Article Text

Abstract
Introduction Over half of the 5 million annual deaths among children aged 0–59 months occur in sub-Saharan Africa. The period immediately after hospitalisation is a vulnerable time in the life of a child in sub-Saharan Africa as postdischarge mortality rates are as high as 1%–18%. Identification of neonates and children who are at highest risk for postdischarge mortality may allow for the direction of interventions to target patients at highest risk.
Methods and analysis The Predicting Post-Discharge Mortality study is a prospective, observational study being conducted at Muhimbili National Hospital (Dar es Salaam, Tanzania) and John F. Kennedy Medical Center (Monrovia, Liberia). The aim is to derive and validate two, age population specific, clinical prediction rules for the identification of neonates (n=2000) and children aged 1–59 months (n=2000) at risk for all-cause mortality within 60 days of discharge from the neonatal intensive care unit or paediatric ward. Caregivers of participants will receive phone calls 7, 14, 30, 45 and 60 days after discharge to assess vital status. Candidate predictor variables will include demographic, anthropometric and clinical factors. Elastic net regression will be used to derive the clinical prediction rules. Bootstrapped selection with repetitions will be used for internal validation. Planned secondary analyses include the external validation of existing clinical prediction models, determination of clinicians’ ability to identify neonates and children at risk of postdischarge mortality at discharge, analysis of factors associated with hospital readmission and unplanned clinic visits and description of health-seeking behaviours in the postdischarge period.
Ethics and dissemination This study received ethical clearance from the Tanzania National Institute of Medical Research, Muhimbili University of Health and Allied Sciences, the John F. Kennedy Medical Center Institutional Review Board, and the Boston Children’s Hospital Institutional Review Board. Findings will be disseminated at scientific conferences and as peer-reviewed publications.
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Postdischarge mortality rates among children in sub-Saharan Africa are estimated to be as high as 1%–18%.
Two clinical prediction rules have been derived from studies conducted in Uganda and Mozambique to identify children at risk of postdischarge mortality in sub-Saharan Africa.
Neither of the existing clinical prediction rules have been externally validated and have not specifically targeted neonates.
What this study hopes to add?
This prospective, observational cohort study in Liberia and Tanzania will derive and validate two, novel, population-specific, clinical prediction rules to identify neonates and children at risk of postdischarge mortality·
This study will elucidate clinician gestalt in the identification of neonates and children at risk of postdischarge mortality·
This study will add further understanding of postdischarge health-seeking behaviours for children in sub-Saharan Africa.
Introduction
Since the 1990s, mortality rates among children under 5 years of age decreased by >50% globally.1 However, progress in reducing childhood mortality has been geographically uneven, with more than half of the 5 million annual deaths among children occurring in sub-Saharan Africa.2 Limited access to healthcare providers, long distances to healthcare facilities and delayed care seeking contribute to high rates of childhood mortality in sub-Saharan Africa.3–5
Recently, emphasis has been placed on increasing access to high-quality healthcare for children in sub-Saharan Africa.6 However, the period immediately after hospitalisation is a vulnerable time in the life of a child in resource-limited settings. Postdischarge mortality rates among children in parts of sub-Saharan Africa are estimated to be as high as 1%–18%, even outpacing inpatient mortality rates in some studies.7 Despite this documented vulnerability, postdischarge mortality has largely been neglected in policy and practice.8
Two clinical prediction rules have been derived to identify children at risk of postdischarge mortality in single countries in sub-Saharan Africa. Wiens et al derived a model to identify infants and children aged 6–59 months at risk of postdischarge mortality up to 6 months after discharge from two Ugandan hospitals with suspected or proven infections.9 In addition, Madrid et al derived a model to identify children aged <15 years admitted with all diagnoses at risk of 90-day postdischarge mortality in Mozambique.10 Only malnutrition, HIV-positive status and altered mental status were associated with postdischarge mortality in both studies. All other clinical parameters associated with postdischarge mortality differed between these two studies.
