Article Text

Abstract
Background Burn is a major cause of childhood injury-related morbidity and mortality. Global estimates suggest that 90% of all cases occur in low-income and middle-income countries and over half of the disability-adjusted life-years are lost from fire-related burns in children. In Bangladesh, there is a scarcity of data on childhood burn injuries. The goal of the study was to describe the epidemiology of non-fatal burns in Bangladeshi children, including incidence estimates and identify high-risk groups.
Methods Bangladesh Health and Injury Survey 2016 was a large scale cross-sectional survey. The survey was conducted among 299 216 population utilising a multistage cluster sampling method. Among the 100 842 children, there were 437 non-fatal burn cases.
Results Among different injury mechanisms in children, burn was ranked fifth (7.4%). The overall yearly incidence rate (IR) of burns was 866.7 per 100 000 children (95% CI 785.6 to 947.8) in Bangladesh. The incidence was highest among 1–4 years old children (IR 2028.3, 95% CI 1761.1 to 2334.7) and had a 3.5 times higher risk of burns compared with the 15–17 years age group. Females had a much higher IR of non-fatal burns than males between the ages of 10–15 years (1655.2 vs 482.2). About 70% of burns occurred in rural areas. Hot liquid (44.7%), flames (32.5%) and hot objects (20.7%) were identified as the main causes of burns. The kitchen (60.9%), yards (20.8%) and bedroom and living room (10.5%) were the three most common places for burns. According to the study, 34.8% of burn incidences occurred between the hours of 7:00 and 10:00.
Conclusion Children in Bangladesh suffer from a high rate of non-fatal burns. The high-risk category was identified as preschool-aged boys and adolescent girls. The majority of the incidents occurred in the morning and inside the kitchen. These findings will help raise awareness and create intervention measures to reduce the high incidence of non-fatal childhood burns in Bangladesh.
- Epidemiology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
About 90% of childhood non-fatal burns occur in low-income and middle-income countries.
More than 90% of burns in children happen in the home environment, mostly in the kitchen.
Children from rural areas are more likely to sustain burns than urban children.
WHAT THIS STUDY ADDS
According to estimates, around 500 000 children in Bangladesh suffer non-fatal burns each year.
Preschool children in rural areas were at high risk of burns. Hot liquid is the leading source of non-fatal burns in Bangladeshi children.
Adolescent girls were shown to be at a high risk of burns due to their involvement in cooking.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study will facilitate the development of future implementation and intervention of burn prevention research in Bangladesh
The study findings will help build community awareness and thus improve the burn prevention behavior and practice at the community level
It will add value to the national burn injury prevention strategy in Bangladesh
Background
Burn injuries are a major public health concern, which cause significant morbidity and mortality across the world.1 2 Every year, around 300 000 people die from this devastating form of injury, 90% of them from low-income and middle-income countries (LMICs), where two-thirds of them occur in the African and South-East Asia regions.3 Despite WHO’s repeated outcry for attention and persistent call for action, limited progress has been made in LMICs, including Bangladesh to reduce the risk of burns that takes away an estimated 9000 lives annually.4 This burden is disproportionately higher in the younger population (40% of the total population) and WHO estimated nearly 173 000 Bangladeshi children suffer from moderate or severe burns every year.3
Mortality among burn patients is high in Bangladesh, and recovery from less severe injuries is usually very slow and difficult.5 6 Burn injuries in children are usually more traumatic and their burden always extends out to the family members.7 In Bangladesh, Colombia, Egypt and Pakistan, 17% of children with burns result in temporary disability and 18% have a permanent disability—according to one study.3 About a quarter of all burn injuries have been documented to afflict children who are under the age of 16 years; many victims are quite young and are under the 5 years age bracket.8
Progress has been made in high-income countries to reduce the morbidity and mortality associated with burn injuries. However, many of these advances in clinical care and rehabilitation have not reached Bangladesh and most other LMICs, even though nearly 90% of all burn injuries occur in LMICs.3 With very few specialised burn management centres and trained professionals, management of severe burns is challenging in Bangladesh.9 Globally, limited population-based epidemiological survey data on burn injury are available, and information on burn injuries is mostly documented from hospital-based surveys. Previous studies have suggested that age, sex and residence are key predisposing factors for children to sustain burn injuries.10 11 Furthermore, understanding the high-risk activities that result in burns, as well as the most prevalent sites where burns occur, provided vital insights on how to avoid as many burns as possible.
