Article Text

Statistics from Altmetric.com
Introduction
Hyperthyroidism, or excess thyroid hormone production, causing signs and symptoms of thyrotoxicosis, is a rare but serious disorder in children and young people. Biochemically, the hallmarks of hyperthyroidism are an excess of circulating free thyroxine (fT4) and triiodothyronine (fT3) secreted from the thyroid gland and a suppression of thyroid-stimulating hormone (TSH). The most common cause is Graves’ disease, resulting from TSH receptor stimulation by autoantibodies.1 Thyrotoxicosis can occur at any age, but frequency increases with age and peaks during adolescence, with an incidence of Graves’ disease reported as 1 per 100 000 in children under the age of 16 years.2 3 Less commonly, thyrotoxicosis could be due to subacute thyroiditis, early Hashimoto’s thyroiditis, chronic lymphocytic thyroiditis, autonomous functioning nodules, amiodarone induced thyrotoxicosis and activating TSH receptor mutations. More recently, COVID-19 infections have been proposed as triggers with association studies demonstrating an increased frequency of thyrotoxicosis, likely to be a consequence of cytokine fluxes,4 as reported in adult populations.5
Although relatively rare in children, it is important for paediatricians to recognise features early to minimise the risks arising from thyrotoxicosis.6 In mild cases, attention span and school performance can be affected due to the cognitive and psychosocial impact of excess thyroid hormones.3 7 While accelerated growth8 does not usually lead to early puberty and reduced final height,9 the long-term risk of osteopaenia through suboptimal bone mineralisation remains pertinent.10 Children often present with irritability, weight