Article Text

Abstract
Background Children have been relatively spared from the direct effects of COVID-19 globally, but there are significant concerns about indirect effects on the most vulnerable children’s well-being. Nigeria is the largest African nation, but little is known about children’s experience of the COVID-19 pandemic. Our aims were to determine children’s knowledge of COVID-19 and their mental health responses to the pandemic.
Methods Children aged 6–17 years living in Calabar, Nigeria, were surveyed using a combination of online data collection assisted by parents and on-site data collection at schools. Parents filled out sociodemographic details, while children answered questions about COVID-19 knowledge and preventive measures. An adapted version of the ‘Perceived Stress Scale for Children’ was used to assess stress with additional free text space for expression of views and experiences of COVID-19.
Results A total of 265 children completed questionnaires, mean age was 12.5 years, 52.1% were girls. All children knew about the virus and over two-thirds (67.8%) had good knowledge of COVID-19 transmission. Children identified television (60.8%), parents (44.2%) and social media (32.8%), as main sources of COVID-19 information. The overall mean stress score among the children was 20.47. Children mentioned the following as stressors: fear of the COVID-19 disease, effect of pandemic restrictions on schooling and social interactions as well as home/family tensions. Parental love and support were overwhelmingly reported as strengths.
Conclusions Nigerian children in this study had good knowledge and understanding of the COVID-19 pandemic and preventive measures to counter the virus. Children had high stress levels and expressed pandemic-related concerns but parental love and support were mitigating factors. Government and child health service providers need to tailor health and support services in response to children’s needs and concerns.
- COVID-19
- Child Psychiatry
- Adolescent Health
- Psychology
- Qualitative research
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
The effects of the COVID-19 pandemic and infection control measures have been wide reaching.
The pandemic disproportionately affects the health and well-being of children and young people in low-income settings and the most marginalised.
Studies from other low-resource settings have highlighted children suffering most from the effects of financial strain and lack of education.
What this study adds ?
Nigerian children in the study had adequate knowledge of COVID-19 and associated preventive measures.
The effect of the pandemic and its control measures on children’s mental well-being using psychological stress scales showed high stress scores.
The positive effect of parental support and increased parental contact caused by lockdown due to the pandemic featured strongly in children’s reported coping mechanisms.
How this study might affect research and public policy ?
Greater attention should be paid by researchers to the needs of children and enabling their experiences and voices to be heard.
Governmental response to the pandemic and recovery efforts should consider the rights of the child with specific efforts targeted at recovery of the educational system from the pandemic and psychological support for children.
Introduction
The public health crisis born from the emergence and spread of the SARS-CoV-2, or COVID-19, has dramatically changed the global public health landscape.1 The pandemic brought drastic changes to people’s livelihoods, with economic, social and infrastructural disruptions across the globe. Children and young people (CYP) have been relatively spared from significant morbidity and mortality, but have faced indirect effects of the pandemic and related health measures.2 At the height of the pandemic, a record 1.6 billion children were out of school. The pandemic, including the impacts of public health containment measures, impinges on CYP’s access to rights and safety.2
Nigeria’s first case of COVID-19 was diagnosed in February 2020. Consequently, the Nigerian government instituted a series of virus containment measures.3 Federal policies were developed in line with WHO strategies for virus containment: the institution of restrictions on international travel, closure of schools, universities, churches, mosques and bans on large social gatherings.3 4 There have been attempts to document how the pandemic has impacted mental health and lived experiences of adults globally, including specific studies in Nigeria.5 6 These studies conducted in Nigeria have largely excluded children’s experiences. Other reports noted increased gender-based violence targeting women and children, and predicted that Nigerian children would suffer from pandemic control measures.7 8 In sub-Saharan Africa, there were significant concerns about the mental health impacts of COVID-19 restrictions, particularly school closures and stay at-home policies which heighten family and parent–child stressors.9 As seen in other countries, Nigerian children may have also suffered consequences of school closure including loss of play, supplementary meals, physical and social networking, and isolation.10 11
This study was conducted in Calabar, the capital of Cross River State in Southern Nigeria, which has an estimated population of 371 022.12 In compliance with federal directives, state lockdown came into effect in the latter part of 2020, with cessation of interstate travel.13 In addition to pandemic restrictions, civil unrest led to the implementation of a statewide curfew, which was lifted in mid-2021.14 These protests over COVID-19 food subsidy items and police violence involved looting of businesses, governmental establishments and private homes resulting in tighter movement and security measures by the government. This increased social, economic and institutional strain, threatening livelihoods and well-being of families and children.15 16 Our aims were to assess children’s knowledge of COVID-19 and experience of stress during the pandemic, using a structured tool. A simple stress screening tool was used to capture experiences, with the addition of free-text responses to allow children’s voices to be heard.