Bangladesh is undergoing an epidemiological transition, with injuries now outnumbering infectious diseases as the leading cause of childhood mortality.12 Despite the high incidence of non-fatal burns in Bangladesh, very few research studies have been attempted to characterise the nature, aetiology and risk factors comprehensively. The most recent burn injury study was almost two decades ago, and new evidence on childhood burns in Bangladesh is crucial for developing the most up-to-date evidence-based interventions. The goal of this study is to describe the epidemiology of non-fatal childhood burn injuries from a large survey and to identify the high-risk population, with the expectation that the findings will serve as a guide to raise awareness and develop intervention strategies to reduce the burden of childhood burns in Bangladesh.
Materials and methods
Bangladesh Health and Injury Survey (BHIS) was a community-based large scale cross-sectional survey conducted between March and June 2016. The survey used a multistage cluster sampling strategy based on probability-proportion-to-size methodologies with separate urban and rural samples. Among 64 districts of Bangladesh, 16 were randomly selected. From each district, one Upazila was randomly selected for the rural area. The village (comprised around 300 households) was considered a cluster and 100 villages were selected from each Upazila, whereas 80 households were selected from each of the villages. For the urban area, a systematic sampling technique was adopted to attain the required number of households from mohallas/ward (cluster). Mothers were preferred as respondents for children, if not available, caregivers were interviewed. For injury morbidity, a 6-month recall period was considered. To minimise the recall bias, data collectors encouraged the other responsible family members to ensure the injury incidence. Sixty-four trained data collectors and 16 experienced supervisors were involved in this survey. Data were collected in REDCAP (Research Electronic Data Capture) software. A total of 350 000 population were scheduled for the interview and 333 000 community people were reached. The details on sample size calculation have been provided in online supplemental file. After cleaning and validation, data from 299 216 respondents were available for the final analysis. Among the populations covered, 198 374 were adults (≥18 years) and 100 842 were children (0–17 years). Descriptive statistics were used to present the sociodemographic characteristics of respondents. Non-fatal burns were stratified by age groups, sex, and residence, and yearly incidence rates were calculated. All rates