loss, excessive sweating and heat intolerance; these features should prompt investigation for thyroid status without delay.3 It is critical to act early to prevent deterioration into more severe forms of thyrotoxicosis, such as a thyroid storm. This is a medical emergency with potential for life-threatening cardiovascular instability and a high mortality rate, estimated at 10%.6 In contrast to unhindered thyrotoxicosis, overtreatment, resulting in hypothyroidism, risks deceleration in growth and impaired quality of life.11 Thus, treatment of thyrotoxicosis in childhood is finely balanced and requires a deep understanding of the diagnostic principles and complex short-term and long-term risks.
At present, consensus treatment guidelines for childhood thyrotoxicosis are emerging and intended mainly for specialist review.3 12 Given the common practice of managing children with hyperthyroidism in a non-specialist setting, we have adopted a general paediatric perspective to discuss the diagnostic and therapeutic management of thyrotoxicosis in children and young people (excluding neonates) in shared care with specialist paediatric endocrine services. Our aim has been to review and assimilate information from an up-to-date evidence base with practice insights from specialists in endocrinology and biochemistry to provide recommendations for general paediatricians.
Clinical assessment
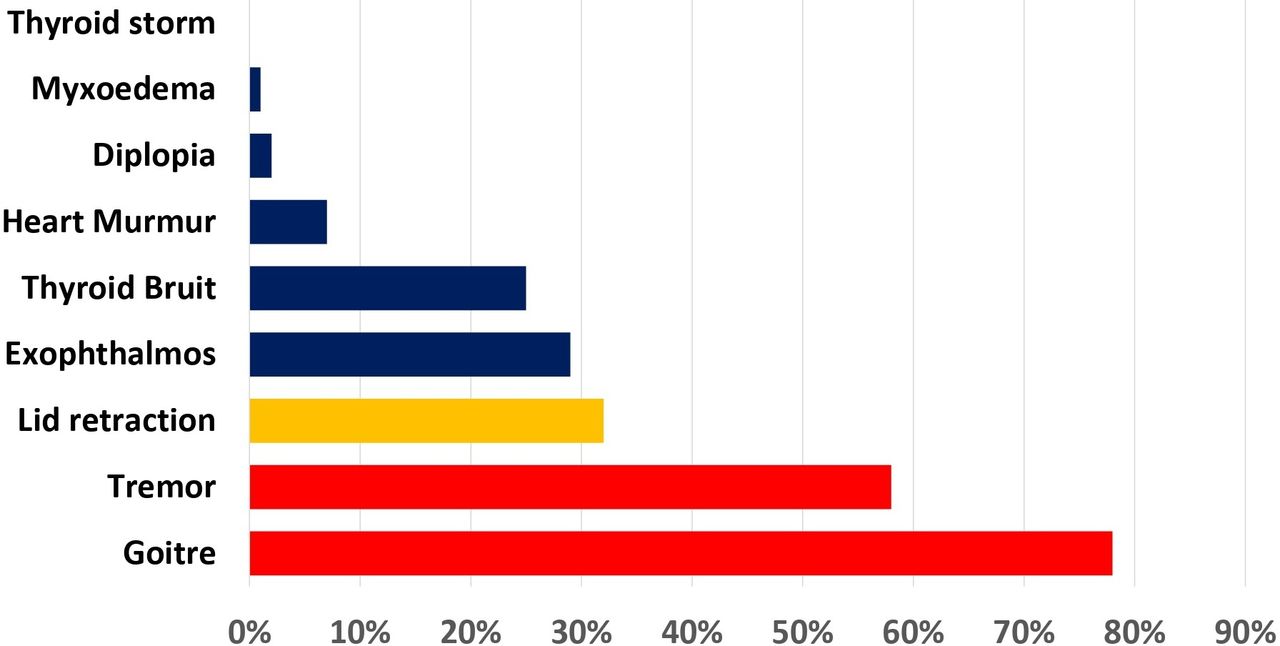
The diagnosis of thyrotoxicosis is relatively simple in children presenting with the typical features of tremor and goitre on a background of tiredness and weight loss.13 However, a wide variety of symptoms and signs may be present at diagnosis (figures 1 and 2) thereby making clinical diagnosis