Methods
We undertook a mixed-methods cross-sectional study from August 2020 to March 2021. Children aged 6–17 living in Calabar from March 2020 were recruited. The sample size was determined using minimum sample size for descriptive studies.17
This study included online data collection from CYP who participated during school closures, and data collection carried out at schools after reopening. Purposive and snowball sampling were used to recruit online participants. Researchers disseminated the online questionnaire link to parents through social, religious and school groups within the study area. Parents also forwarded the link to other parents within the locality. Online data collection halted when no new entries were received. A stratified sampling method was used to recruit respondents in schools that met COVID-19 reopening guidelines within Calabar. A list of these schools was obtained from the State Ministry of Education and grouped into public and private ownership. A sampling ratio was created using the sample size required and the total population in the schools approved for reopening. This ratio was used to obtain the number of children to be polled from each group of privately owned versus public/government owned schools. A simple ratio of the number of private to public schools was used to determine the number of schools to be visited. A random number generator was used to identify specific schools per category.
An equal sample size was thereafter taken from each school. Each sample was evenly distributed across all grades and then streams of classes. In each class, the register was used to pick every second name on the class list until the allocated sample for the class was exhausted. Children who wished to participate took forms home to their parents who provided signed consent and answered brief demographic questions. These questions covered social class information, type of schooling during the pandemic, tribe and religion (online supplemental file). Social class was grouped according to Oyedeji social classification which allocates a score to each parent based on their occupation and level of education. The score is tallied together to provide a grouping for the family from level 1–5 which is further reclassified into upper, middle and lower social classes.18 For online data collection, parents completed consent and forwarded the questionnaire links to their children to complete. Younger children or those without personal devices were aided by parents, who were instructed to record only the child’s responses. For onsite data collection, children completed questionnaires in school with investigators present after returning parental consent forms. The instrument was disseminated in English, which is the common language of communication in the region.
Supplemental material
Patient and public involvement
The researchers liaised with parents and children during the prepilot study to identify outcome measures which children felt most concerned about. This was instrumental to the identification of a study tool that considered schooling and social activity via play.
Informal discussions were held with children during clinic visits about their opinions on the pandemic and control measures. Parents were involved in the voluntary recruitment of other parents within the study area by forwarding online links to other parents only. Key identified parents who were leaders of parent–teacher associations in the selected schools also perused the questionnaires before the study commenced. Results of the study were sent to participants parents via email, text or phone calls. A correspondence sheet was used for the school-based arm of the study while online respondents were contacted via phone call and email; indicating children’s stress score category and psychologist referral for children with high stress scores. Information materials were given to all the children who participated.
