Article Text

Abstract
Background The mortality rate for children with septic shock is stil quite high in low-income and middle-income countries (31.7%). One of the most widely used scoring systems to assess mortality in sepsis or septic shock is Paediatric Logistic Organ Dysfunction 2 (PELOD-2). However, it requires various laboratory evaluations. A non-invasive, fast and easy method is needed to assess the mortality of children with septic shock at an early stage. Therefore, this study aims to evaluate the ability of Vascular Reactivity Index (VRI) compared with PELOD-2 score as a predictor of mortality in children with septic shock based on vascular response to vasoactive agents.
Methods A retrospective cohort study was conducted using data from children aged 1 month to 18 years with septic shock treated in the ER and paediatric intensive care unit (PICU) of the tertiary hospital from 2017 to 2021. The serial haemodynamic data were analysed including Systemic Vascular Resistant Index (SVRI) and the cardiac index from ultrasound cardiac output monitoring device was recorded in the first and sixth hours after the diagnosis of septic shock. The VRI was determined by dividing SVRI/Vasoactive Inotropic Score (ie, accumulated doses of dopamine, dobutamine, epinephrine, milrinone, vasopressin and norepinephrine). The receiver operating curve was used to calculate the area under the curve (AUC), sensitivity and specificity of each cut-off point.
Results A total of 68 subjects fulfilled the inclusion and exclusion criteria, the median age was 54 months with a range of 2–204 months and the mortality rate was 47%. The majority of the patients who died were found in the high cardiac index and low SVRI group (17.6%). Moreover, the optimum cut-off point of VRI was obtained to predict mortality in septic shock of 32.1, with 87.5% sensitivity and 88.9% specificity. The AUC for predicting death using VRI was 95% (95% CI 90% to 100%, p<0.001) and PELOD-2 92.6% (95% CI 96.4% to 98.8%, p<0.001).
Conclusion The VRI <32.1 may potentially be used to predict mortality in children with septic shock and its predictive ability is as good as PELOD-2. The assessment of VRI is faster and easier than PELOD-2.
- Mortality
- Resuscitation
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Case fatality rate (CFR) in paediatric severe sepsis and septic shock was higher in low-income and middle-income countries.
WHAT THIS STUDY ADDS
In septic shock, systemic vasodilation occurs, which correlates with the severity and response to therapy.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Calculation of Vascular reactivity index (VRI) using ultrasound cardiac output monitoring is less invasive method to predict mortality in paediatric septic shock
Introduction
Paediatric septic shock is associated with high mortality globally, according to a recent systematic review and meta analysis of global case fatality rates (CFR) in paediatric severe sepsis and septic shock, the CFR was higher in low-income and middle-income countries with 31.7% (95% CI 27.3% to 36.4%) compared with high-income countries with 19.3% (95% CI 16.4% to 22.7%, p<0.001).1 The International Consensus Conference on Pediatric Sepsis defines sepsis as a life-threatening organ dysfunction caused by dysregulated host response to infection. Meanwhile, septic shock is defined as a progression of sepsis with circulatory, metabolic and cellular abnormalities that can substantially increase mortality.2 Sepsis in children can cause hypotension and shock through vasodilation, hypovolaemia, decreased myocardial function or a combination of two or more of these mechanisms. Decreased perfusion causes dysfunction or failure of several vital organs, including the kidneys, lungs, liver, brain and heart, which potentially lead to death.3–5
Several scoring systems have been developed to predict mortality in paediatric sepsis or septic shock, for example, Paediatric Logistic Organ Dysfunction-2 (PELOD-2) scores.6–8 The test are relatively expensive because it requires various laboratory evaluations and the process of taking blood samples makes children uncomfortable. Therefore, less invasive, easy and fast methods are preferable to predict mortality in paediatric sepsis.
Lee et al9 developed the calculation of Vascular Reactivity Index (VRI) as a non-invasive method to predict mortality in children with refractory septic shock. The VRI value was determined by dividing Systemic Vascular Resistant Index (SVRI)/Vasoactive Inotropic Score (VIS).9 It represents the vascular response to vasoactive agents, while, the vascular endothelium is considered to be a key organ involved in the pathogenesis of the host response in sepsis and one of its main functions is to control arterial tone.9 10 In septic shock, systemic vasodilation occurs, which correlates with the severity and response to therapy. In clinical practice, this can be evaluated by the use of vasopressors and lowering blood pressure. A low systemic vascular resistance index reflects systemic vasodilation.9 Therefore, the primary objective of this study was to evaluate the potential of VRI as a predictor of mortality in children with septic shock compared with the PELOD-2 score. The secondary objectives included describing the haemodynamic patterns of paediatric patients with septic shock and determining the correlation between VRI and PELOD-2 score.