challenging, especially in mild cases. In thyrotoxicosis, deteriorating academic performance and anxiety could be incorrectly attributed to psychosocial stressors, while mild degrees of lid retraction or a small goitre might be overlooked. Nonetheless, the presence of more than one symptom/sign should prompt investigation to explore the possibility of thyrotoxicosis. In most cases, a thorough history and examination should be sufficient to identify even the mildest cases. Reluctance to walk upstairs in children previously capable, suggesting proximal muscle weakness, could be missed as a sign of thyrotoxicosis in preschool children. At this age, clinical features such as heat intolerance and inadequate weight gain may be less frequent, being overshadowed by behavioural changes, sleep disturbances and feeding problems. Asymptomatic presentations have been reported13 but subtle features may have been overlooked in such cases.
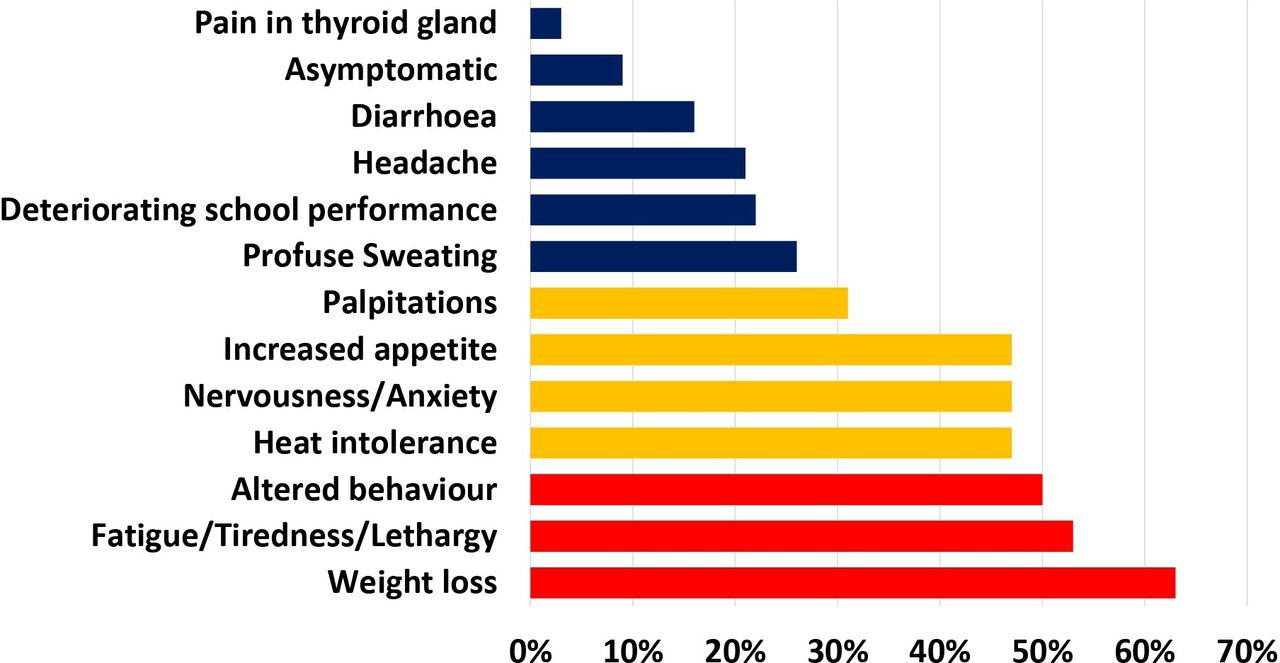
Presenting symptoms of thyrotoxicosis represented as percentages of all manifestations at diagnosis in a national survey of children and young people below age 15 years. Modified data have been derived from a 1-year British Paediatric Surveillance Unit study.13 Symptom frequency >50% is represented by red bars, 30%–50% by amber bars and <30% by blue bars.
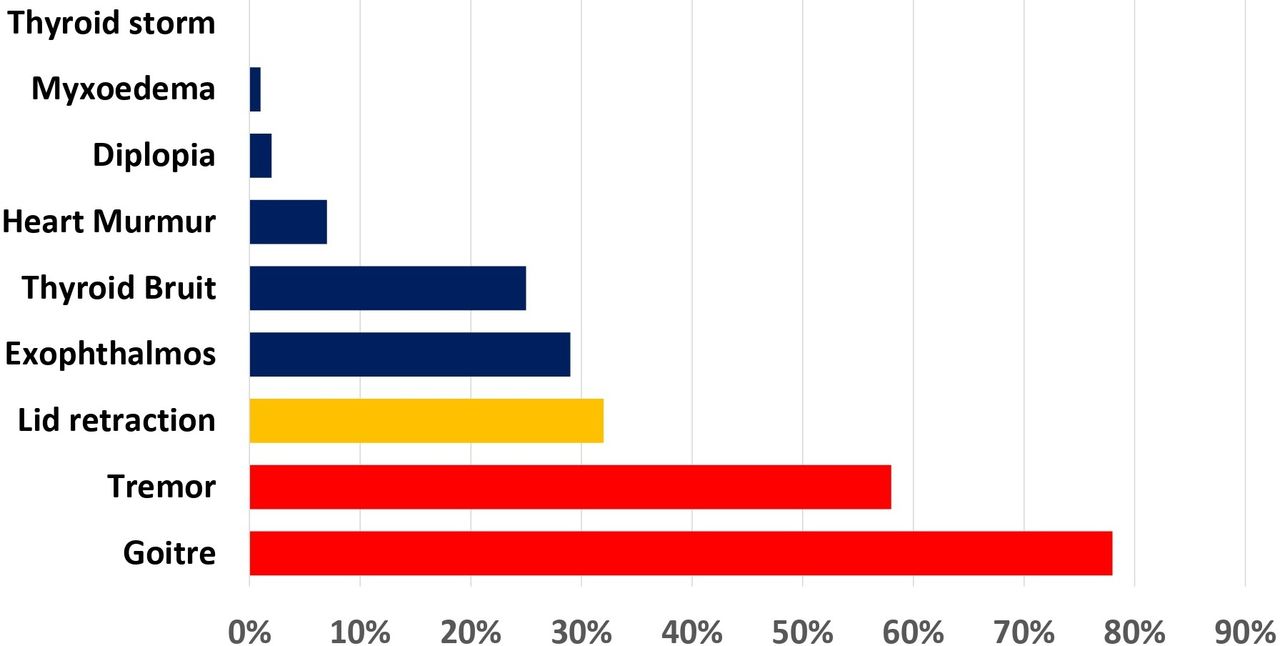
Presenting signs of thyrotoxicosis represented as percentages of all manifestations at diagnosis in a national survey of children and young people below age 15 years. Modified data have been derived from a 1-year British Paediatric Surveillance Unit study.13 Symptom frequency >50% is represented by red bars, 30%–50% by amber bars and <30% by blue bars.