Tools
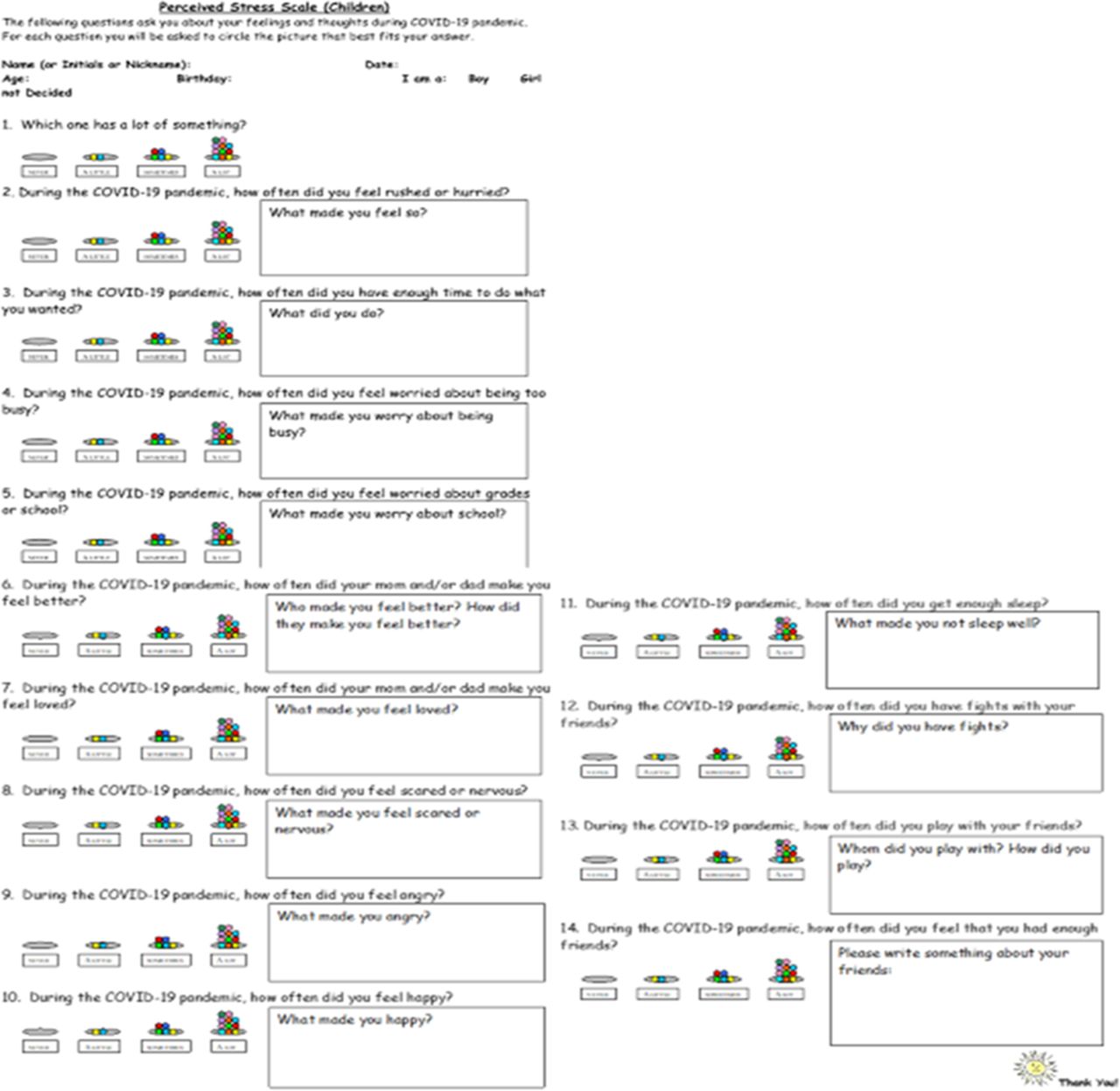
White et al’s Perceived Stress Scale-Children (PSS-C), a validated redesign of the original Perceived Stress Scale for children aged 6–17, was used to assess participants’ stress.19 The PSS-C is an easy to use tool for children: concise, efficient and well-suited to online application. The PSS-C was modified with White’s permission (see figure 1), changing the time designation in each question to ‘during the COVID-19 Pandemic’ instead of ‘in the last week’. Additionally, open-ended ‘free text’ versions of each question were added to collect qualitative data on children’s experiences. The PSS-C comprises 14 questions targeting key areas of childhood stress perception, including experiences of time pressure, concerns about grades, parental relationships, feelings of fear, anger and happiness, sleep and friendship. Possible scores range from 0 to 39. Responses were scored from 0 to 3, with ‘never’ 0 points and ‘A lot’ 3 points. Questions 3, 6, 7, 10, 11, 13 and 14 were reverse scored, as in the original PSS-C. Higher total scores indicated higher stress perception.19

{kind=link}
Questionnaire.