Methods
The sampling was carried out retrospectively on patients aged from 1 month to 18 years old and the data were collected from January 2017 to June 2021. The patients had been diagnosed with septic shock and admitted to the ER and PICU of Cipto Mangunkusumo Hospital. Septic shock was defined based on The International Consensus Conference on Pediatric Sepsis as a condition marked with persistent cardiovascular dysfunction following adequate fluid resuscitation of 40 mL/kg intravascular in <1 hour, characterised by the use of vasopressors.2 Inclusion criteria were paediatric patients aged 1 month to 18 years with International Classification of Diseases (ICD) 10 administrative coding of septic shock (R65.21). The exclusion criteria were: (1) patient transferred out to another hospital; (2) patients with congenital heart defects, (3) hospital length of stay<6 hour including those who died or were transferred to another hospital and (4) incomplete information to calculate VRI and PELOD-2. All management algorithms were based on Indonesian Pediatric Society guidelines which referred to Surviving Sepsis Campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children.11 12
The medical record data were accessed through an electronic database using the keyword septic shock (R65.21) based on the ICD 10 administration coding. Subsequently, the medical records were open to collect the data. The data evaluated were demographics, medical/surgical diagnosis, physical examination, as well as laboratory data needed for PELOD-2 score during a 6-hour sepsis diagnosis, shock stage, vasoactive drugs, VRI, PICU length of stay and mortality outcome. The optimal cut-off point for PELOD-2 score was ≥11 based on Indonesian Pediatric Association. Also, haemodynamic monitoring measurements such as preload parameters (stroke volume variation), cardiac contractility (cardiac output, cardiac index and minute distance) and afterload (SVRI) were evaluated using ultrasound cardiac output monitoring (USCOM) at first and sixth hours after therapy.
VRI is defined as SVRI/VIS. VIS is calculated based on the highest dose of vasoactive and inotropic drugs used within the first 6 hours since the septic shock diagnosis. The value of VIS is calculated as follows dopamine dosage (μg/kg/min) + dobutamine dosage (μg/kg/min) + 100 × epinephrine dosage (μg/kg/min) + 10 × milrinone dosage (μg/kg/min) + 10 000 × vasopressin dosage (U/kg/min) + 100 × norepinephrine dosage (μg/kg/min).13
The sample size was calculated using the diagnostic value cut-off point estimation (one-way hypothesis) test, with 5% significance, absolute accuracy of 10%, and expected sensitivity of 90%. The minimal sample size calculated was 48. All Data were analysed with SPSS V.23.0 software. Descriptive data were presented as frequency and percentage, while the discriminative value of VRI was obtained using receiver operating characteristic (ROC) curve and expressed as area under the curve (AUC). Discriminatory power of 90%–100% was considered excellent. The accuracy of predicting mortality for VRI was also assessed by calculating the sensitivity, specificity, negative predictive value, positive predictive value, positive likelihood ratio (LR+) and negative likelihood ratio (LR−). Furthermore, Spearman’s rank correlation test for the non-normal distribution of data was conducted to determine the correlation between VRI and PELOD-2, while the risk ratio value to mortality was analysed with Fisher’s exact test for unmet minimum expected value in cross-distribution between VRI and PELOD-2. Results with p<0.05 were considered to be statistically significant with 95% CI.
Results
A total of 190 subjects diagnosed with septic shock were admitted to the emergency room (ER) and PICU of Cipto Mangunkusumo Hospital between January 2017 and June 2021. Seventy subjects with congenital heart disease were excluded as well as 38 with incomplete data, and 14 were screened doubly. Consequently, 68 subjects were included in the final analysis. The demographic characteristics are described in table 1. The majority of the patients were male with 60.3%, while 51.4% were aged 5 years, and the medical diagnoses of 91% were more frequent than surgical of 9%. The median age was 54 months with a range of 2–204 and the highest number was found in the 13–60 month age group, namely 36.8%. In addition, the overall patient mortality was 47%.
Characteristics of subjects
One of the targets for septic shock is cardiac index value of 3.3–6 L/min/m2. In this study, the subjects were divided into three groups according to cardiac index classification namely low cardiac index with <3.3 L/min/m2, normal cardiac index ranging from 3.3 to 6 L/min/ m2 and high cardiac index >6 L/min/m2.14 The highest number of subjects who died was found in the high cardiac index and low SVRI group with 17.6%. The baseline haemodynamic profile was also described from the USCOM, including cardiac index and SVRI at the time of septic shock diagnosis, as shown in table 2.