Acute presentations
In children with significant hyperthyroidism, signs of thyrotoxicosis reflect a rapid metabolic and cardiovascular state. An extreme form, although rare, is thyroid storm. Diagnosis is clinical (table 1), and no specific laboratory tests are available. Precipitating factors include incompletely treated thyrotoxicosis, major trauma, stress, infection and medications.14 Scoring systems to indicate the likelihood of thyroid storm are available for adults15 and, although not validated in children, have reasonable rationale for use in young people. In all cases, suspicious features should prompt an urgent referral to paediatric endocrine services.
Features of thyroid storm due to a major surge in thyroid hormone production
Eye signs
A third of children with Graves’ disease have significant eye disease13 due to antibody-mediated infiltrates in retro-orbital fat and muscles.16 Eye signs range from minimal lid lag to proptosis. Early ophthalmology referral is essential to consider treatment to reduce inflammation. In adults, Graves’ orbitopathy is resistant to treatment with steroids in 20%–60%, prompting the need for alternative therapies.17 Fortunately, in children, Graves’ orbitopathy is rarely as problematic and simple measures to lubricate and protect the cornea are sufficient. In the rare cases where orbitopathy is prominent, a referral to a specialised ophthalmology service would be suggested18
Recommendation: All children with eye signs should be promptly referred to specialist paediatric ophthalmology services.
Associated autoimmune disorders
Many children with Graves’ disease have an increased risk of other autoimmune conditions such as diabetes mellitus, coeliac disease, primary adrenal insufficiency, vitiligo, systemic lupus erythematosus, rheumatoid arthritis and pernicious anaemia.19 Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy is a subtype of Graves’ disease with higher mortality.20 Polyglandular autoimmune endocrinopathy,21 where Graves’ disease is associated with Addison’s disease and diabetes, must be recognised, as treatment implications are wider. The risk of associated autoimmune disorders should also be considered in conditions where the background risk is higher, for example, in trisomy 21 and Turner’s syndrome.19
Investigations
Thyroid function tests
In overt hyperthyroidism both fT4 and fT3, concentrations are elevated and TSH is suppressed. In milder hyperthyroidism or T3 predominant Graves’ disease, fT4 levels can be normal, with an undetectable TSH; here only fT3 is elevated.6 When interpreting results, age-related local laboratory ranges should be considered. The diagnosis of Graves’ disease is supported by the finding of positive TSH receptor antibodies (TRAbs) and thyroid peroxidase (TPO) antibodies.
It is important to recognise resistance to thyroid hormone (RTH) where thyroid hormones are high but TSH remains normal. If RTH is suspected, specialist review would be recommended to confirm the diagnosis and to investigate for genetic mutations in the thyroid hormone receptor.22 In RTH, antithyroid treatment is counterproductive, unless peripheral toxic effects justify its use.23 There is no place for thyroidectomy in these children.
Thyroid hormone levels are commonly measured by immunoassays and can be influenced by interference from chemicals and metabolites (box 1). If there is discordance between clinical features and biochemical analysis, the results are best discussed with the laboratory. Methods to investigate possible interference include comparison with an alternative platform, dilution, polyethylene glyco precipitation and blocking agents.24 Antiruthenium interference has been described using the Roche assay as the platform uses Ruthenium as a label in its immunoassays.25 Similarly, antibodies such as thyroid hormone autoantibodies (THAAbs) can result in falsely elevated thyroxine levels without affecting TSH.26 27 Heterophilic antibodies are another cause of assay interference; typically, falsely elevated TSH levels are found, while thyroxine levels are unaffected.26 27 Theoretically, assays relying on streptavidin–biotin binding, estimated to be 60% of all immunoassays, are susceptible to biotin interference, used, for example, in the treatment of rare metabolic disorders such as biotinidase deficiency and propionic acidaemia).28 Results mimic hyperthyroidism, with a falsely low TSH and elevated thyroid hormones.28 However, manufacturers are increasingly producing new assays which are much less susceptible to biotin29 to substitute the current generation of assays.