Neither of these clinical prediction rules have been externally validated, making their impact on reducing postdischarge mortality unclear. Moreover, neonates have not been the focus of either clinical prediction rule despite contributing to nearly half of all deaths among children aged 0–59 months.11 Factors that predict postdischarge mortality for neonates may differ from those for children 1–59 months due to differences in leading causes of death by age. Identification of neonates and children who are at highest risk for postdischarge mortality may allow for the direction of interventions to target patients at highest risk.8
To this end, the Predicting Post-Discharge Mortality (PPDM) study will derive and validate two, age population-specific, clinical prediction rules to identify neonates and children aged 1–59 months at risk of all-cause mortality within 60 days of discharge from the neonatal intensive care unit (NICU) or paediatric ward at two sites in sub-Saharan Africa.
Methods
Study design
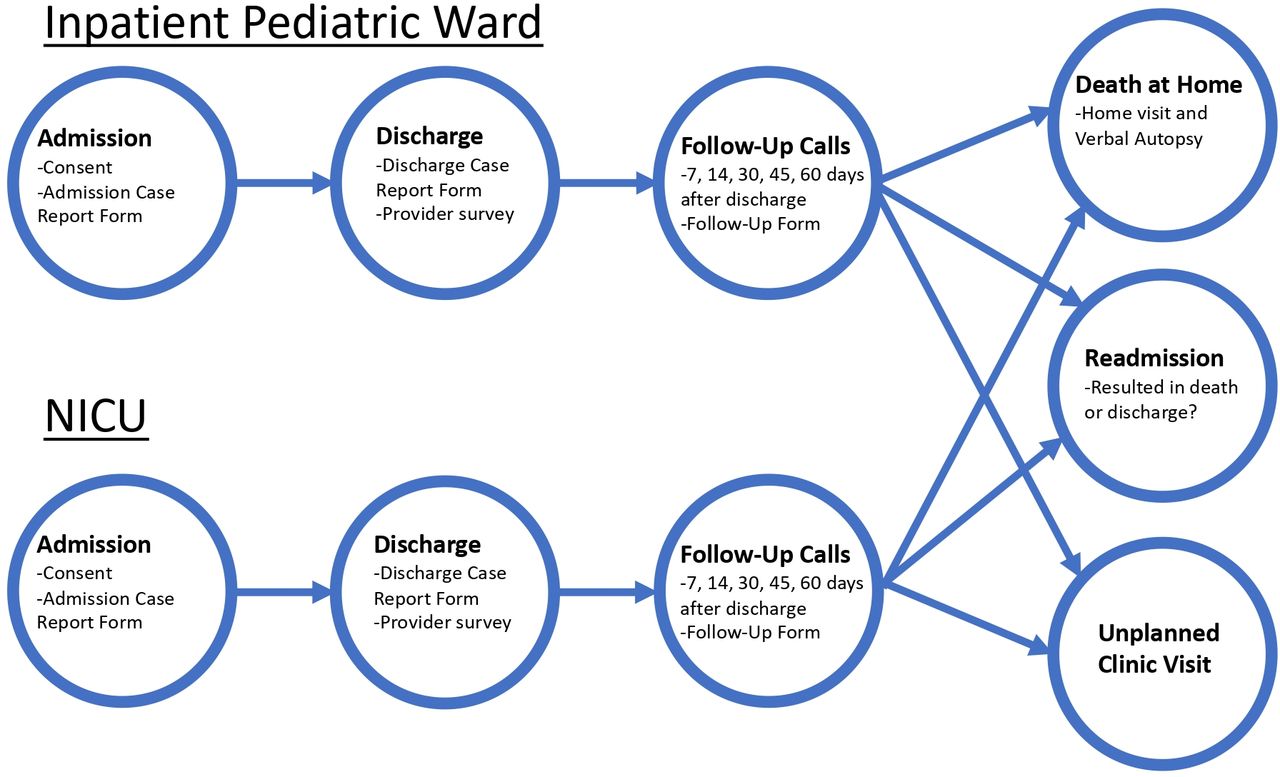
PPDM is a prospective, observational study being conducted at Muhimbili National Hospital in Dar es Salaam, Tanzania and John F. Kennedy Medical Center in Monrovia, Liberia. The study protocol was developed by collaborators in Tanzania (Muhimbili University of Health and Allied Sciences and Muhimbili National Hospital), Liberia (John F. Kennedy Medical Center) and the USA (Boston Children’s Hospital, Harvard T.H. Chan School of Public Health and Emory University School of Medicine). The study diagram is included in figure 1. Enrolment began on 1 October 2019. Patient follow-up data collection will conclude on 31 January 2022. This protocol follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cohort studies (online supplemental file 1).
