Article Text

Abstract
Objective To identify risk factors for severe disease in children hospitalised for SARS-CoV-2 infection.
Design Multicentre retrospective cohort study.
Setting 18 hospitals in Canada, Iran and Costa Rica from 1 February 2020 to 31 May 2021.
Patients Children<18 years of age hospitalised for symptomatic PCR-positive SARS-CoV-2 infection, including PCR-positive multisystem inflammatory syndrome in children (MIS-C).
Main outcome measure Severity on the WHO COVID-19 Clinical Progression Scale was used for ordinal logistic regression analyses.
Results We identified 403 hospitalisations. Median age was 3.78 years (IQR 0.53–10.77). At least one comorbidity was present in 46.4% (187/403) and multiple comorbidities in 18.6% (75/403). Eighty-one children (20.1%) met WHO criteria for PCR-positive MIS-C. Progression to WHO clinical scale score ≥6 occurred in 25.3% (102/403). In multivariable ordinal logistic regression analyses adjusted for age, chest imaging findings, laboratory-confirmed bacterial and/or viral coinfection, and MIS-C diagnosis, presence of a single (adjusted OR (aOR) 1.90, 95% CI 1.13 to 3.20) or multiple chronic comorbidities (aOR 2.12, 95% CI 1.19 to 3.79), obesity (aOR 3.42, 95% CI 1.76 to 6.66) and chromosomal disorders (aOR 4.47, 95% CI 1.25 to 16.01) were independent risk factors for severity. Age was not an independent risk factor, but different age-specific comorbidities were associated with more severe disease in age-stratified adjusted analyses: cardiac (aOR 2.90, 95% CI 1.11 to 7.56) and non-asthma pulmonary disorders (aOR 3.07, 95% CI 1.26 to 7.49) in children<12 years old and obesity (aOR 3.69, 1.45–9.40) in adolescents≥12 years old. Among infants<1 year old, neurological (aOR 10.72, 95% CI 1.01 to 113.35) and cardiac disorders (aOR 10.13, 95% CI 1.69 to 60.54) were independent predictors of severe disease.
Conclusion We identified risk factors for disease severity among children hospitalised for PCR-positive SARS-CoV-2 infection. Comorbidities predisposing children to more severe disease may vary by age. These findings can potentially guide vaccination programmes and treatment approaches in children.
- COVID-19
- Epidemiology
Data availability statement
Data are available upon reasonable request. The corresponding authors will consider data sharing requests that are accompanied by a study protocol and approval by an independent research ethics board.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Symptoms associated with SARS-CoV-2 infection are generally milder in children than in adults.
Severe courses can also occur in children and it is important to understand the risk factors for severity.
Several risk factors for severity have been identified, but the data are partly contradictory, especially with regard to age as risk factor among children.
WHAT THIS STUDY ADDS
Severe disease among children hospitalised for SARS-CoV-2 infection is associated with several risk factors including the presence of comorbidities, obesity and chromosomal disorders.
The risk profile and presence of comorbidities differ between paediatric age groups, but age itself is not associated with severe outcomes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Improved understanding of paediatric risk factors for severe SARS-CoV-2 infection can help guide management and refine risk-benefit analyses of paediatric vaccination programmes against SARS-CoV-2
Introduction
The clinical presentation of SARS-CoV-2 infection is generally milder in children than in adults. However, children can also experience morbidity and mortality due to COVID-19.1 Knowing the risk factors for severe disease allows for identification of patient groups that require closer monitoring or early treatment, and help guide targeted vaccination campaigns. While many countries started a vaccination programme against SARS-CoV-2 for all adolescents and children≥5 years of age, others had limited access to vaccines or decided to focus on high-risk groups following WHO recommendations.2 3
Previous studies have attempted to identify risk factors for severe disease in paediatric patients for severe SARS-CoV-2 infection.4–15 Some risk factors such as presence of comorbidities, obesity and increased inflammatory markers have been implicated,5 8 10–13 15 16 but many studies were small and there is substantial heterogeneity.17 Importantly, most major studies were from high-income countries, and data from low-income and middle-income countries are scarce.
