Article Text

Abstract
Objective To assess variation in current practice of initial health assessments (IHAs) for unaccompanied asylum-seeking children (UASC) across England.
Design Cross-sectional survey.
Main outcomes measures Type of routine assessment carried out, threshold to specialist referrals and facilities available to complete IHA.
Results Eighty-six health professionals responded across England; 47% had received training in UASC IHA and 33% in UASC mental health issues. The majority (80%) of IHAs were conducted with translator support and 7% of participants reported Child and Adolescent Mental Health Services (CAMHS) input. Around half of clinicians (53%) performed tuberculosis and bloodborne virus screening for all UASC, while other infectious diseases (IDs) screening was symptom and risk factor dependent. Overall, 14% of clinicians routinely comment on age assessment and 76% share the IHA report and health plan with UASC. The time allocated for assessment range between 30 and 90 min.
Conclusion There is significant variation in practice around UASC IHAs across England, notably around CAMHS input, time allocated, translation facilities and ID screening. The results suggest that, an increase in resources available for UASC teams, improved access to specialist services and further training on UASC health are all needed. Guidance that aims to set a best practice framework for UASC IHA delivery such as a ‘one-stop shop’ model would help to standardise UASC IHA across the country.
- adolescent health
- epidemiology
- health services research
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Unaccompanied asylum-seeking children (UASC) frequently have complex physical and mental health needs due to trauma and violence, poor access to healthcare, family separation and their inherent vulnerabilities as children.
Initial health assessment (IHA) should include a holistic comprehensive health review of current and past health needs to set out an action plan.
What this study adds
We found variety in what health screening is routinely offered to UASC during IHA and who is involved in supporting them.
Professionals involved in IHA need further training and education on UASC and their health needs.
How this study might affect research, practice or policy
Our findings should encourage further research on UASC health needs and outcomes, to inform further health system strengthening strategies in this area.
Policy makers, practitioners and researchers should work with UASC themselves to build a best practice framework to deliver appropriate joined-up care
Introduction
From June 2020 to June 2021, the UK received 2756 applications for asylum from unaccompanied children.1 Unaccompanied asylum-seeking children (UASC) enter a country to claim sanctuary on the grounds of persecution in their country of nationality. The majority of UASC arriving in the UK originate from Sudan, Afghanistan, Eritrea, Iran and Vietnam.2 Latest figures from the Office National Statistics report that 92% of UASC are male and 13% are aged under 16.
After arrival in the UK, UASC are taken into the care of a local authority and become ‘looked after children’ (LAC). UASC represent 5% of all LAC in England.3
UASC are entitled to the same local authority support as other LAC. This includes access to a safe and stable placement and the care they need to promote their welfare and fulfil their educational potential.4 5 Local authorities are also responsible for their health and well-being, which includes a thorough health assessment. This statutory initial health assessment (IHA) should be carried out within 28 days of the child being registered with the local authority.6
Health needs of UASC
UASC frequently have complex physical and mental health needs due to trauma and violence, poor access to healthcare, family separation and their inherent vulnerabilities as children.7 8 Following arrival, language and cultural differences act as barriers to engagement with health services, which may be further exacerbated by stigma and discrimination in healthcare.9
Lack of routine data on UASC health across the UK limit research on health outcomes of this group.10 As a result, surveys of health services are needed to evaluate UASC health needs further.
Pathways for UASC health assessments
There is a lack of guidance, education and best practice examples on management of UASC, especially regarding how their IHA should be carried out.11 Anecdotal evidence highlights that many teams follow local procedures depending on the resources available, and the capacity of specialist services such as paediatric infectious disease (ID) or CAMHS teams in the area.
Previous audits exploring UASC health services highlighted concerns regarding delays in accessing IHA appointments, as well as issues with appropriate screening offered and follow-up arranged.12 13
To inform future practice, it is vital to understand what services are currently being delivered. We therefore aimed to survey current practice of IHAs for UASC across England with a view to describe variation in care and identify targets for intervention and standardisation. Secondary aims were to inform policy recommendations and future UASC health research.