In addition to stress measures, data were collected on COVID-19 knowledge and preventative measures for COVID-19. We created a simple questionnaire using yes/no questions to assess children’s knowledge of COVID-19 transmission and their practice of preventative measures, scored as 1 mark per question (range 0–4) (table 1). These questions were based on mode of transmission of the virus and the preventative measures adopted. Questions formulated were based on COVD-19 information disseminated by the government and private sector on television (TV), social media and other public fora including schools, churches and malls. The information was fact checked for validity based on scientific publications prior to inclusion in the questionnaire20 Data on COVID-19 information sources were additionally collected through multiple choice responses.
COVID-19 knowledge and preventative measures
Analysis
Qualitative
Free-text descriptions were analysed using thematic analysis.21 We triangulated the results from qualitative and quantitative data to get a full understanding of children’s experiences of COVID-19.
Results
Quantitative
The total number of valid entries in the study were provided by 265 children. Table 2 lists the sociodemographic details of participants. Participants’ age range was 6–17 years with an average age of 12.5 years. Majority of children were from the middle social class, one-fifth of children had no form of schooling.
Sociodemographic characteristics of study participants N=265
Knowledge and information sources regarding COVID-19
All respondents had knowledge of the existence of COVID-19. Children identified TV (n=161, 60.8%) as the primary means by which they obtained information. This was followed by parents (n=117, 44.2%), social media (n=87, 32.8%) and lastly radio (n=70, 26.4%), with some children having multiple sources of information.
Knowledge of COVID-19 and preventative practices
Knowledge and preventative practice scores are provided in table 3. Knowledge was varied, but relatively high; 96 children (36.2%) obtained the highest possible score. Almost half (n=127, 48%) of children who responded had the highest possible score regarding preventative measures.
Score of knowledge of COVID-19 and preventive measures N=265
Stress scores
The overall mean stress score among participants was 20.47 (SD=5.109). The range of scores was 3–33. The mean stress score for females was 20.59 (SD=5.08) and for males was 20.34 (SD=5.224).
Qualitative results
Children’s free-text responses revealed several pandemic-related and exacerbated stressors, while highlighting key protective factors. The most salient and prevalent responses to questions about stressors and protective factors are detailed.
Stressors
Disruptions to schooling
‘I could not learn’ 10 year old, Male
School was a pervasive factor in children’s responses about stressors during the pandemic. Uncertainty related to school disruption was notable, despite most children engaging in online school methods. Many children described ‘missing school’ and wanting to ‘go back’. Children bemoaned ‘lost schooling time’, ‘regressing academically’ and ‘declining’ performance, they feared repeating classes and felt frustrated they ‘could not learn’. Children worried about ‘coping when school resumes’ with the volume of schoolwork. One child was angry that they ‘still had exams after corona (sic)’. Despite frustration with lost physical schooling, there were responses about too much online schoolwork during lockdown.
COVID-19 virus and contextual fears
‘The virus might take the world including my family’ 9 year old, Male.
Another stressor for children was pandemic-related fear. This was in relation to mortality—being ‘nervous about deaths’, hearing that ‘Corona kills people’ and scared ‘people were dying’. A few children were specifically scared about contracting COVID-19 or losing families and loved ones. Concern about the virus and awareness of its high transmissiblity was notable with a 7-year-old child reporting being scared of ‘what will happen when I go out’.
Responses were in highly emotive language and included how ‘people went down the drain’ and ‘the world may come to an end’. Some responses also alluded to rioting causing ‘so much disruption’. There were prevalent feelings of not ‘knowing what will happen next’. One child noted, ‘things changed drastically and not in my favour’.
Pandemic restrictions
‘I felt I had lost all my friends’ 16 year old, Female
This encompasses the stay-at-home mandates for which many children report feeling bored and trapped, distress and anger at being ‘deprived of going outdoors’ or not let out of their homes. It also includes general frustration at preventative measures with reports of being angry at the lockdown and feeling rushed always due to wearing facemasks. Loss of social opportunities, loneliness and missing friends was of particular concern with children upset they could not see friends, go to church and play with others. One child stated they ‘had lost all my friends’ over lockdown.
Home and domestic stress
A few children mentioned stress related to their parents and home life. For some, the pandemic brought increased domestic labour, with ‘too many house chores’. Others mentioned punishments from parents ranging from increased ‘scolding and beating at home’ to having possessions ‘collected’ by parents. There were also reports of fighting ‘with my siblings a lot’ during lockdown.