Baseline cardiac index and SVRI values in paediatric septic shock
ROC analysis was used to evaluate the performance of VRI as a predictor of mortality. The AUC of VRI was 95% (95% CI 90% to 100%, p<0.001) to predict mortality as shown in figure 1. The optimal cut-off point was obtained from the intersection between sensitivity and specificity by observing the AUC value and determining the coordinates from the ROC curve (figure 2). VRI score of ≤32.1 was shown to be the optimum cut-off point with 87.5% sensitivity and 88.9% specificity.
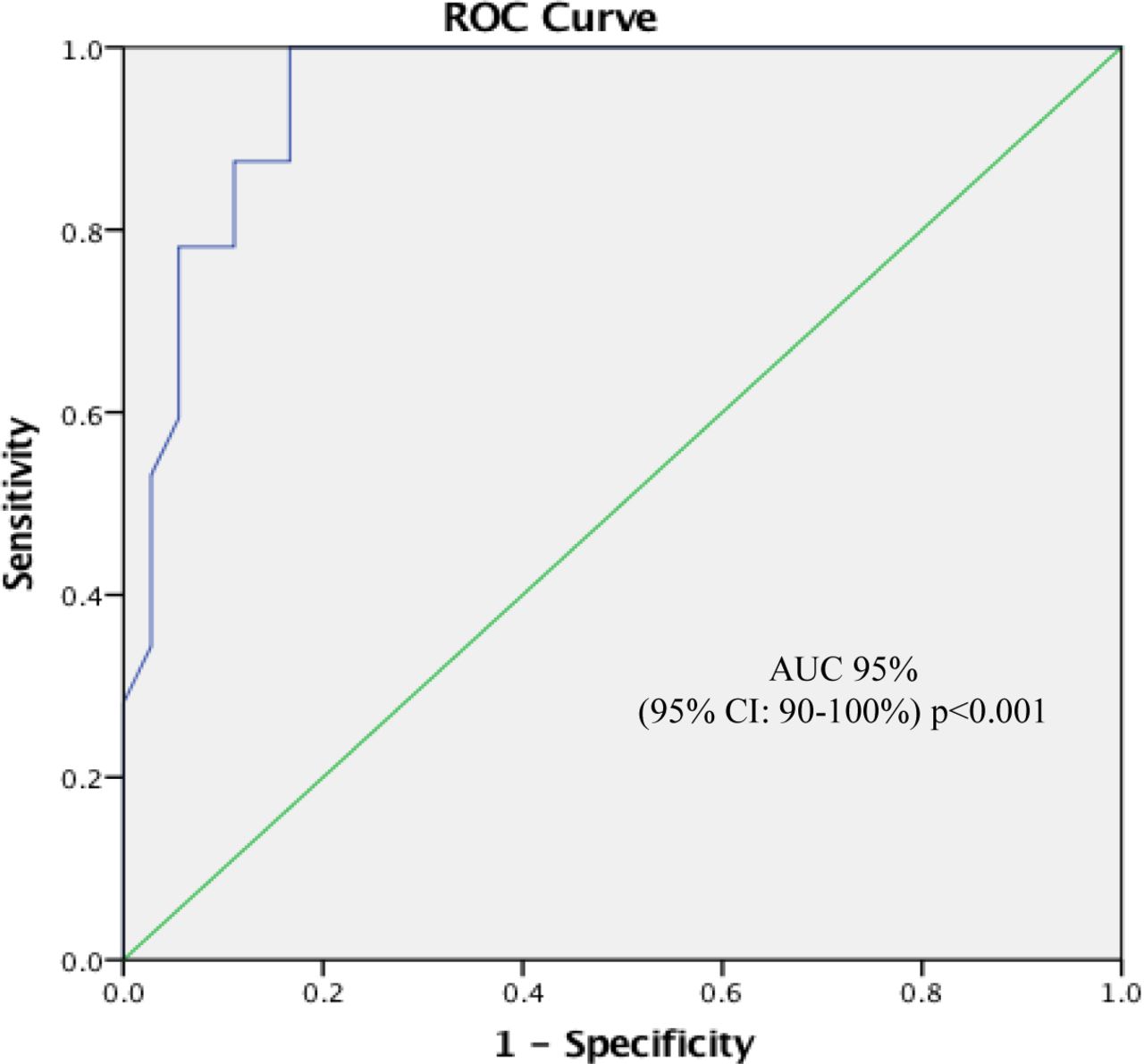
ROC curve of Vascular Reactivity Index in predicting mortality in paediatric septic shock. ROC, receiver operating characteristic.