Methods
We designed an online survey to explore how IHAs for UASC are carried out across England. A questionnaire was developed iteratively and piloted across two local authorities. Potential participants were identified from the membership of national colleges and associations including, British Association for Community Child Health and Royal College of Paediatrics and Child Health. Any healthcare professional involved in UASC IHAs in England could participate. The survey was open to multiple members of the same team to try to capture the multidisciplinary team experience.
We collected key information on the IHA process, including multidisciplinary team involvement and routine screening carried out. The final survey contained 57 questions across five sections: (1) demographics, (2) health system, (3) IHA process, (4) training and (5) current situation. Response format included multiple selections, single answer, free text or 5-point Likert-scale options. Online supplemental file 1 includes a copy of the survey. The online survey was distributed using Qualtrics software V.04/2021. Respondents were invited to participate via email and social media. Data were collected from March 2021 to June 2021.
Supplemental material
For survey responses to be taken onto the analysis stage, over 75% of the survey must have been complete. Descriptive analysis was performed using R software V.4.0.3.
Patient and public involvement statement
No patients or members of the public were directly involved in the design of the study.
Results
Participant’s setting
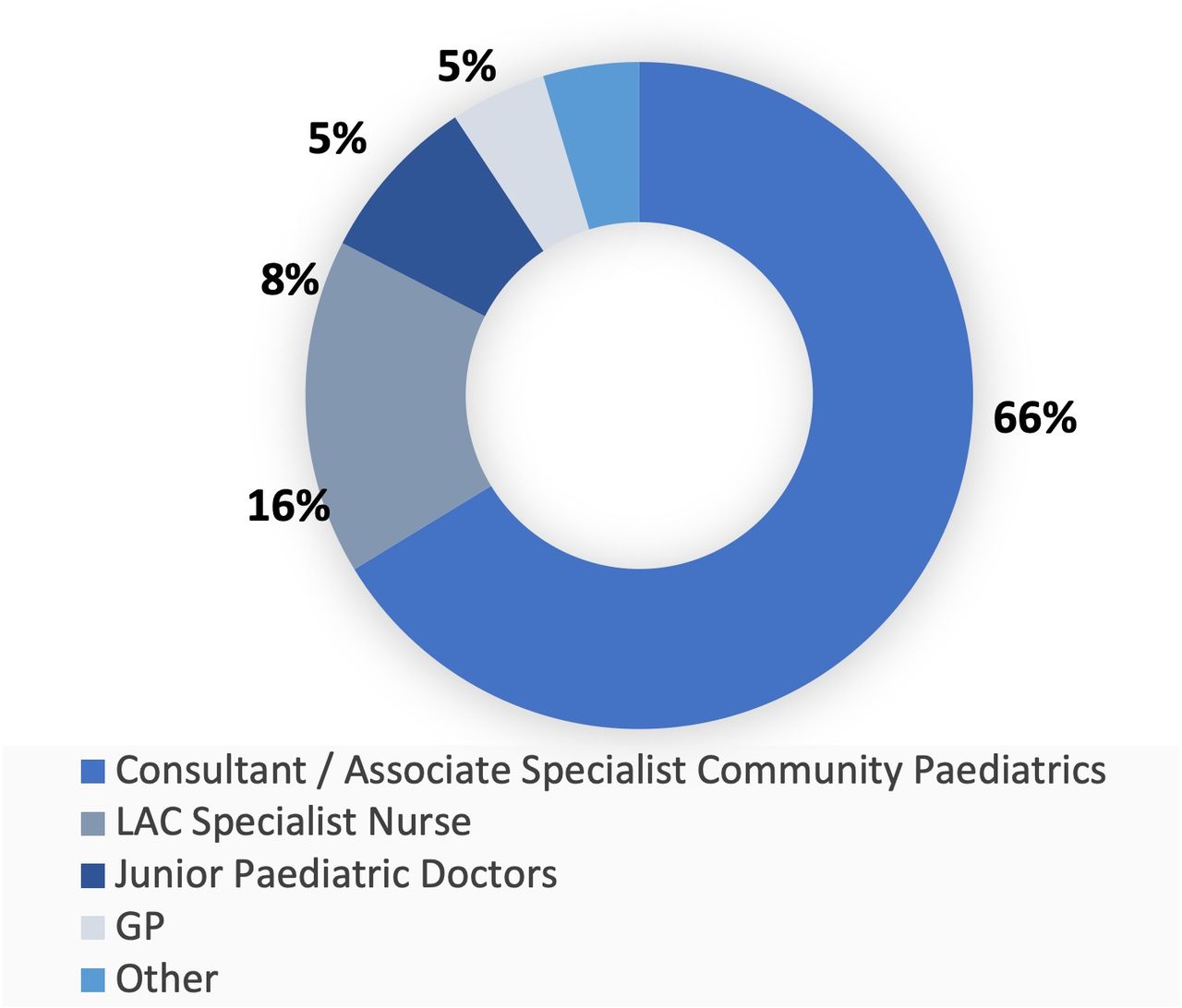
Overall, 86 responses were included in the analysis from 84 local authorities and boroughs across England (figure 1). A wide variety of members from the multidisciplinary team completed the survey, including consultant community paediatricians and specialist nurses in LAC. figure 2 summarises the roles of the survey participants. Designated doctors or nurses for LAC made up 42% of the respondents.