The aim of this study was the identification of risk factors for severe disease in children hospitalised for symptomatic PCR-confirmed SARS-CoV-2 infection including PCR-positive multisystem inflammatory syndrome in children (MIS-C) in a multicentre retrospective cohort study from Canada, Costa Rica and Iran.
Methods
Study design and data collection
Sixteen paediatric hospitals from the Canadian Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) group and two international collaborators from Tehran, Iran and San José, Costa Rica identified all children<18 years of age admitted from 1 February 2020 through 31 May 2021 for PCR-positive SARS-CoV-2 infection or PCR-confirmed MIS-C. Patients who were admitted for reasons other than their SARS-CoV-2 infection (ie, incidental infections), as per each local investigator’s adjudication, were excluded. Data on primary indication for admission, demographics, comorbidities, clinical presentation and course, coinfections, treatments and complications were abstracted by the investigators from the patient’s medical charts and managed using REDCap electronic data capture tools.18 19
Variables of interest and study definitions
The primary outcome was severity of PCR-positive SARS-CoV-2 infection on the ordinal WHO Clinical Progression Scale (online supplemental table 1).20 Given the inclusion criterion of hospitalisation, all patients had a score of ≥4. As a secondary outcome, we used the WHO Clinical Progression Scale in a categorical fashion with a score of ≥6 for severe disease, that is, oxygen by non-invasive ventilation or high flow or mechanical ventilation or vasopressors or death.20 Baseline exposure variables (including the presence of chronic comorbidities: neurological, cardiac, pulmonary (also subcategorised into asthma; non-asthma pulmonary disease), metabolic, renal, and chromosomal disorders, immunosuppression (including malignancy), obesity, prematurity (<37 weeks gestational age), anaemia and/or haemoglobinopathy and ‘other’ comorbidities which included patients who could not be classified into the previous categories) and additional predictor variables are shown in tables 1 and 2 and described in detail in the online supplementary methods.21
Supplemental material
Baseline characteristics of patients with PCR-positive SARS-CoV-2 infection (N=403) according to country of origin
Clinical characteristics, investigations, treatments and outcomes of patients with PCR-positive SARS-CoV-2 infection (N=403) according to country of origin
Data analysis
Data were analysed using R V.3.5.2 (R Core Team, Vienna, Austria) and STATA V.17.0 (StataCorp, College Station, Texas, USA). Statistical significance was assessed by using two-tailed tests, with an α of 0.05. Baseline and demographic characteristics were summarised using frequencies, percentages, means and SD, medians, and IQRs. Categorical data were compared using χ2 or Fisher’s exact test as appropriate and continuous data compared using Wilcoxon rank-sum test. Statistical testing was limited to hypothesis-driven and biologically plausible comparisons; accordingly, correction for multiple hypothesis testing was not done. Ordinal logistic regression analyses were performed with the WHO Clinical Progression Scale as an integer to determine crude and adjusted ORs (aORs) and corresponding 95% CIs for factors associated with more severe disease. To investigate the association of specific individual comorbidities and disease severity, separate multivariable models were created for each individual comorbidity. Covariates considered potential confounders based on literature and clinical experience were included a priori: age, chest imaging findings, laboratory-confirmed bacterial and/or viral coinfection, and MIS-C diagnosis. We adjusted for age using cubic splines.22 23 To further explore the association of age with the outcome, age was categorised as <1 year, 1–4 years, 5–11 years and ≥12 years in separate analyses. Prespecified age-stratified analyses were also performed. Patients were excluded from the corresponding analyses in case of missing data points.
The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines were followed.24 There was no patient, parental or public involvement at any stage of this study.
Results
From 1 February 2020 through 31 May 2021, 982 children<18 years of age hospitalised for SARS-CoV-2-related illness and/or PCR-positive MIS-C were reported by the 18 study hospitals. We excluded 579 cases in whom SARS-CoV-2 was not confirmed by molecular testing from respiratory specimens or because the patient was admitted for non-SARS-CoV-2-related reasons. We included the remaining 403 hospitalisations (figure 1).