were multiplied by 2 to present a yearly estimate as a 6-month recall period was considered. To compare the burn risk in different age groups, sex and residence, the incidence rate ratio (IRR) was calculated. In all estimates, a 95% CI was considered. Injury place, time and item responsible for burns were presented using the descriptive table and graphs. Microsoft Excel, Open EPI-Info software and SPSS V.23 were used for data analysis and representation. STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) statement was included by completing the STROBE checklist.
Supplemental material
Case ascertainment
Any male or female aged between 0 and 17 years who had a burn injury that resulted in a loss of 1 day of work, school or ability to care for him or herself was included as a case of non-fatal burn injury.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
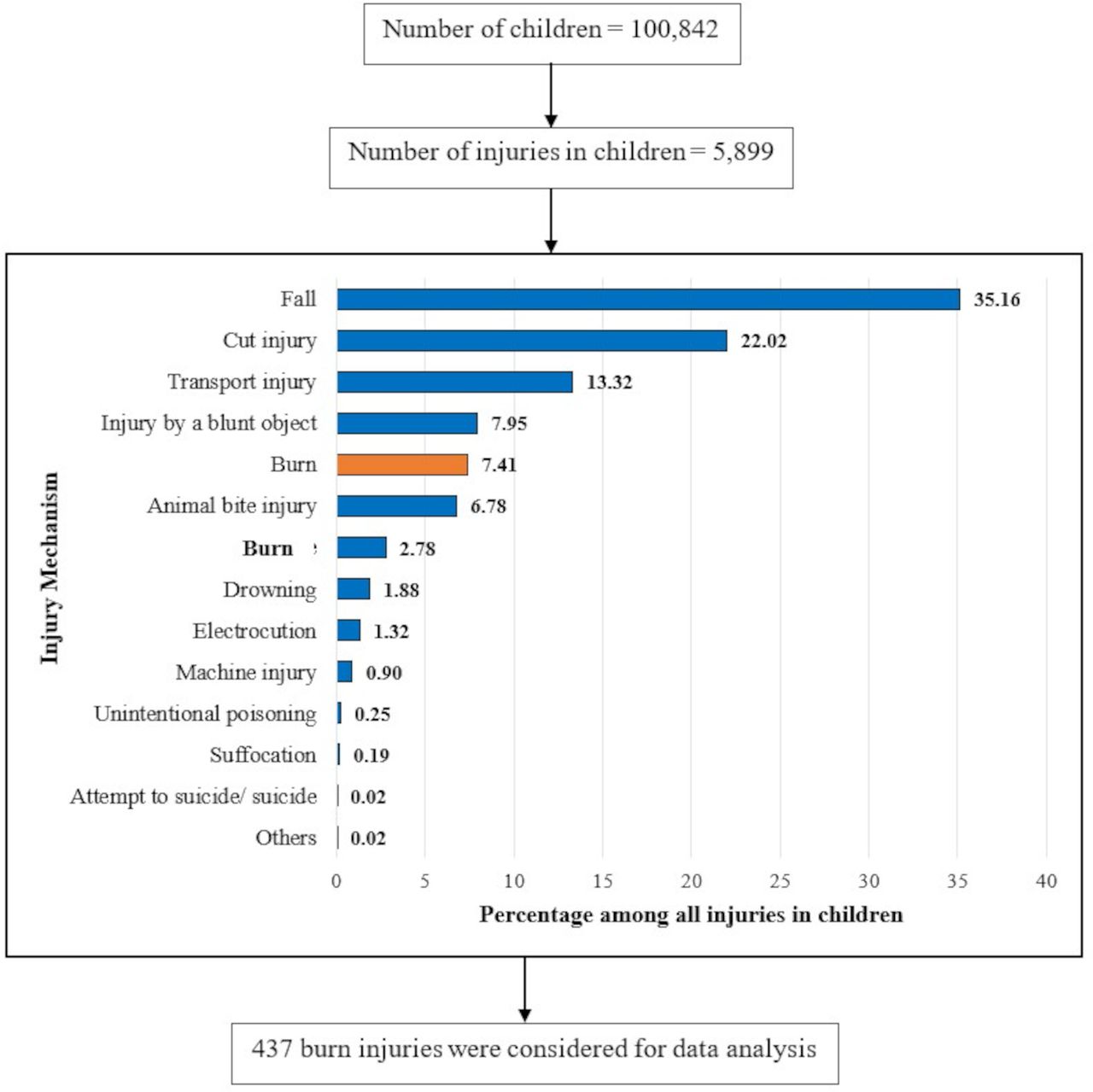
From figure 1, the households reported 5899 non-fatal injuries among 100 842 children. With 437 cases, burn injury was the fifth (7.41%) leading non-fatal injury among Bangladeshi children.

Flow chart presents the proportional distribution of burns among all non-fatal injuries.
Demographic characteristics of the respondent
The demographic features of the children are shown in table 1. The majority of the 100 842 children surveyed (31%, n=31 289) were in the 10–14 years age group, followed by the 5–9 years age group, which accounted for 28.2% of the total children. The infants (<1 year) represented only 3.7% (n=3749) whereas the 1–4 years and 15–17 years together contributed about 37% of the respondents. Male children (51.8%) topped female children by a small margin in the survey and approximately 67% of the children (n=67 264) were from rural areas of Bangladesh.
Sociodemographic characteristics of the study population
Distribution and incidence rate of non-fatal burns by age, sex and residence
The overall annual incidence rate of non-fatal burn among Bangladeshi children was 866.7 (95% CI 785.6 to 947.8 per 100 000 children per year). Age stratified data showed that the incidence rate of the burn was highest among the 1–4 years age group of children (IR 2028.3, 95% CI 1761 to 2334.7) contributing to 45.3% of the total burns. Six (1.4%) infants contributed to the total burns and had the lowest incidence rate with 320.1 non-fatal burns per 100 000 infants (95% CI 13.1 to 733.8). The 10–14 years and 15–17 years age groups combined contributed to about 28% of the total burns in children. The IRR presented in table 2 shows that the 1–4 years children had 3.5 (95% CI 2.61 to 4.82) times higher risk compared with the 15–17 years age group.