Conditions mimicking the biochemical diagnosis of hyperthyroidism in clinically euthyroid individuals.
Thyroid hormone resistance.
Familial dysalbuminaemic hyperthyroxinaemia.
Biotin interference.
Antiruthenium interference.
Thyroid hormone autoantibodies.
Heparin treatment and other displacing agents.33 47
Imaging
A thyroid ultrasound scan is commonly undertaken at the time of diagnosis of thyrotoxicosis although the majority of cases are due to Graves’ disease where an ultrasound scan is unlikely to change the acute management. However, in cases where a goitre appears asymmetrical or nodular, a thyroid ultrasound may be useful. Scan appearances of diffuse echopatterns are reassuring, as it excludes the rare possibility of focal enlargement in nodular goitre.30 The National Institute for Health and Care Excellence (NICE) guidelines recommend that a technetium (Tc99m) scan should be performed if antibodies are negative.31 However, this recommendation is not commonly undertaken in children,32 as toxic nodules are rare and radiation exposure is not insignificant (1.0–1.6 mSv, equivalent to 10–16 chest X-rays).32 33 Routine technetium scans can be helpful in special circumstances such as thyrotoxicosis, possibly due to amiodarone use. An early technetium scan may differentiate between type 1 and type 2 amiodarone-induced thyrotoxicosis (AIT). While type 1 can be treated with carbimazole, type 2 requires high-dose steroids and thyroidectomy34 for which paediatric endocrine services should be contacted.
Recommendation: Perform a thyroid ultrasound scan if nodular goitre is suspected.
Treatment of thyrotoxicosis
It is common for general paediatricians to diagnose thyrotoxicosis; hence, it is important that they are aware of basic concepts underlying therapy and referral routes to specialised paediatric endocrine services. All patients with new-onset, overt thyrotoxicosis should be discussed with a paediatrician with a special interest in endocrinology or with a paediatric endocrinologist depending on local arrangements. In many cases, the specialist paediatric endocrine centre may choose to review the patient and share care with the local general paediatrician. Networked care offers high-quality clinical services through realistic and careful counselling, managing expectations, reinforcing adherence to treatment and providing follow-up.35 Families require counselling that thyrotoxicosis in children is usually more aggressive than adults36 and that carbimazole may be required for several years.37
Medical therapy
The initial treatment of thyrotoxicosis is with antithyroid drugs such as carbimazole, while longer term and more definitive therapies include radioiodine and total thyroidectomy. Propylthiouracil as a treatment alternative to carbimazole is no longer routinely used in children, due to the risk of fulminant hepatic failure.38
Carbimazole
Carbimazole is a prodrug that is converted to the active form methimazole, which in turn decreases iodination of tyrosine residues by the enzyme TPO and subsequently reduces thyroid hormone production. While carbimazole is routinely available in the UK, in other countries such as the USA, methimazole is more commonly used as first-line treatment. Treatment of thyrotoxicosis aims to restore an euthyroid state and optimise growth and neurocognitive development. Starting doses depend on severity and age of the patient. In those under 11 years, the recommended starting dose of carbimazole is 0.75 mg/kg/day (figure 3). For older children, a starting carbimazole dose of 30 mg/day is reasonable. The total daily dose of carbimazole could be spread over three divided doses but a once daily dose is preferred to promote adherence.39

{kind=link}
{kind=link}
{kind=link}
Suggested clinical pathway to initiate treatment of thyrotoxicosis with carbimazole, along with monitoring and follow-up plans. *Paediatric Formulary Committee. British National Formulary for Children London: BMJ Group, Pharmaceutical Press and RCPCH Publications, 2021.
Carbimazole: dose titration V block and replace
Historically, there have been two options when treating patients with carbimazole40: ‘dose-titration’, where the dose is adjusted to ensure an euthyroid state on a lower dose; and ‘block and replace’, where a daily dose is used that stops endogenous thyroid hormone production completely and levothyroxine is then added as a replacement dose. A randomised controlled trial40 comparing these two regimens found no difference in biochemical control in young people. This trial supported a recommendation of dose titration as the preferred option as block and replace regimens are associated with greater side effects due to the higher doses required.38 Unless extenuating circumstances suggest otherwise, a dose-titration plan should be the default treatment choice.