Flow chart of hospitalised children<18 years of age reported to the PICNIC study between 1 February 2020 and 31 May 2021 with a diagnosis of SARS-CoV-2 infection. MIS-C, multisystem inflammatory syndrome in children; PICNIC, Pediatric Investigators Collaborative Network on Infections in Canada.
Demographics and clinical characteristics
Hospitalisations occurred from 19 March 2020 through 31 May 2021; 266 cases (66.0%) were from Canada, 107 (26.5%) from Costa Rica and 30 (7.4%) from Iran (tables 1 and 2). Overall median age was 3.78 years (IQR 0.53–10.77). At least one chronic comorbidity was present in 46.4% and multiple comorbidities in 18.6% of children. Fever (82.1%), cough (51.6%), shortness of breath (46.6%) and vomiting (31.5%) were the most common presenting symptoms. Intensive care unit (ICU) admission was required in 115 patients (28.5%). Six patients died, all with comorbidities, including 2 patients with malignancies receiving palliative care.
Compared with the two middle-income countries, cases from Canada were older (median 5.82 (IQR 0.84–14.27) vs 2.15 (IQR 0.48–6.01) years) with a higher proportion of adolescents (32.8% vs 4.4%, p<0.001) and occurred later during the study period (66.5% vs 40.9% admitted in 2021, p<0.001). Other key demographic, clinical and outcome parameters were similar between countries.
Predictors of disease severity
Univariable ordinal logistic regression ORs for the primary outcome of severity along the WHO Clinical Progression Scale are presented in table 3. Presence of 1 and of >1 comorbidity was associated with disease severity. Individually, obesity, pulmonary, neurological and chromosomal disorders were significant risk factors. In contrast, immunosuppression and its subcategory malignancy were associated with decreased risk (table 3). Shortness of breath, cough and wheeze were the clinical presentations associated with severity. Among laboratory and imaging investigations, viral coinfection, chest imaging compatible with COVID-19, neutrophilia, increased C-reactive protein (CRP), increased ferritin and low albumin were statistically significant risk factors.
Characteristics of patients with PCR-positive SARS-CoV-2 infection (N=403) according to severity of disease (WHO COVID-19 Clinical Progression Scale of ≥6) and univariable ordinal logistic regression ORs for more severe disease along WHO COVID-19 Clinical Progression Scale
Multivariable ordinal logistic regression analyses adjusting for age, coinfection, chest imaging and MIS-C demonstrated that obesity (aOR 3.42, 95% CI 1.76 to 6.66) and chromosomal disorders (aOR 4.47, 95% CI 1.25 to 16.01) were independent predictors of severe disease (figure 2A). In a separate model adjusting for the same covariates, we examined the effect of the number of comorbidities instead of each comorbidity individually. The presence of a single comorbidity (aOR 1.90, 95% CI 1.13 to 3.20) and of multiple comorbidities (aOR 2.12, 95% CI 1.19 to 3.79) were significant risk factors.
