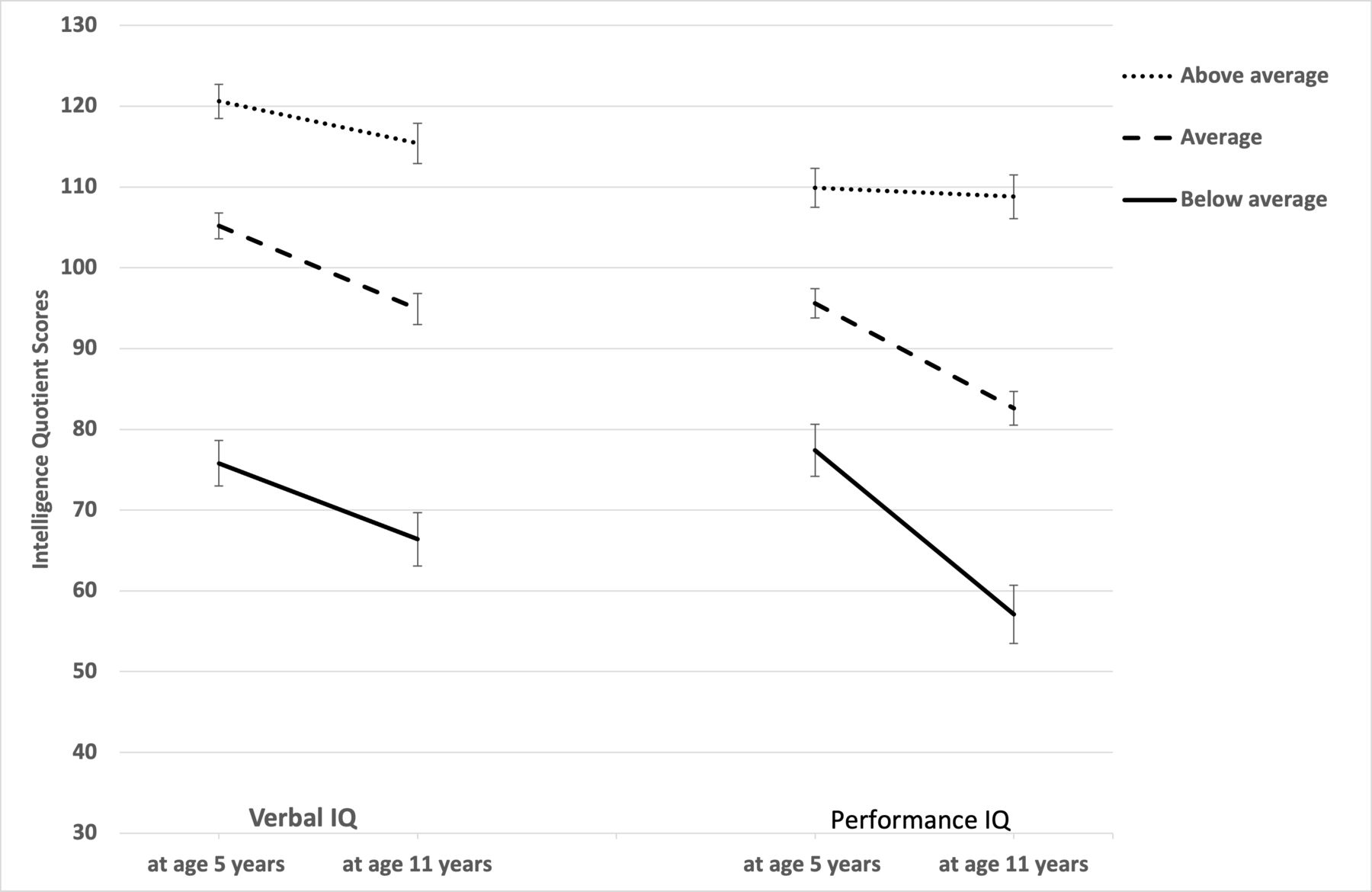
The difference in mean values (SE) for 115 ELBW children on intelligence tests at 5 years and 11 years, presented separately for the three groups identified in the LCGA. ELBW, extremely low birthweight; LCGA, latent class growth analysis.
If children with cerebral palsy (n=11) were excluded from the analysis, the results remained. There was a significant effect of time (F(1,99)=11.40, p=0.001, ηp2=0.103) with overall test scores deteriorating by −9.8 points (95% CI −6.5 to −13.0).
Subgroup with GA <27 weeks
When cognitive outcome was analysed in the subgroup with GA <27 weeks (n=60), the significant effects of group (F(2,57)=162.84, p<0.001, ηp2=0.851) and time (F(1,57)=16.10, p<0.001, ηp2=0.220) remained. However, the time×group interaction was no longer significant (F(2,57)=0.94, p=0.395, ηp2=0.032). Overall test scores deteriorated by −9.2 points (95% CI −4.4 to −13.8). The below average (n=11, –13.2 points, p=0.009) and average (n=33, –9.7 points, p=0.001) groups deteriorated significantly, while the above average group showed stable development (n=16, –4.8 points, p=0.237).