Protective factors
Parents
‘They always take care of me.’ 6 year old, Male
Children’s responses to happiness and feeling loved prominently featured being taken care of and having needs met by parents. Many responses were non-specific descriptions of care: ‘treating me with care’, ‘took care of me’. Some identified security as an expression of love, being ‘protected’ from outsiders and made to ‘feel safe’. This notion of security included needs, with children emphasising being ‘provided’ for. Others said parents bought things for them, particularly to facilitate schoolwork and to, ‘keep us busy and happy’. Parents purchased electronic devices and internet data to allow for remote learning. Additionally, children were bought special gifts, games, books and recreational goods. Multiple responses described new subscriptions to TV channels/streaming services. A number of responses about parents involved expressions of physical and verbal affection through being hugged and held. One child explained how parents ‘carried me to the village’. Parents also provided emotional support and encouragement, ‘ensuring us that we will be ok’.
Quality time with family
‘Having the opportunity to discuss with my parents which I never did before now’ 12 year old, Female
Children’s descriptions of support included increased time spent with family. Numerous responses to how parents made children feel loved asserted that parents ‘spent time’ with children. Many children noted that parents deliberately stayed home for this purpose and actively engaged with children, ‘doing things we want to do’. Such ‘things’ included ‘playing’, ‘reading interesting books’, praying together, telling stories and ‘playing musical instruments’. Children also spent increased time conversing with parents. One child appreciated ‘having opportunity to discuss with my parents which I never did before’.
Food
‘They wore me a face mask and took me to Domino’s pizza because I was crying to go there’ 7 year old, Female
Food security played a central role in descriptions of having ‘needs’ met. Being fed, given special treats were mentioned more than forms of physical affection. Many children indicated that simply providing food was a way parents made them feel loved. Examples included ‘plenty’ of food provided, and ‘enough’, food at home. A number of children also noted special practices around food during the pandemic—parents made children feel loved by cooking ‘delicacies’, ‘special dishes’, buying ‘treats’ and making snacks.
Benefits of lockdown
‘I could play without thinking of school’ 8 year old, Female.
While lockdown was a source of much frustration and anxiety, some children were happy about not attending school with no homework and more time for recreation. One child described freedom to ‘play without thinking of school’, and being able to do enjoyable things without worrying about schoolwork. A number of children mentioned they were happy because they had more leisure time—to play games, watch cartoons on TVand sleep more.
Discussion
This study was carried out at the peak of the COVID-19 pandemic in Nigeria. The mean stress score in this study using the PSS-C was 20.47. This is higher than the mean scores of American children with (15.44) and without pre-existing psychological conditions (11.24) found in White’s original PSS-C study.19 We acknowledge that it is not plausible to draw comparisons between Whites’s population and our study. It has however been documented that global estimates of depression and anxiety in CYP have doubled from prepandemic levels.22 There is a paucity of comparable objective assessments on pandemic related effects of the mental health of children in the West African subregion. The stress score from this study mirrors reports of stress and loneliness in Nigerian university students as well as depression and anxiety levels in the adult populace.5 8 There is also the possibility of pre-existing health and social inequities in Nigeria aggravating mental health outcomes with lack of social security to cushion income losses. In addition, a paucity of palliative measures to ameliorate mass suffering from hunger and social restrictions manifested in protests, rioting and looting.15 23 Free-text responses from children reflected societal instability with ‘fear of riots’. In addition, a range of stressors were identified by the children including the lack of schooling and fear of the COVID-19 virus. The effects of pandemic restrictions with loss of social life, home/family tensions were cited as contributors to stress in this study. This is in keeping with reports regarding CYP during the pandemic; particularly females in the home and community who were found to be at higher risk of stress, gender based violence and abuse as well as increased depression and anxiety.10 22 24 25 Furthermore, younger children requiring more parents physical presence and exhibiting ‘clinginess’ could increase stress at home and responsibility of child care on older siblings.22 24 26 The additional burden on parents of home-schooling children or supervising online learning with generating income may also heighten home tensions with negative consequences on children.