Carbimazole: dosing and follow-up
Carbimazole is commonly available as 5 mg or 20 mg tablets, and therefore, titration of carbimazole is advisable in multiples of 2.5 or 5 mg, for ease of administration (figure 3). During dose titration, NICE recommends the monitoring of thyroid function at 4–6 weekly intervals initially and then 3–6 monthly once stable.31 35 Initial improvement in thyroid function can be appreciated by a reduction in fT4 levels; in contrast, TSH may continue to remain suppressed for several weeks even after fT4 levels return to the normal range. Following a baseline evaluation, regular monitoring of blood counts or liver function is not required unless there is a clinical suspicion of agranulocytosis or liver dysfunction.
In children with Graves’ disease, remission rates are low and remain below 25% after 2–3 years of treatment.41 There is currently limited evidence to support an exact duration of carbimazole treatment in young people. NICE guidelines recommend reviewing the need for carbimazole treatment every 2 years.31 However, several studies have shown that a longer initial duration may reduce the of risk relapse and that remission rates of 50% can be achieved after a course of carbimazole for at least 8 years.42 In contrast, a heightened awareness of relapse is required for young children (age <5 years), those with non-Caucasian ethnicity, persistence of TRAbs and a large goitre.40 42 Individual components of the management are often influenced by patient response, relapse on treatment, specialist preference and patient choice. In addition, the decision to stop carbimazole is often guided by educational milestones, particularly in those undertaking vital academic examinations. It is worth noting that both hypothyroidism and hyperthyroidism are detrimental to cognitive functioning, reiterating the need to achieve an euthyroid state during examinations. Furthermore, perception of the quality of life can be low with antithyroid treatment3 and this might adversely influence adherence and expectations from treatment in young people. Once carbimazole is stopped, relapse is most likely to occur within 6–12 months. Therefore, all patients should be followed up closely.40 If relapse occurs, carbimazole can be restarted but with consideration given to more definitive treatment options.12
Carbimazole: side effects
Carbimazole has a range of side effects, occurring in 5%–25% of patients, as listed in table 2.37 Agranulocytosis (absolute neutrophil count<0.5×109 /L) is a major side effect, manifested by fever and a sore throat and reported in 0.2%–1.0% of patients.37 Agranulocytosis tends to occur in the first 3 months of treatment. Families should be counselled on the need to check a blood count if the child has a sore throat. If agranulocytosis is confirmed, carbimazole should be stopped immediately, with no further plan to recommence treatment. Alternative treatment should be discussed with the specialist paediatric endocrine centre and thyroidectomy should be considered after stabilisation. Occasionally, carbimazole-related generalised bone marrow suppression, hepatitis and antineutrophil cytoplasmic antibodies (ANCA) positive vasculitis can occur, widening the repertoire of side effects.37
Side effects of carbimazole and their estimated frequency3 39
Minor side effects, such as rashes, arthralgia, urticaria, nausea and headaches, may also occur during the first weeks of therapy.37 These reactions tend to be mild and transient, easily treated by an antihistaminic without the need to stop carbimazole. Another common side effect is the tendency to gain weight, resulting from slower metabolism with reducing thyroid hormone levels.12 Patients should be counselled and expectations around weight management discussed at follow-up appointments.
Treatment with carbimazole requires regular review and monitoring. Over time, it is anticipated that the natural history of Graves’ disease will tend to remission; hence, dose titration in response to biochemical change in thyroid status is appropriate and recommended.12 However, patient adherence may be problematic when carbimazole is used for prolonged periods and in adolescents with tendencies to deviate from strict adherence.
Recommendation: Carbimazole should be used as the first line therapy in the majority of cases. It should be started at an age-appropriate dose and titrated according to response. Duration of treatment and recognition of serious side effects should be discussed with the family.
Adjunctive early therapy: beta adrenergic blockers
Most children have ‘toxic’ features13 with palpitations and tremor at diagnosis. Beta-adrenergic blockers provide symptomatic relief before carbimazole takes effect and can be continued until the thyroid hormone levels have normalised (usually around 4–6 weeks). Propranolol is most commonly used. Rare side effects include alopecia, neuromuscular dysfunction, postural hypotension, psychosis and thrombocytopaenia.39 Atenolol can be used as an alternative as it has the advantage of beta-1 adrenergic receptor selectivity, and therefore, safely used in patients with asthma.