Developmental trajectories on individual level
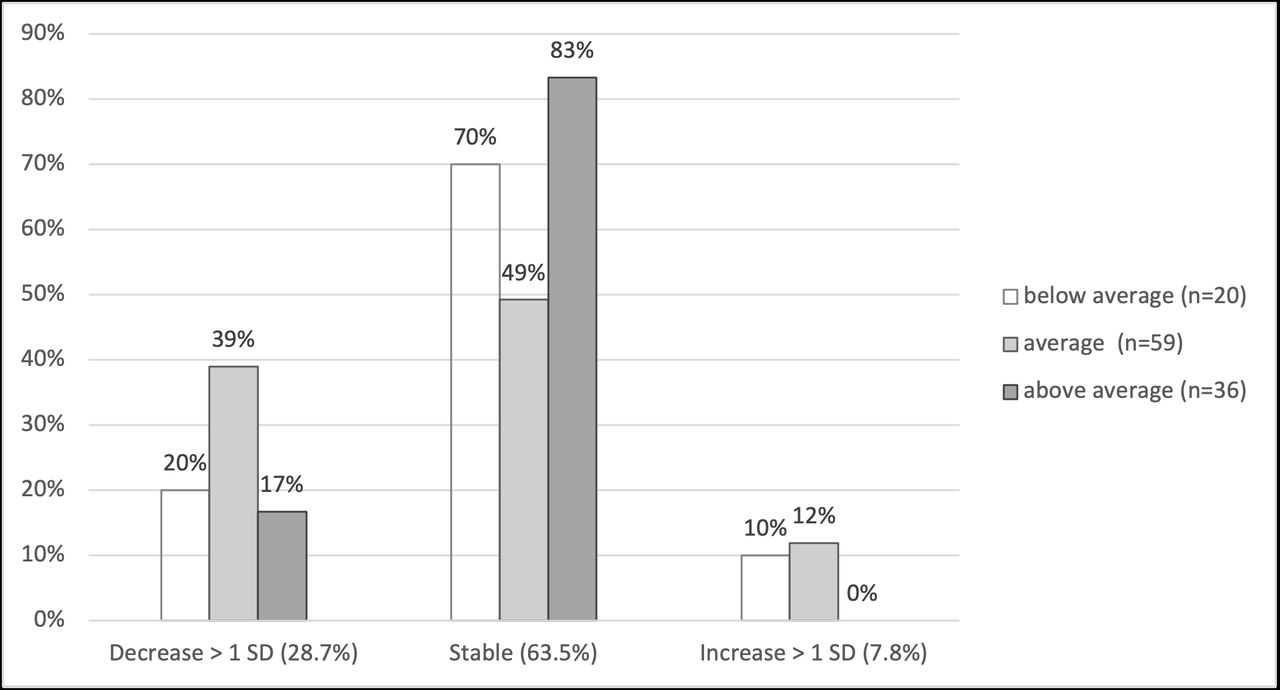
In analyses of change of more than 15 points (ie, 1 SD) in individual test scores between the 5-year and 11-year assessments, there were significant differences between the groups (χ2(4)=12.96, p=0.010) (figure 2).
{kind=link}
{kind=link}
Percentages of ELBW children with decrease, increase and stability in FSIQ scores between 5 years and 11 years of age. Change was defined as test scores changing more than 15 points (>1 SD). Results are presented separately for the three groups identified in the LCGA. ELBW, extremely low birthweight; FSIQ, Full-Scale IQ; LCGA, latent class growth analysis.
Risk analysis
A significant regression equation was found (F(3,106)=7.27, p<0.001, adjusted R2=0.147). The absence of IVH grades 3–4 (β=–0.270, p=0.003), sepsis (β=–0.209, p=0.020) and higher maternal education level (β=0.230, p=0.011) were significant predictors of higher FSIQ at 11 years of age.
Discussion
To identify different developmental trajectories in a national ELBW cohort, three outcome groups were defined based on LCGA. ELBW children with below average and average IQ at 5 years had on group level decreasing intelligence scores between preschool and preteen years, while those with high average IQ at 5 years had stable development. Both clinical risk factors (IVH and sepsis) as well as maternal education level predicted IQ at 11 years.