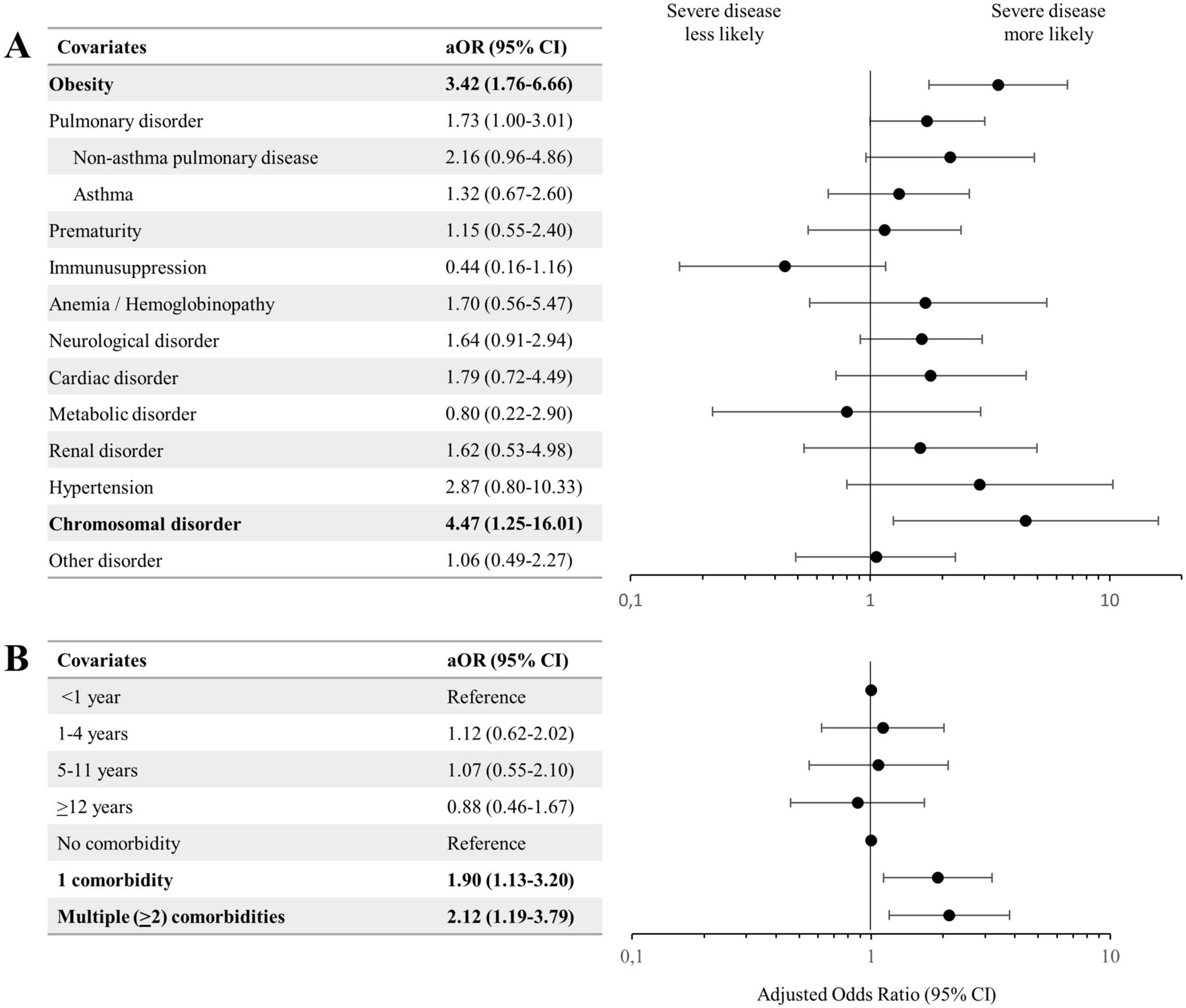
Multivariable ordinal logistic regression models for factors associated with more severe PCR-positive SARS-CoV-2 infection on WHO COVID-19 Clinical Progression Scale. (A) Model evaluating individual comorbidities. (B) Model evaluating age and the number of comorbidities as risk factors for disease severity. aOR, adjusted OR.
While adolescents≥12 years of age had a higher risk of severe disease in univariable analysis (table 3), age as a categorical variable (figure 2B) and age modelled as a cubic spline (figure 3B) did not demonstrate a statistically significant association with disease severity.

{kind=link}
{kind=link}
{kind=link}
Age as an exposure variable for factors associated with more severe PCR-positive SARS-CoV-2 infection on the WHO COVID-19 Clinical Progression Scale. Analyses according to ordinal logistic regression. (A) Unadjusted OR. (B) OR adjusted for the number of comorbidities, presence of any bacterial and/or viral coinfections, chest imaging results and multisystem inflammatory syndrome in children (MIS-C). Shaded areas represent the 95% CIs.