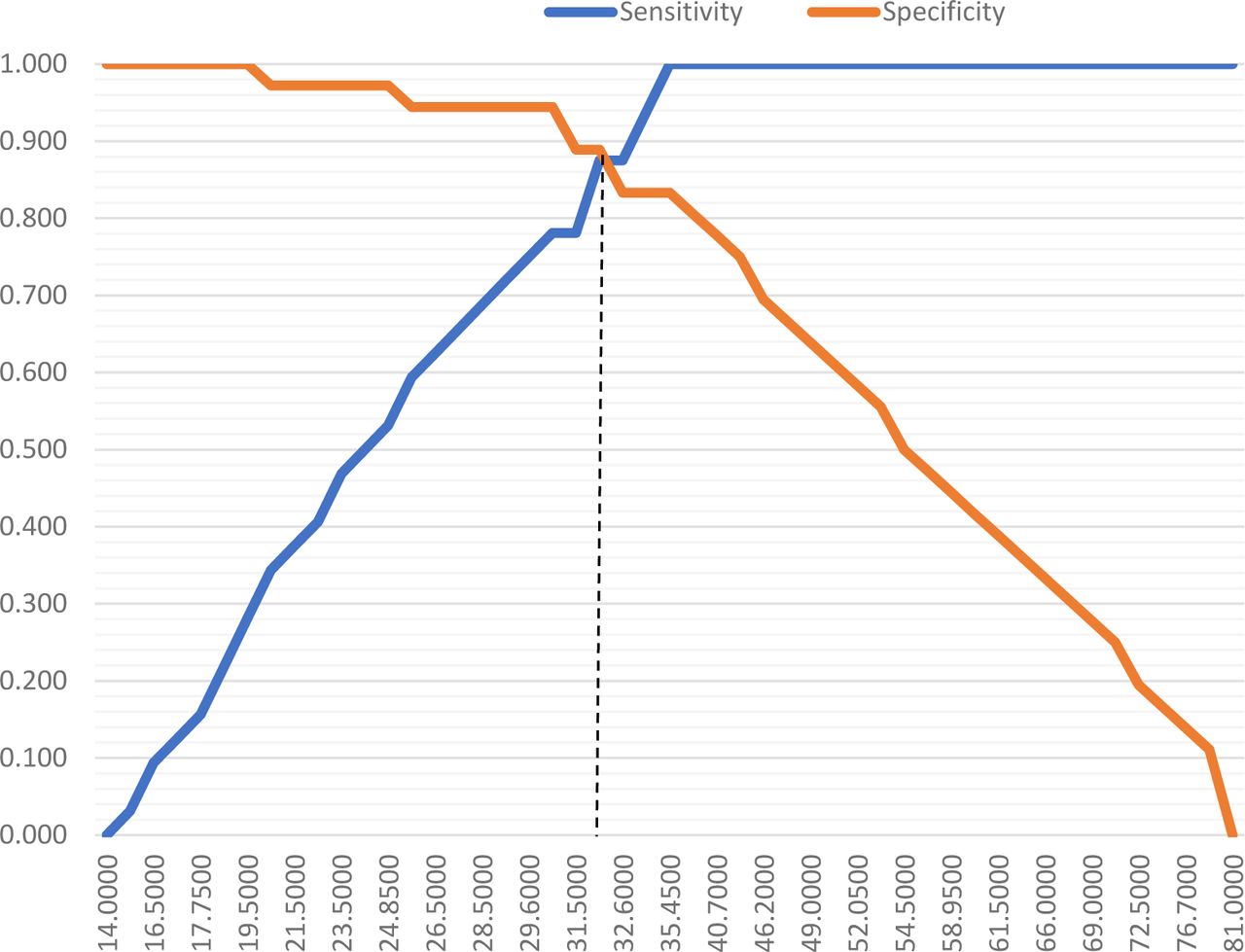
Cut-off point curve of VRI in paediatric septic shock mortality. VRI, Vascular Reactivity Index.