Incidence rates of non-fatal burns among children by age, sex and residence
Female children were 56.5% (n=247) of the total burn cases and had a 1.3 (95% CI 1.08 to 1.57) times higher risk of burns compared with the male children. The overall incidence rate in females was 1016.63 (95% CI 894.8 to 1153.3) per 100 000 children in a year. About 70% of burns occurred in rural areas. The children from rural areas were found to have a higher incidence rate (906.9) compared with the children living in urban areas (786.2).
When broken down by sex, the difference in terms of incidence rate becomes dramatic when female children become 10 years and above; their burn risk goes much higher; 720.3 vs 245.5 for males in the 10–15 years age group and 934.9 vs 237.1 for males in the 15–17 years age group. Infants and 5–9 years age group from the urban area had a higher incidence of burns compared with the rural area. On the other hand, residential variation (rural vs urban) was not significant in this study (table 3).
Age distribution of the injured children by sex and geographical location
Sources of non-fatal burns in children
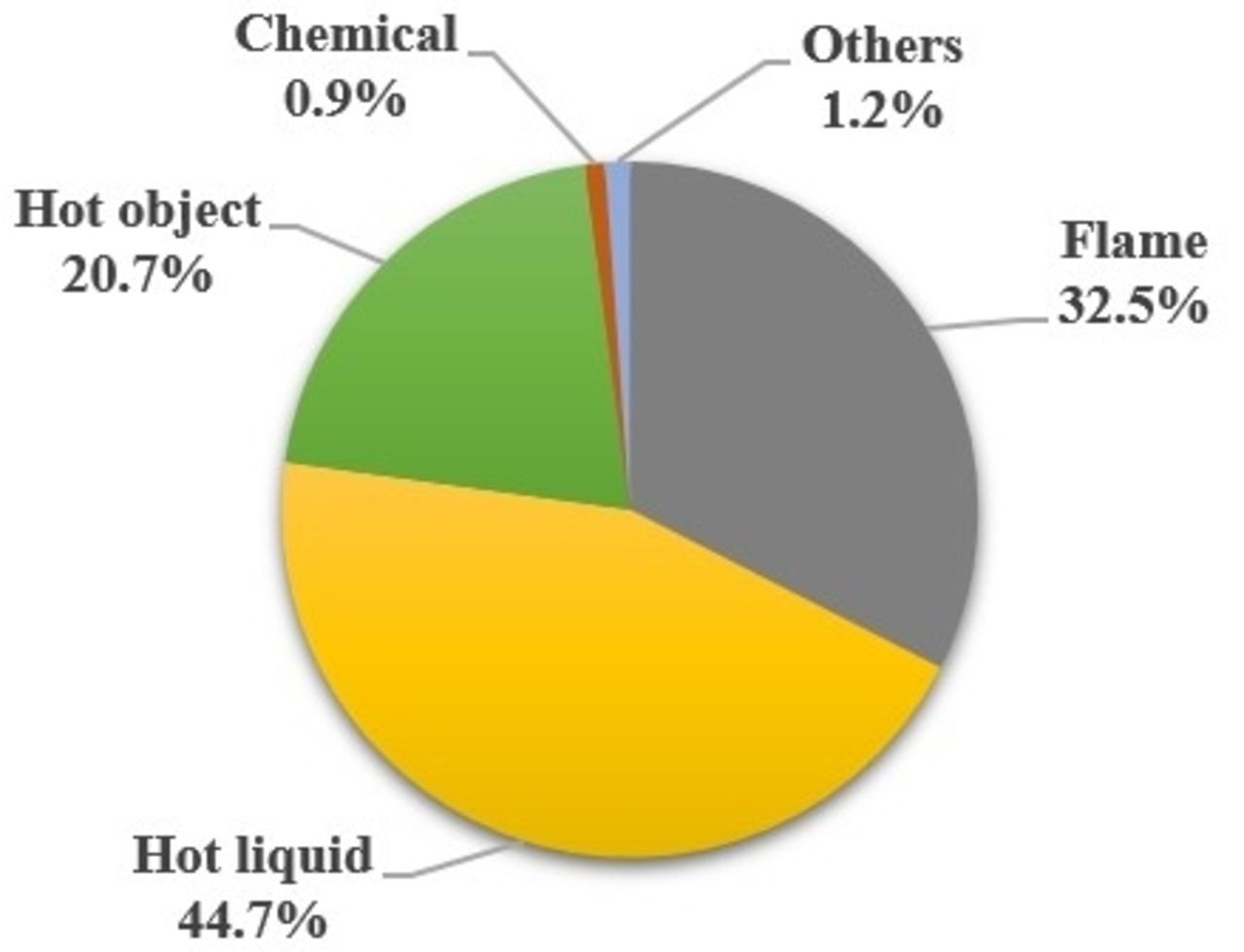
Figure 2 presents the source of non-fatal burns among children in Bangladesh. Hot liquid (44.7%), flames (32.5%) and hot objects (20.7%) were identified as the main causes of burns among children. There were 194 burn cases from hot liquid, where females sustained about 60% of the injuries. About 36% of injuries were from soups or liquid foods followed by cooking oil (23%) and water (20%) as the hot liquid sources. Among the 141 (32.3%) burn cases that were caused by flames, 105 (74.4%) occurred from cooking fire (wood, leaf, cow dung). Females contributed about 56% (n=82) of burns cases due to cooking fires. About one-fifth (n=90) of the total burns were sourced from hot objects, mostly from cooking utensils and coal (60%). Male sustained more burns (52%) than females from the hot object. Only 1% of the total burns were sourced from chemical objects (n=4) (online supplemental file).