In adjusted age-stratified analyses, among children<12 years, the individual comorbidities associated with severity were pulmonary disorders (aOR 2.33, 95% CI 1.20 to 4.51), especially non-asthma pulmonary disorders (aOR 3.07, 95% CI 1.26 to 7.49) and cardiac disorders (aOR 2.90, 95% CI 1.11 to 7.56; table 4). Among adolescents≥12 years of age, the only comorbidity associated with severity was obesity (aOR 3.69, 95% CI 1.45 to 9.40). Of note, risk factors were not equally distributed between the two age groups. More adolescents had any (66.7% vs 40.2%, p<0.001) or multiple (25.8% vs 16.5%, p=0.049) comorbidities than younger children; obesity was markedly more common in adolescents (40.9% vs 3.9%, p<0.001). Among infants<1 year of age, neurological (aOR 10.72, 95% CI 1.01 to 113.35) and cardiac disorders (aOR 10.13, 95% CI 1.69 to 60.54) were independent predictors of severe disease.
Multivariable ordinal logistic regression models for factors associated with more severe PCR-positive SARS-CoV-2 infection on WHO COVID-19 Clinical Progression Scale, stratified according to age groups (children<1 year old; children<12 years old; children≥12 years old)
The secondary disease severity outcome (WHO COVID-19 Clinical Progression Scale ≥6) occurred in 102 (25.3%) of 403 children (table 3). In univariable analysis, patients with severe disease were older (median 6.69 (IQR 1.31–13.46) vs 3.21 (IQR 0.31–9.87) years, p=0.002). The proportion of children with severe disease increased progressively with age, with the lowest prevalence in neonates (8.1%) and the highest in ≥12 years old (35.5%). Compared with previously healthy patients, those with 1 or with ≥2 comorbidities were more likely to have severe disease (19.9%, 31.5% and 37.3%, respectively; p=0.009).
Discussion
In this multicentre cohort study from three countries, we identified risk factors for severe disease among children admitted to hospital for PCR-positive symptomatic SARS-CoV-2 infection. Previous studies have been either limited to administrative data,4 8 12 were smaller5–7 10 11 13 14 or had a different scope.25 We confirmed several previously described risk factors for severity including the presence of one or more comorbidities,4 6 9 12–16 obesity,5 8 11 14 15 neurological,8 14 15 pulmonary13–15 and chromosomal26 disorders.
Previous studies have described a bimodal age pattern regarding severe disease, with a first peak in the very young and a second increase in adolescence mimicking global non-SARS-CoV-2-related childhood mortality.4 5 7 12 Infants in our study population were over-represented compared with the general paediatric population. For Canadian children, the proportion of infants was 4.3 times higher than its share of the population,27 suggesting a higher probability of hospitalisation. It is likely that some young infants with mild symptoms were admitted for observation, especially early during the pandemic.28 We did not see a higher rate of severe courses according to age, in line with other studies which restricted their analysis to hospitalised children.10 14–16
Similar to other studies, we saw a higher proportion of severe disease in adolescents in our univariable analysis,4 10–12 but this was not confirmed in the multivariable models. This age group had a different risk profile than younger children. We found evidence that the comorbidities predisposing children to more severe disease may vary by age. While pulmonary (especially non-asthma disorders) and cardiac disorders were strongly associated with severe disease in children under 12 years old, neurological and cardiac disorders were risk factors in infants<1 year old, and only obesity predicted severe disease in adolescents. Two recent studies from the USA also observed that obesity was an independent risk factor for critical illness in adolescents but not younger children.15 29 This association more closely resembles adults, in whom metabolic risk factors are among the most important.30 The observed higher proportion of severe cases among adolescents in crude analyses could be mainly due to the markedly higher prevalence of obesity (40.9% in adolescents vs 3.9% in younger children in our study) and other comorbidities.
Our primary outcome using an ordinal scale differed from many previous studies which defined severity as ICU admission.5–8 16 31 ICU admissions are simple to measure, but can be problematic as a severity outcome because of heterogeneity across study sites due to dependence on local healthcare delivery structures and practice. In addition, patients with some comorbidities or within certain age categories may be admitted to ICU mainly for monitoring or for treatment of a condition independent of the severity of the current illness.32 In our dataset, 10 patients with high flow nasal cannula and/or non-invasive ventilation were managed outside of an ICU; in contrast, 26 patients in the ICU did not require mechanical or medical support of vital functions. Using ICU admission alone to define severity would have obscured the effect of several important risk factors. Therefore, we used the more objective WHO COVID-19 Clinical Progression Scale.20 Furthermore, to obviate the need for a cut-off, which can be arbitrary, we used ordinal logistic regression to measure associations with more severe disease.