Supplemental material
{kind=link}
The Predicting Post-Discharge Mortality study design. (NICU: neonatal intensive care unit).
The combined study population between Liberia and Tanzania will be approximately 4000 participants (2000 neonates, 2000 children aged 1–59 months) who are discharged from the two sites. Each site will enrol 1000 neonates and 1000 children aged 1–59 months. Enrolled neonates and children will be followed through phone calls after discharge at 7, 14, 30, 45 and 60 days to assess postdischarge outcomes and health-seeking behaviours.
Patient and public involvement
Caregivers, patients and the public were not involved in the development of the study protocol.
Primary and secondary objectives
The primary objective of the study is to derive and internally validate two, age population-specific, clinical prediction rules to identify neonates and children aged 1–59 months at risk of postdischarge mortality within 60 days of discharge from the NICU or paediatric ward at two sites in sub-Saharan Africa. Our secondary objectives are to (1) externally validate existing clinical prediction rules for postdischarge mortality developed from studies in Uganda and Mozambique,9 10 (2) determine clinicians’ ability to accurately identify neonates and children at risk of postdischarge mortality and hospital readmission at the time of hospital discharge, (3) describe factors associated with hospital readmission and unplanned clinic visits after discharge and (4) describe health-seeking behaviours in the postdischarge period among children who die as well as those who survive beyond 60 days.
Study setting
Muhimbili National Hospital and John F. Kennedy Medical Center are large, referral, training hospitals for Tanzania and Liberia, respectively. Both hospitals are government hospitals supported by each country’s Ministry of Health. Both hospitals are located in urban areas with surrounding populations of 4 million for Muhimbili National Hospital and 1.5 million for John F. Kennedy Medical Center. Both hospitals have approximately 140–150 paediatric discharges and approximately 170 NICU discharges per month.
Eligibility
We will include participants aged 0–59 months with all diagnoses who are discharged from the NICU or the paediatric ward. Participants will be included if their caregivers consent to have their hospital admission data gathered and to receive follow-up phone calls. We will exclude children who (1) die during their initial hospitalisation, (2) are older than 59 months of age or (3) have non-consenting caregivers. We will not enrol participants who are transferred to other hospitals; however, both hospitals are large referral hospitals and, therefore, transfer out is rare.
Sample size
Previous studies at Muhimbili National Hospital evaluating patients with malnutrition and abdominal pain suggest postdischarge mortality rates as high as 13%–15%.12 13 Since there are no previous studies describing postdischarge mortality at John F. Kennedy Medical Center and postdischarge mortality rates among all discharged patients at Muhimbili National Hospital may be lower than among specific populations, we conservatively estimate a 5% postdischarge mortality rate. We also anticipate a lost-to-follow-up rate of 3% in each cohort. Therefore, we will enrol 1000 patients in each cohort (NICU and paediatric wards) at each site (n=4000 total) to derive and validate two, age population-specific, clinical prediction rules to predict postdischarge mortality (2000 in each population). We expect at least 100 deaths and 150 hospital readmissions in each cohort. Using the rule of 10 events per item in a clinical prediction rule and assuming a 5% mortality rate, we will be able to include at least five variables in each clinical prediction rule for postdischarge mortality.14
Standard of care
All enrolled children will receive standards of care per Tanzanian Ministry of Health guidelines at Muhimbili National Hospital and standards of care set forth by the John F. Kennedy Medical Center and the Liberian Ministry of Health. This care will be provided by the clinical care teams and not by this study’s staff.
Recruitment
Caregivers of participants will be approached by research assistants at the time of hospital discharge and asked to consent to the study. Consenting providers will provide informed consent in their own language (written in Kiswahili or witnessed thumbprint if not literate in Tanzania and verbal consent in English in Liberia). We will collect data at the time of discharge using a secure case report form on password-protected tablets or computers. Research assistants at each site will undergo rigorous training regarding study enrolment, data collection, retention and follow-up.