{kind=link}
{kind=link}
Source of non-fatal burns in children.
Place of childhood non-fatal burns
Table 4 depicts the places where non-fatal burns among children occurred. The three most common places were the kitchen (n=266, 60.9%), yards (n=91, 20.8%) and bedroom and living room (n=46, 10.5%). Gender differential showed, for males, 52.6% occurred in the kitchen, 24.7% in yards, and 11.1% in the bedroom and living room whereas for females, 67.2% occurred in the kitchen, 17.8% in yards and 10.1% in the bedroom and living room.
Places of non-fatal burn by gender among children in Bangladesh
Infants sustained an equal number of burns in the kitchen and bed/living room. Kitchen was the prominent place for non-fatal burns with 60%, 50% and 65% of the burns cases occurring here among the 1–4 years, 5–9 years and 10–14 years age groups, respectively. Yard was the second most prevalent place accounting for 25% of the total burn cases among 1–9 years children, and 20% of the burn cases among 10–14 years children. Among the 15–17 years children, above 80.0% of burn injuries occurred in the kitchen (online supplemental file).
Time of occurrence for childhood non-fatal burns
The majority of injury incidences occurred between the hours of 7:00 and 10:00, accounting for 34.8% of all incidents. About 31% (n=135) of the burn occurrences among children occurred between 11:00 and 14:00 hour, during the time when lunch is usually prepared. Furthermore, 86 (19.7%) of the burn incidences were in the evening (15:00–18:00 hour). Between the hours of 7:00 and 18:00, 373 (85.4%) non-fatal burns occurred. About 15% (n=64) burns occurred at night. The results are given in online supplemental file.
Discussion
Our goal is to use data from a large population-based survey to investigate the current epidemiological distribution of non-fatal burn injury in Bangladeshi children. In both the BHIS 2003 and the BHIS 2016, the burn injury was placed fifth among all injury mechanisms in children.13 Every year, more than 500 000 children in Bangladesh suffer non-fatal burns, according to our estimates.
Children under the age of 5 accounted for nearly half of the total cases in this study, making them the most vulnerable category. The finding is consistent with previous BHIS conducted in 2003, but the incidence rate was three times higher in 2016.13 However, the rate of burns in 2003 was much lower as the study considered different operational definitions for the case ascertainment. Studies conducted in rural Bangladesh such as the SoLiD project and two others in urban slum dwellers also demonstrated that this age group is the most vulnerable.14–16 This age group was also found to be vulnerable in epidemiological studies conducted in other developing countries such as India, Sri Lanka, Pakistan and Taiwan.17–20 This high number of burns in children under 5 years of age was largely due to their ability to start walking and wandering around and trying to become gradually independent from their parents.
The study found an overall higher non-fatal burn incidence among females than male children. Male children, on the other hand, had a greater incidence according to BHIS 2003. Furthermore, the female incidence rate in older BHIS data was around three times lower than that in contemporary BHIS data. However, several studies around the world found similar female multitude,13 21–23 while some other studies produced disagreeing findings as well.24 25 When broken down by sex by age groups, the difference becomes dramatic when female children become 10 years and above; their burn risk goes much higher than same aged males. The increasing trend in their adolescence is probably because they start to engage in the kitchen environment and their lack of knowledge on how to handle flammable substances.