Catchment areas (blue) of LAC teams participating in the survey
{kind=link}
{kind=link}
Profile of survey participants
Initial health assessment (IHA)
All healthcare professionals reported making use of available regional and national guidelines, having local guidelines in place or using a combination of these. ‘RCPCH: refugee and UASC and young people—guidance for paediatricians’ was the most common referenced guideline (57/86, 66%) together with UASChealth.org (47/86, 55%) and public health england: migrant health guides (16/86, 19%). A small number of participants reported using local guidelines (8/86, 9%) and 1 participant reported using the ‘caring for kids new to Canada’ guideline.
The Coram-BAAF Form IHA-YP (54/86, 63%) was most frequently used to document the IHA. Some participants reported using a local proforma to document this clinical assessment (27/86), while a minority used the Kent UASC Proforma (5/86).
There was significant variation in the time allocated to carry out UASC IHA. The majority of IHAs took between 30–60 min (37/86, 43%) and 60–90 min (39/86, 45%) and a minority allocated over 90 min for this consultation (10/86, 12%).
In-person translation services were the preferred interpretation option (77/86, 90%), with a small number of participants using other facilities such as language line (8/86, 9%), video interpreter (3/86, 3%), relatives or foster family members (7/86, 8%) or members of staff (1/86, 1%).
Approximately, half of participants reported that when no in-person interpreter was available the IHA appointment would be carried out using alternative options (44/86). However, some participants report that in these instances they would cancel and reschedule the IHA once (15/86) or more than one (19/86).
Most participants worked in teams with no health improvement practitioner or equivalent position, responsible for liaising with UASC and multidisciplinary team to increase engagement and reduce the ‘did not attend’ rates for appointments (71/86). Similarly, in most cases, participants reported that child and adolescent mental health services were not present during this initial assessment (80/86).
IDs screening
Asymptomatic screening of tuberculosis disease (TB) and bloodborne viruses (BBV) was the most common ID screening carried out (46/86, 53%). The level of screening for other IDs was hugely variable from teams who would perform routine asymptomatic screening for sexually transmitted infections (11/86, 13%) and helminth infections (11/86, 13%) to participants reporting no routine screening in place (6/86, 7%), or screening only if symptoms were present (2/86, 3%). A smaller proportion risk assessed to determine what IDs screening was offered in asymptomatic UASC (22/86, 26%).
There was significant variation in who carried out the IDs testing; most commonly general practitioners, general paediatricians or ID paediatricians were responsible (58/86). A minority of participants reported offering ID screening during the IHA itself (21/86,).
The range of infections screened for varied between services, these are summarised in table 1.
Infectious disease screening test offered depending on universal screening or risk-based screening used
Mental health
Most participants reported screening for mental health problems using direct questioning in the history (76/86, 88%), but participants also reported using a variety of formal mental health screening tools during IHA (table 2). The strengths and difficulties (SDQ) was the most frequently used tool to screen for mental health. However, few participants reported the SDQ being completed prior to IHA (15/86, 17%).