Screening and enrollment procedures
Research assistants will identify consecutive patients eligible for study enrolment in the days preceding discharge. During that time, research assistants will confirm inclusion and exclusion criteria for each potential participant who is admitted to the NICU or the paediatric ward. For consenting participants, key clinical findings and laboratory data will be documented in case report forms for factors present at admission and discharge (online supplemental files 2, 3). If no contraindication to study participation is found, a research assistant will approach the primary caregiver of the child and describe the study procedures. If the child is eligible and the caregiver consents to participation, informed consent will be obtained. The parent or guardian must provide informed consent prior to enrolment.
Supplemental material
Supplemental material
Research assistants will fill out case report forms on password-protected, encrypted software (Microsoft SQL in Tanzania and Kobo Toolbox in Liberia) with variables collected as part of the study. We will collect patient anthropometrics as measured during hospitalisation using standardised scales for weight, height/length as measured using available measuring boards and middle-upper arm circumference if documented by clinicians caring for children during their hospitalisation. We will calculate weight for height z-scores for age. We will collect data on documented nutritional status for the child during the hospitalisation (eg, severe acute malnutrition, kwashiorkor, etc).
Primary and secondary diagnoses at the time of admission and discharge will be collected by research assistants as documented. We will also collect information on any reported comorbidities (eg, HIV, tuberculosis, malignancies, etc) documented by the clinical care team. We will document the duration of hospital admission as documented in patients’ charts. Research assistants will ask caregivers about recent hospitalisations and document responses. Research assistants will record results from labs and imaging done during the hospitalisation, receipt of therapies including oxygen (ie, nasal cannula, face mask, etc), intravenous fluids and mode of receipt (ie, bolus, maintenance fluids, etc), medications (both type and duration) received during hospitalisation and procedures or surgeries performed.
As this is an observational study, we anticipate there will be some missing variables in clinical documentation. Research assistants will attempt to fill in any missing variables prior to discharge. Variables for individual participants still missing after the research assistants’ attempt to complete data will be accounted for with multiple imputations or excluded from analyses.
Research assistants will collect detailed contact information from the caregivers using a standardised patient locator form, including at least two working cell phone numbers for the caregiver, and a physical description of the whereabouts of the child’s home. If a caregiver does not have a mobile phone, we will obtain the mobile phone information of a household member or friend. We expect fewer than 5% of participants to be without cell phone access.
Follow-up visits
Research assistants will make phone calls to each caregiver of children at 7, 14, 30, 45 and 60 days after hospital discharge to ascertain the child’s vital status and to ask about health-seeking behaviours (online supplemental file 4). The equivalent of US$1 will be transferred via local phone companies to each participant for each follow-up phone call. Text messages will be sent to caregivers who do not answer the phone.15 If caregivers are still unreachable, research assistants will conduct home visits. Participants whose caregivers are unreachable despite three phone calls, two text messages and a home visit will be classified as lost-to-follow-up.
Supplemental material
At each telephone or in-person contact, a research assistant will ask the caregiver about the following and record the responses:
The child’s status (ie, well, ill, hospitalised, dead).
Any intercurrent illnesses.
Any clinic or emergency department visits since hospitalisation.
The caregivers’ seeking of other forms of treatment (ie, herbs, pharmacy, etc).
Reason for returning to clinic (eg, fever, vomiting, etc).
Caregivers will be asked by study staff to take their child to a clinic or hospital if they feel their children are severely ill between phone calls. For patients who are found to have died at home or in hospitals other than Muhimbili National Hospital and John F. Kennedy Medical Center prior to follow-up phone calls, research assistants will conduct home visits to use the WHO’s 2016 Verbal Autopsy Tool16 (online supplemental file 5) used to describe the death of a child outside of the formal healthcare system.17 18 Home visits will be arranged at a time convenient for caregivers and with adequate time after the child’s death to allow the family to mourn as is culturally appropriate. Research assistants will bring a contextually appropriate condolence gift (eg, a bag of rice) to caregivers of the deceased child. All research staff who will conduct home visits will undergo rigorous training in use of the WHO’s 2016 Verbal Autopsy Tool.