The kitchen, as expected, has been identified as the leading source of burn injury to children in the home, followed by the yards (20.80%) and the bedroom and living room (10.5%). Results had a similar pattern to the previous BHIS 2003 survey.13 26 The similarity was also found in many study outcomes in diverse regions.27–30 Other places had little contribution to burn injuries among children. Lack of supervision by mothers and caregivers, especially in rural areas might be one of the possible factors behind this. Toddlers’ frequent movement in the kitchen and touching hot materials kept in sight of them is an additional possibility. Safety measures in the home environment are important which is mostly lacking in LMIC settings,31 in general, correlated with lower educational status among caregivers.32 Various burn sources are exposed in Yard, which is largely in a rural area where children play. Because small children generally stay at home, there were few incidents outside of these two areas. These were all unintended injuries, it is possible that a lack of caution and monitoring is to blame for burn injury.
In Bangladesh, a different pattern of non-fatal burns was seen in both rural and urban areas. In total, 69% of burns occurred in rural regions, and rural children were shown to be at higher risk in every age category, with an overall incidence rate of 906.87 per 100 000 per children years. Most studies reported a higher incidence of burns in rural areas.33 34 In LMICs, the increased incidence of burns among children in rural area is common, specifically from fire-related burns. In another study, Poverty, low education of parents, and poor infrastructure of the housing were found to be the cause of burns.35
Hot liquids were the most common cause of harm, with girls suffering more burns than males in the majority of cases. These findings matched those of studies undertaken in many countries and a WHO report.36–38 Females when they become 10 years and above, start to engage in cooking with or without their mothers’ presence or supervision, and injuries from hot liquid and hot objects are common among this group. In Bangladesh, boiling rice water in the yard and boiling water for bathing in the winter often spill on young children. Mothers often keep hot food plates near the children’s sight. WHO reported that a large number of child burn injuries occur from flame.3 In Bangladesh, open space cooking practice in rural areas with wood, dry leaf and cow dung often produces uncontrolled flames which cause a substantial number of burns in children.
Strength and limitations
This was the largest community-based injury study in a low/middle-income country in the recent decade, and it represents large-scale estimates of injury-related morbidity. This large-scale community-based survey also assisted in controlling for biases found in facility-based surveys, such as reporting bias, age group bias and socioeconomic status bias. The study, however, had some limitations. Because the responses were collected over a 6-month period, there was a risk of recollection bias, and some mild to moderate burn cases may have gone unnoticed. To reduce recollection bias, parents were urged to talk to other family members while documenting the burn incident. Another source of potential bias is in the estimation of annual non-fatal burns incidence rates from 6-month recall data, which was calculated by multiplying the 6-month rate by 2.
Conclusion
Burns were found prevalent among Bangladeshi preschool children. Female children are more likely to suffer non-fatal burns, and the risk increases as they get older. This research reveals a gap in prevention measures that must be addressed in order to lower the risk of particular burns in children. Future studies should focus on the causes and severity of burn injuries, as well as the progress of burn prevention strategies and the development of appropriate interventions to reduce burn injuries.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethical Review Committee of Centre for Injury Prevention and Research, BangladeshERC Reference Number: CIPRB/ERC//2016/005. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We acknowledge the Directorate General of Health Services (DGHS) for funding and technical support. The manuscript was prepared as an academic exercise (Thesis) during Master of Public Health (MPH), and sincere gratitude is due to the thesis supervisor, and academic mentors of the Department of Public Health, North South University, Bangladesh.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MA: Conceptualized the manuscript, analyzed data, interpreted results, and drafted the manuscript; SRM: Designed the study, implemented the study, oversaw the quality control measures, guarantor of the study and reviewed the manuscript; FNR: Interpreted results, and assisted in drafting the manuscript; SR: Interpreted results, and assisted in drafting the manuscript; FR: Designed the study, oversaw the quality control measures, and reviewed the manuscript; AH: Interpreted results critically, conceptualized the manuscript, guided manuscript writing, and critically reviewed it;
Funding The study was funded by the Directorate General of Health Services (DGHS), Dhaka, Bangladesh.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.