Commonly used strategies to screening for mental health problems
Some participants reported routinely signposting to mental health services, either CAMHS (25/86, 29%), third sector services (12/86, 14%) or both (23/86, 27%). However, some respondents did not routinely signpost mental health services in the area (26/86, 30%). Access to a mental health MDT meeting to discuss complex patients was limited within the sample (28/86, 32%).
Sexual health
Most participants reported routinely asking about sexual health during the IHA (77/86). The majority of clinicians would carry out sexual transmitted infection testing if perceived to be required (72/86); while a small number of teams offered sexual health testing routinely (5/86). Regarding the concept of ‘consent’ for sexual activity, most teams provided education on this during the assessment or arranged for this to be done in another setting (52/86, 60%). Direct questions about female genital mutilation were asked about by 61/86 (71%), and 56/86 (65%) explicitly asked UASC whether they had been sexually assaulted or abused in the past.
Most participants routinely signpost young people to sexual health clinics offering walk-in services (59/86), with fewer directing UASC to appointment-based clinics (11/86) or not signposting to sexual health services (16/86).
Family and relationships
In many cases, participants would take a comprehensive family history of immediate relatives (49/86, 57%), but fewer cases included distant relatives (36/86, 42%). Most participants report routinely asking whether UASC were in contact with their family (79/86, 92%) and the majority offered contact tracing services such as British red cross family reunification (59/86, 69%).
Onward referral from IHA
The most frequent referrals reported were to dental (77/86, 89%) and ophthalmology services (77/86, 87%), which are recommended to be carried out as routine. IDs (52/86, 60%) and CAMHS referrals (49/86, 57%) were less common, as were sexual health (40/86, 46%) and hearing assessments (39/86, 45%).
Staff training
Around half of the survey participants reported attending specific training in UASC IHA (41/86, 46%). A smaller proportion had received training on mental health assessment (29/86, 33%). When training had been completed, this was 30–120 min in duration and carried out locally, for example, during induction (38/41, 92%). Participants also received training through modules in e-learning for healthcare (13/41, 32%) regional and national RCPCH training events (9/41, 22%), during conferences or from CoramBAAF (2/41, 5%).
Discussion
We present responses from across 84 local authorities and London boroughs in England describing the routine UASC IHA carried out. We found that IHA usually takes between 60 and 90 min with language interpretation services provided in-person or via phone (language line). The findings suggest that testing for IDs is more likely to be carried out in symptomatic UASC and those with risk factors for infections, as opposed to routinely on all newly arrived UASC. Routine asymptomatic testing aimed to identify TB and BBV, whereas testing for sexually transmitted infections or helminth infections was dependent on risk factors or symptoms being present. Overall, we found that most participants had limited training and reduced access to mental health services. Participants indicated a desire for further training on UASC health.
The current literature highlights several guidelines and documents available to UK professionals, which detail the main requirements of IHA for this vulnerable group. Current national guidance does not set a minimum quality standard for UASC health services and although international frameworks describe what best practice should look like, they are not widely referenced or used.14 Best practice evidence on comprehensive IHA to address and meet the complex of UASC is scarce with few articles describing the local pathways in place to ensure that IHAs identify and address the needs of this vulnerable population.12 15 16
The European Centre for Disease Prevention and Control guidance on the communicable disease screening for migrants including migrant children17 and the Canadian Paediatric Society web resource, ‘caring for kids new to Canada’ includes comprehensive information for health professionals.18 However, no international consensus exists when it comes to the holistic approach to UASC health assessment, an especially vulnerable groups with risks different to those of non-asylum-seeking migrant children.
This survey explored current practices in place to deliver IHAs to UASC across England. The survey was constructed iteratively, was available for an appropriate amount of time and was easily accessible to allow for diverse distribution across the networks. However, a key limitation is that as many responses did not reach the 75% minimum target completeness to be used in the analysis stage, useful data may have been lost. Prospective participants may have found the length of the survey a barrier to participation. As with all cross-sectional survey studies, the sample included may also represent those teams that believe they have an appropriate IHA system in place and so are willing to share details of their practice. To minimise this potential selection and recruitment bias, we ensure that respondents knew responses would be anonymised at analysis stage so that we could not link responses to a particular local authority.