Recommendation: In children with palpitations and tremor, commence beta-adrenergic blocking agents alongside carbimazole and continue until symptoms resolve or thyroid levels normalise.
Definitive treatment choices
It is helpful to discuss alternative therapeutic choices with the family early in the course of treatment. If carbimazole or methimazole provide suboptimal response, the only remaining choices are radioiodine therapy or total thyroidectomy.
Radioiodine therapy
The aim of radioiodine therapy is to ablate the thyroid and reduce hyperthyroidism. It is usually offered only to postpubertal children, that is, 2 years postmenarche in females and slowing height velocity in males. The decision to consider radioiodine should be made by the specialist paediatric endocrine team, based on multiple factors including low adherence to carbimazole, recurrent relapse and inadequate treatment response. The dose is estimated by an ultrasound scan determined thyroid volume. The result is not always predictable and all outcomes, that is, euthyroid, hypothyroid and persistent thyrotoxic states are possible. Typically, post-treatment, thyroid function normalises within 6 months. During this time, regular follow-up is required to wean off carbimazole. In those who become hypothyroid, lifelong levothyroxine is indicated. In those with persistent thyrotoxicosis, a second dose of radioiodine, or surgical treatment, may be required.31
Cancer risk with radioiodine therapy
Given the early radiation exposure in growing children, there has been a reluctance to prescribe radioiodine in preference to surgery, even though outcomes in people <20 years old with Graves’ disease did not identify additional thyroid cancer or leukaemia.43 However, more recent evidence,44 from the UK and USA, suggests a small but significant risk of solid organ cancer in later life. It was calculated that for every 1000 patients treated with radioiodine treatment, an excess of 19 solid cancer related deaths might occur, casting doubts over long-term safety.
Recommendation: In postpubertal children, radioiodine therapy may be discussed as a definitive option, taking into account the possible increased risk in cancer in later life.
Total thyroidectomy
Young children in whom carbimazole treatment is problematic or insufficient may be offered surgery in discussion with specialised paediatric endocrine services.12 Large toxic goitres may also benefit from surgery, as radioiodine would require large radiation doses. Remission with surgery is immediate and does not pose any cancer risk, although surgical risks need to be considered. It is important to normalise the thyroid status with carbimazole before surgery. This may be assisted by the use of Lugol’s iodine (iodide with iodine) to decrease thyroid gland vascularity and reduce intraoperative blood loss as well as reducing thyroid hormone synthesis. All patients should be counselled on the complications of surgery, which include hypoparathyroidism, vocal cord paralysis and scarring.45 Thyroidectomy should only be performed in a specialist centre by a thyroid surgeon with significant experience in paediatric thyroid surgery. All patients will require levothyroxine and continued postoperative follow-up.
Recommendation: Total thyroidectomy should be offered as a definitive treatment option for children in whom carbimazole therapy is problematic or insufficient.
Further treatment options in severe thyrotoxicosis
Similar to the use in the preoperative state, oral Lugol’s iodine (iodide with iodine) can be used in severe thyrotoxicosis to avoid escalation to a crisis.39 Prednisolone can also be used as an adjunct in severe thyrotoxicosis, prior to thyroidectomy and type 2 AIT. High doses (eg, 60 mg/day) prevent conversion of T4–T3 in peripheral tissues, thereby reducing toxicity.46
Conclusions
Thyrotoxicosis in young people can be a challenging problem. The diagnosis is often made by general paediatricians who should ensure regular monitoring and follow-up of their patients in discussion with specialist paediatric endocrine centres, ideally in a shared clinical network. The treatment options for thyrotoxicosis are mostly limited to carbimazole, with long-term definitive options being either total thyroidectomy or radioiodine, the latter being associated with a small risk of solid cancers in later life.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors Concept and design: MV and IB. Drafting the manuscript: MV and IB. Revising the manuscript critically for important intellectual content: CW, LT, BH, LP and AJ. Approval of the version of the manuscript to be published: MV and IB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.