Schooling concerns featured prominently in the reports by children in this study. Interestingly, despite majority of respondents being middle class, one-fifth of surveyed children did not have any form of schooling at the time of the study. The pandemic has increased poverty in Nigeria, Africa’s most populous nation with long-standing educational and social inequity.7 27 As a consequence, an already-low demand for, and access to, quality education may have weakened.16 A worsened effect of this situation on children of lower class families due to prepandemic socioeconomic and educational inequalities is expected.23 In other studies, school disruptions during the pandemic were reported to increase stress and anxiety in children partly due to loss of social and peer group support.24 The experiences from Nigeria were similar to concerns in various other countries over education during the pandemic.10 26 28 Concerns were expressed by respondents over school workload with online classes, on resumption and particularly halting of their education.
All children assessed were aware of the existence of COVID-19. This mirrors findings from India and Kenya, where all respondents had knowledge of the virus.10 11 Direct text responses from children in this study further confirmed their understanding of the COVID-19 virus and its effect on their lives and the world at large. Knowledge of transmission and preventive measures among children was good, with majority having complete awareness of transmission and practice of preventive measures. Children in this study reported unease with physical preventative measures such as wearing a face mask and handwashing. They however acknowledged the role of these practices in reducing their risk of infection.
Children’s coping mechanisms were predominantly parental support, love and provision. Worldwide trends regarding the pandemic have highlighted food security as a concern.29 This agrees with children in this study documenting the knowledge of food safety in allaying fears of uncertainty. In addition, parental bonding featuring discussions supported children during the period. Interestingly, despite the positive impact of family, physical violence was reported by respondents as constituent of identified home based stressors. Other studies have highlighted the dual role of families during the pandemic both as providing strength and support, while being a source of stress.30 31
Strengths and limitations of the study
This study employed the use of mixed methods in assessing the experiences of Nigerian children during the COVID-19 pandemic. The use of an objective stress scale allowed for an unbiased view of the children’s mental health. Qualitative analysis provided a hitherto unexplored access to children’s feelings. The authors, however, note that a larger number of respondents came from the middle socioeconomic class; and therefore, this study cannot reflect the totality of all Nigerian children’s experiences. In addition, this may have affected observations with members of the middle class largely able to provide coping mechanisms for their children and buffer effects of the pandemic by working from home, providing food and other amenities. Additionally, not all the respondents filled in the free text questions for qualitative analysis. Prepandemic levels of stress were also not available for the study area to provide further comparison of the findings in this study.
Conclusion
This study reports on Nigerian children’s experiences during the COVID-19 pandemic. Children had good knowledge about COVID-19 as well as public health measures in keeping with other studies from low-resource settings.10 32Stress levels were high with children worried about schooling, access to food, COVID-19 virus and the effect of control measures. Family-related stressors and the value of parental love and support featured prominently as stressors and coping mechanisms respectively. The public health and policy response to the pandemic and recovery in Nigeria should consider children’s voices and concerns. These responses should be based on equity and child-rights for the greater good of all Nigerian children particularly the marginalised, out-of-school, children in poverty and younger children.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Cross River State Ministry of Health Research Ethics Board (No.: CRSMOH/RP/REC/2020/129).
Acknowledgments
Great thanks go to Barbara P. White, University of New Hampshire for accepting the rearrangement of the original questionnaire for the COVID-19 pandemic. Additional acknowledgements go to the International Society for Paediatrics whose team members were vital to the development of this research work as part of the ‘voices of the children’ in COVID-19. Further thanks go to head teachers and the parents teachers association leaders who gave advise on the conduct of the study. We appreciate the contribution of Dr. Leo Muoneke who assisted in data collection in schools.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @@Hajime Takeuchi6
Contributors OAA: conceptualised, funded, proposal note for ethical, collected data, entered, cleaned, analysed data, wrote major parts of manuscript.Responsible for the overall data. SR: data cleaning and analysis, editing. SN-R: data cleaning and analysis, writing and editing. HT: methodological support, data cleaning. EAA: assisted in writing ethical, collected data, entered data. EN: collected data, entered data. All authors previewed and contributed to manuscript writing. OAA acts as gurantor for this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.