Supplemental material
Quality assurance
A study coordinator will be employed to assure that training of the field staff is high quality and rigorous. A data manager will generate weekly data summaries showing recruitment progress, follow-up and event rates to ensure high-quality and complete data reporting. These quality assurance approaches will be reinforced by each site’s principal investigator and by collaborators from the USA. Data cleaning will be performed using consistency and range checks. Data quality checks will also be applied weekly, and feedback will be provided to the study coordinators at both sites.
Outcome measures
Our primary outcome of postdischarge mortality and secondary outcomes including hospital readmissions, unplanned clinic visits and other care-seeking behaviours will be measured by caregiver report during follow-up calls and in-person home visits.
Statistical analysis
All candidate variables will be selected a priori based on prior studies,7 19–22 modified Delphi studies of factors thought to be associated with postdischarge mortality in sub-Saharan Africa,23 24 and experience among the research team. For the derivation of the clinical prediction rules, we will use elastic net regression,25 including all candidate variables to assess the strength of the association of each candidate variable on postdischarge mortality. Associations with 95% CIs for adjusted ORs that do not cross one will be considered significant. To determine the weighted points assigned to each candidate variable, we will calculate the adjusted log coefficient of each candidate variable from the multivariable model, round it to the nearest 0.5, and then double the rounded log coefficients to form an integer.26–29 We will assess the performance of the clinical prediction rules through internal validation using bootstrapping methodology with repetitions and calculate the area under the receiver operating characteristic (ROC) curve.30–33
We will also externally validate the clinical prediction rules derived in Uganda9 and in Mozambique10 by calculating the sensitivity, specificity and positive and negative likelihood ratios of each score at ≥ each specified cut point as defined in these rules. We will also create ROC curves for each existing score. We will assess the association of clinicians’ estimated probability of postdischarge outcomes and actual outcomes using ROC curves. We will use multivariable logistic regression to identify factors independently associated with 60-day hospital readmission and unplanned clinic visits among neonates and children. As previous studies suggest that healthcare seeking is infrequent among children who experience postdischarge mortality,34 35 we will review data from follow-up calls and verbal autopsies to calculate descriptive statistics of the proportion of caregivers who seek care in the postdischarge period and compare rates of care-seeking between children who die in the postdischarge period to those who survived.
Ethics and dissemination
This study received ethical clearance from the Tanzania National Institute of Medical Research, Muhimbili University of Health and Allied Sciences, the John F. Kennedy Medical Center Institutional Review Board and the Boston Children’s Hospital Institutional Review Board. We will disseminate our results in the form of scientific conference presentations and as peer-reviewed publications.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Juliana Mghambha, Mohamed Bakari, Dr. Nodermus Elias, Dr. Lawrence Kurwa, Dr. Tabu Mvile, Dr. Musa Malifedha, Veneranda Ndesangia, Naomi Mmbaga, Christina Japhet, Celestine Kagunila, Agnes Obed, Anna Fundi and Sarah Somji for their assistance in data collection and data management. We thank Melvin M. Kabba-Kay and Fidelis Njokanma for their support of this study. We also thank the nurses and nurse supervisors who have contributed to data collection at both Muhimbili National Hospital and the John F. Kennedy Medical Centre.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KPM and CPD are joint senior authors.
KPM and CPD contributed equally.
Contributors All authors contributed to the study conceptualisation, the study design, sample size calculations and writing of the protocol for this study. CAR, KM and CD prepared the first draft of the paper. All authors contributed to revisions of the manuscript and contributed to the revision of the final manuscript. All authors have read and approved the final manuscript.
Funding This work was supported by the National Institutes of Health (K24 DK104676and P30 DK040561 to CPD), the Boston Children’s Hospital Global Health Program to CAR and the Palfrey Fund for Child Health Advocacy to CAR.
Disclaimer The funders had no role in the study design or in the collection, analysis, or interpretation of the data. The funders did not write the report and had no role in the decision to submit the paper for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.