VRI and PELOD-2 were analysed in accordance with mortality incidence (table 3). PELOD-2 score of ≥11 was used based on the consensus guidelines for diagnosis and management of sepsis in children from the Indonesian Pediatric Association. Patients with VRI ≤32.1 had a higher mortality risk than VRI >32.1 (RR 7.87, 95% CI 3.09 to 20.02, p<0.001). Similarly, PELOD-2 ≥11 had a higher mortality risk than PELOD-2 <11 (RR 2.44, 95% CI 1.67 to 3.57, p=0.001).
The relationship between VRI, PELOD-2 and mortality in paediatric septic shock
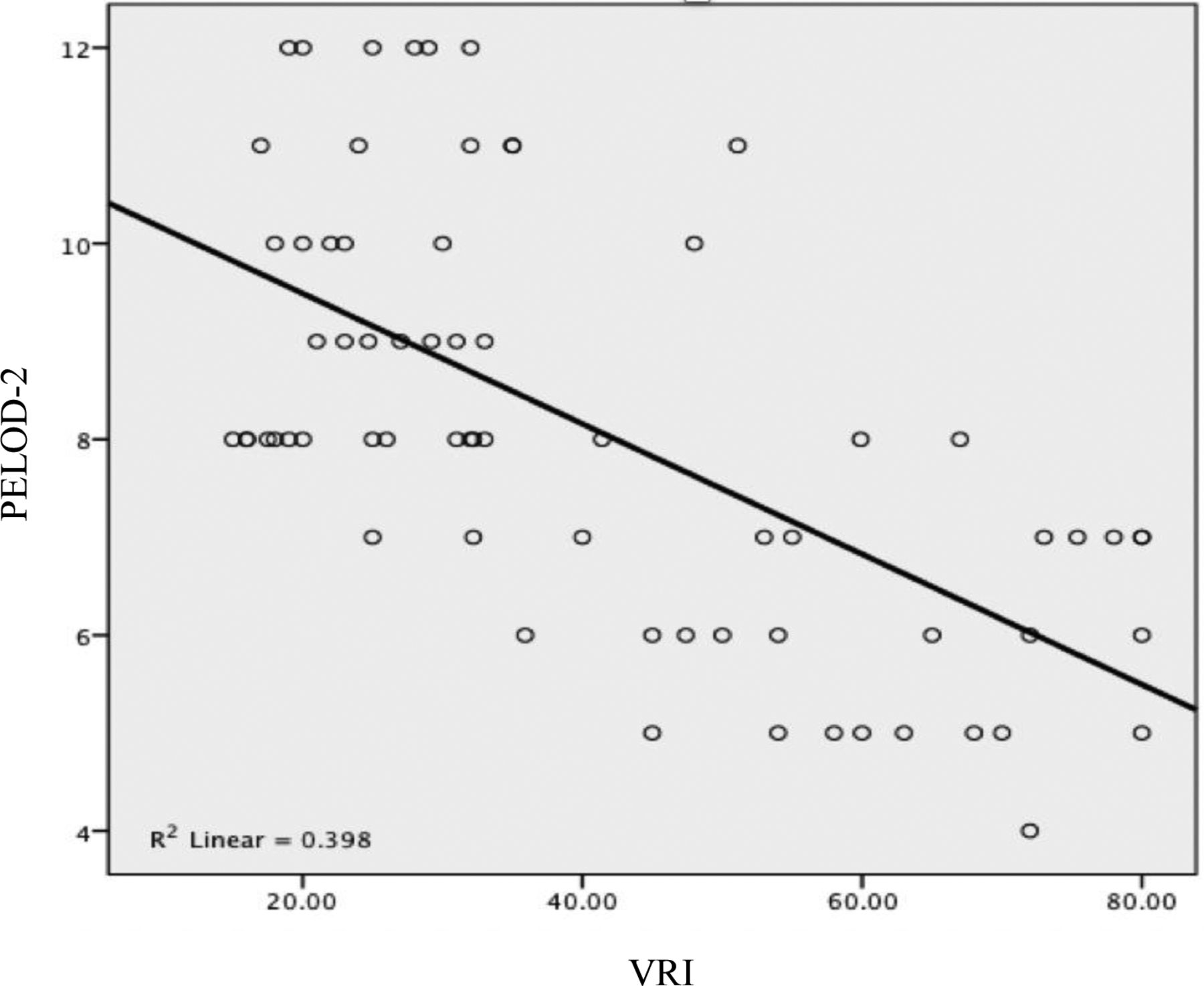
Correlation analysis between VRI and PELOD-2 is represented graphically by the scatter diagram (figure 3). A statistically significant negative relationship was observed between VRI and PELOD-2 (r=0.627; p<0.001). The prognostic accuracy of VRI and PELOD-2 is described in table 4. The AUC of VRI was 95% with 95% CI 90% to 100%, p<0.001, and was as good as the AUC of PELOD-2 of 92.6% with 95% CI 86.4% to 98.8%, p<0.001.