The majority of previous studies found stable cognitive development over time10 11 23; however, declining IQ scores have also been reported.12 13 This discrepancy may be accounted for by differences in study inclusion with different GA and birthweight criteria used as well as differences in assessment methods. Our study group resembles those that have assessed children born at GA 32 weeks or less.8 12 13 Furthermore, we used similar subtests at both time points to compile comparable estimated IQs, while in many previous studies the compiled IQs have been based on different subtests, thus, possibly assessing somewhat different functions at different ages.8 9
A new line of research is to identify groups of children with different developmental paths.7–9 In our study, three groups of ELBW children were identified: 17% with below average, 51% with average and 31% with above average intelligence at 5 years of age. On group level, the above average group was the only group without significant decline in IQ scores during a 6.3-year follow-up. Results of previous studies have been inconclusive with low performance being associated both with stable development11 and decrease in scores over time.9 On individual level, most children had stable IQ, when defined as test scores within one SD between assessments. Significant decrease was greatest among ELBW children with average IQ at 5 years, of whom more than a third decreased their scores. Increase in scores was more unusual, as has been reported previously.7 9 This will lead to an increased number of children with suboptimal intelligence and highlights the importance of long-term follow-up through school years. The decrease in scores could not be attributed to cerebral palsy. Cognitive development may be affected even in the absence of obvious developmental problems in early development.
The risk factors found in this study are well established in previous literature. A detrimental effect of brain damage in particular7 8 but also neonatal clinical complications5 9 24 on development are evident in the preterm population. Sepsis per se has not presented as a risk factor for cognitive outcome in meta-analyses.5 25 Low maternal education and family social risk,7–9 but even more so the combination of high social risk and medical or neurological complications have been highlighted as risk factors for cognitive development.8 26 Improvements in perinatal care to minimise brain damage and other major neonatal morbidities, optimise nutrition and efforts to give extra support particularly to families with lower parental education are important steps in supporting cognitive development for preterm children.
A limitation in this study was the lack of a control group to control for normal developmental change and possible effects of different test methods used at the two time points. Furthermore, the cohort was enrolled in 1990s when birth weight was a commonly used inclusion criterion. The attrition rate was 33%, somewhat higher than reported in many other studies.8 9 13 Children from disadvantaged socioeconomic backgrounds and with lower cognitive functions are more likely to drop out.11 Hence, this may be the best-case scenario of cognitive results. In cohorts enrolled after the turn of the millennium, survival of the most immature has increased. However, according to two meta-analyses, similar IQ results were found, irrespective of publication year or birth year of the cohort, covering more than 40 years of studies.4 5 Thus, the results of this study may be generalisable for ELBW children growing up today.
Conclusion
In this ELBW population, the stable or decreasing intelligence scores indicate that the majority do not outgrow their cognitive deficits. On the contrary, a group of ELBW children are at a risk of not keeping up with the expected developmental pace, leading to a decline in intelligence scores between preschool and preteen years. Consequently, it is important to monitor and support development in this patient population throughout school years, even if average cognitive skills have been reported prior to school start. Cognitive assessment helps in evaluating the need of rehabilitation services and planning timely educational support.
Data availability statement
No data are available. Due to ethical reasons and the nature of this study, supporting data are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The ethics committee of the Helsinki University Hospital (102/E7/2006, 21 April 2010) and the National Institute for Health and Welfare (1617/504/2006, 12 January 2007) approved the study. Written informed consent was obtained from the child and the parents.
References
Footnotes
Collaborators The Finnish ELBW Cohort Study Group members: Annika Koivisto, MA in Psychology, Attentio Oy, Turku, Finland. Professor Marit Korkman, PhD, Department of Psychology and Logopedics, University of Helsinki, Helsinki, Finland. Deceased, April 2012. Professor Liisa Lehtonen, MD, PhD, Head of Neonatology, Turku University Hospital, Pediatrics, Turku University, Turku, Finland. Tuija Löppönen, MD, PhD, Pediatric Neurologist, Kuopio University Hospital, Kuopio, Finland. Päivi Olsén, MD, PhD, Pediatric Neurologist, Oulu University Hospital, Oulu, Finland. Outi Tammela, MD, PhD, Adjunct Professor in Neonatology, Head of Division in Neonatology, Pirkanmaa Hospital District, Tampere Center of Child Health Research, Tampere, Finland. The authors express our sincere gratitude to late professor Marit Korkman for her significant contribution in initiation and implementation of this study.
Contributors AH conceptualised and designed the study, carried out the analysis of the data, interpreted the data, drafted the initial manuscript, revised the manuscript, and acted as the guarantor. LK participated in conceptualising and designing the study, interpreted the data and reviewed and revised the manuscript. AL, VT and KM participated in the acquisition of data and revised the manuscript. VF designed the data collection instruments, coordinated and supervised data collection, conceptualised and designed the study and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding Signe and Ane Gyllenberg Foundation (VF, AH), Medicinska Understödsföreningen Liv och Hälsa rf (VF).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.