We present evidence of the need for improved guidance and education on routine assessment of UASC. Service standardisation, together with best practice guidance, would help to reduce the variation in practice and reduce the disparities in health outcomes that may consequently occur
The results highlight a clear need for further training being available to professionals working with UASC to ensure that they have the right skills set to address their complex health needs, including assessing and managing mental health problems. In addition, we believe that there is a clear need to improve the resources available to teams across the country and both central government and local authorities should ensure work together with LAC health teams to ensure that appropriate facilities and resources such as in-person interpreting and access to specialist members of the multidisciplinary team are available.
We advocate for LAC teams to implement a ‘one-stop shop’ IHA model that meets proposed framework of best practice in management of newly arrived refugee children14 using a multidisciplinary approach to the holistic care needs of UASC during a single healthcare episode. Box 1 details a proposed ‘one-stop shop’ model. We also believe that a platform that encourages service user participation in health service planning is key to improve health outcomes. Patient surveys and focus groups can empower children and young people to express their views and wishes regarding their health needs and how these should be met. Their voice should be central to design and development of new services.
Proposed ‘one-stop shop’ model
Comprehensive Multidisciplinary Team (MDT)-led approach to health assessment of migrant children.
Community paediatrics/looked after children teams should coordinate a holistic and comprehensive health assessment service that is culturally and linguistically appropriate. The service should be designed in consultation with service users and a mechanism to obtain regular feedback should be in place to ensure children and young people participation in service development.
The initial health assessment (IHA) should take place in a ‘one-stop shop’ model, whereby health needs are identified, and initial investigations are carried out.
We advocate for specialist input during the IHA, including presence of Child and Adolescent Mental Health Services (CAMHS), paediatric infectious diseases and community sexual health as well as dietetics to guide most appropriate management.
We believe a one-stop shop model will facilitate care coordination, ensure accessibility whilst integrating physical, developmental and psychosocial health needs. In addition, this service model will reduce the number of follow-up appointments required, something that can lead to them being loss to follow up.
We also recognise that this approach to initial health assessment has disadvantages especially as specialist teams may have limited availability or capacity to be present during IHA, communication between teams can be difficulty and a one-stop shop model places further workload on the community LAC team.
The findings presented show that UASC are often referred to a wide array of teams to assess and address different aspects of their complex health needs. However, we know from the literature that this can be troublesome, as many of these children are then lost to follow-up, or their social circumstance makes it challenging to attend all the different appointments. We suggest setting up a service that provides the IHA together with a comprehensive and holistic health assessment would be a model of care that may maximise the engagement of UASC with the health system.
Improving health outcomes of UASC requires health and child right advocacy. Healthcare professionals should regard all interactions with these vulnerable children as an opportunity to highlight their right to healthcare as well as ensure that their health needs are being addressed. Raising awareness on the barriers to healthcare faced by UASC together with political advocacy to improve the health services available are key to improve UASC health outcomes.
Conclusion
Our findings suggest significant variation in practice around UASC IHA across England, particularly regarding specific elements such as time allocated, translation facilities, ID testing, CAMHS involvement and training of staff. The findings highlight key differences that require further research to evaluate whether there is significant impact on UASC health outcomes. The results suggest there is a pressing need for further education and training on UASCH health for health professionals, which should include the voice of UASC themselves. Future research should focus on the health outcomes of UASC and explore the preparedness of health workers and health system to better meet the health needs.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This cross-sectional survey is exempt from formal ethics review under Health Research Authority guidance. Consent was obtained from participants prior to participating in the survey.
Acknowledgments
We would like to thank all the participants that took the time to complete the survey. We would also like to acknowledge the British Association for Community Child Health, CoramBAAF and Royal College of Paediatrics and Child Health who helped to distribute the survey.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @behrouzn
Contributors BNM, AJA and BW conceived and designed this study. BNM and AJA designed the survey. BNM, AJA and BW were responsible for survey distribution. BNM carried out data analysis and data interpretation. BNM wrote the first draft. This was critically revised for intellectual content by AJA and BW. All authors have approved the final version of the manuscript. BNM acts as guarantor.
Funding This research is support by the National Institute for Health Research grant ACF-2020-21-011 awarded to BNM. Imperial College London Open Access Fund supported the publication and dissemination of this work.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.