We decided to include all hospitalised symptomatic patients with positive SARS-CoV-2 PCR, independent of the diagnosis of MIS-C. Although the pathophysiology is different,33 it is frequently impossible to distinguish severe acute SARS-CoV-2 infections from PCR-positive MIS-C and both can be present at the same time.25 Thus, the strict separation of acute COVID-19 and early PCR-positive MIS-C may be an oversimplification. Moreover, treatment regimens for both conditions can overlap. Late, and typically PCR-negative, MIS-C has been shown to have different severity risk factors.5 13 25 34 By requiring patients to be PCR-positive, two-thirds of patients with MIS-C were excluded.
Our study has limitations. First, reporting may not have been uniform across centres despite the use of a study protocol and a standardised data capture tool. This includes but is not limited to the interpretation of chest radiographs, the definition of obesity and the severity of comorbidities. Second, despite being one of the largest paediatric cohort studies with more than 100 severe cases, the numbers of some individual comorbidities are small. This might overestimate or underestimate the impact of infrequent comorbidities such as anaemia and/or haemoglobinopathy, chromosomal or cardiac disorders. Third, laboratory investigations were not systematically performed. Complete blood counts, CRP and albumin values were missing in 4.2%, 14.9% and 67.2%, respectively. Moreover, laboratory investigations were done at the clinicians’ discretion, not at set time points during the illness. Other parameters previously described as risk factors could not be evaluated including ethnicity,4 7 9 12 which was not readily accessible from hospital records. In addition, viral sequencing data were not available. Fourth, indications for testing for SARS-CoV-2 likely varied by centre and over time, which might have affected the clinical spectrum of included patients. Fifth, our study was not population-based. Most participating hospitals are referral centres so milder hospitalised cases might have been missed and this might overestimate the rate of severe courses. In addition, there were only two hospitals from Costa Rica and Iran, representing one-third of the total sample size; they may not be representative of middle-income countries in general. Accordingly, we did not systematically compare risk factors between Canada and the middle-income countries.
A strength of our study includes its multicentre, multinational design covering the first 15 months of the COVID-19 pandemic. The patient population of symptomatic children hospitalised for PCR-confirmed SARS-CoV-2 is well defined and reduces potential biases from including incidental detections of SARS-CoV-2. Finally, this study represents a large yet comprehensive dataset with over 100 severe cases with a WHO severity score ≥6, thereby allowing us to identify differences in risk factor profiles across age subgroups.
In conclusion, we identified several independent risk factors for severe disease in children hospitalised for symptomatic PCR-positive SARS-CoV-2 infection. Based on our analyses, age was not an independent risk factor, but there appears to be a notable age dependence of specific comorbidities that predispose to severe disease, with obesity in adolescence and cardiac, pulmonary and neurological disorders in younger children as the most important underlying comorbidities. Improved understanding of paediatric risk factors for severe SARS-CoV-2 infection among children requiring hospitalisation can help guide management and refine risk-benefit analyses of paediatric vaccination programmes against SARS-CoV-2.
Data availability statement
Data are available upon reasonable request. The corresponding authors will consider data sharing requests that are accompanied by a study protocol and approval by an independent research ethics board.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from each participating institution’s ethics research board, with waiver for informed consent for health records research (online supplementary methods).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @TilmannSchober, @drtammiedewan, @TalPedsRheum, @peterjgill, @DrFatimaKakkar, @leifsok, @LucPanetta, @manishs_, @drkarinatop, @rolandoug, @JWong_PedsID
Contributors The study was conceived by JLR, MB and JP, and supervised by JLR and JP. Analysis was conducted by CC, JM and TS. TS wrote the first draft of the manuscript. All authors contributed to data collection and interpretation, reviewed the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work. JP is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.