{kind=link}
{kind=link}
{kind=link}
Negative linear relationship between VRI and PELOD-2. PELOD-2, Paediatric Logistic Organ Dysfunction 2; VRI, Vascular Reactivity Index.
Discriminative value of VRI and PELOD-2 in predicting mortality in paediatric septic shock patients
Discussion
The results suggest that VRI can be used to predict mortality in paediatric septic shock. The majority of subjects were in the 13–80 months age group. Most of the patients had come in critical condition, which caused the majority of PICU length of stay to be less than 7 days (54.4%) because some of them did not survive. This illustrates that Indonesia as a low and middle income country still has a high mortality rate due to septic shock in the paediatric group.
In septic shock, there are complex cardiovascular responses and changes in vascular tone that vary from individual. These conditions are critical for survival. The adult population usually manifests haemodynamic patterns of high cardiac index and low SVRI (hyperdynamic), while data are limited for children, but a greater proportion showed low cardiac index and high SVRI (hypodynamic). Adults can maintain high cardiac output through dilated ventricles and increased heart rate, while children have limited capability to improve these conditions.15 16 Furthermore, the baseline haemodynamic profile of patients was very diverse as shown in table 2. The highest number of subjects who died was in the high cardiac index and low SVRI group (17.6%). A study by Bierley et al15 in England also found more haemodynamic patterns of high cardiac index and low SVRI (94%) in septic shock children with the source of infection from a central venous catheter, while sepsis from community origin had a low cardiac index with varying SVRI (14%).15 Moreover, Lee et al17 analysed haemodynamic parameters to identify predictors of mortality in children with septic shock and cardiogenic shock.17 The study used a transpulmonary thermodilution technique through the pulse-induced cardiac output. The result showed that SVRI was significantly lower in children with septic shock who died compared with those who survived. The SVRI value for children who died was 901.08±305.69 compared with 1584.23±429.63 in survived children, with p<0.001. Meanwhile, the cardiac index was a predictor of mortality in the cardiogenic shock group.17
Another haemodynamic pattern was found as 16.1% of patients were in the normal cardiac index and SVRI group, indicating that compensated shock still occurred. A compensated shock phase was also observed in the low cardiac index and normal SVRI group of 16.1% in which normal vascular tone was maintained due to activation of the sympathetic system in the hypotensive state. Conversely, in the low cardiac index and SVRI groups of 8.8%, the patients were in a prolonged shock condition, hence, compensatory mechanisms failed to work which led to death.
The concept used in the VRI assessment was the occurrence of endothelial dysfunction in sepsis which causes the formation of reactive oxygen species, activation of complement systems, platelet aggregation and various cytokines. Multiple endothelial dysfunction reflects microvascular perfusion abnormalities and associated organ dysfunction. In septic shock, systemic vasodilation can occur which correlates with the severity and response to therapy.9 18
The VRI cut-off point of ≤32.1 correlated with higher mortality in children with septic shock. This supports a previous study by Lee et al9 that demonstrated the usefulness of VRI as a predictor of mortality in children with refractory septic shock. Lee et al9 assessed serial VRI at 6-hour intervals in the first 72 hours after PICU admission in a child with septic shock. The mean AUC within the first 72 hours was 0.8, and the serial values of VRI were significantly lower in the mortality group than in the survival group during the period from 0 to 48 hours. It was found that the VRI cut-off point <30 had good predictive power of mortality with an average AUC>80%, sensitivity 85%, specificity 77%, LR+3.7, LR− 0.2.9 Low VRI value suggests that systemic vascular reactivity had the worst response towards the vasoactive-inotropic agents and reflects the high mortality rate in children with septic shock. The differences in the cut-off point with the study of Lee et al9 are presumably due to the variation in the sample size.
The significance of predictive accuracy between VRI and PELOD-2 to mortality was analysed with Fisher’s exact test. It showed that both parameters were significant mortality predictors with p<0.001. The RR value for VRI ≤32.1 was higher 7.87 (95% CI 3.09 to 20.02) compared with PELOD-2 ≥11 which was 2.44 (95% CI 1.67 to 3.57). These data were considered because the component of PELOD-2 scoring is a biomarker of tissue dysfunction in microcirculation. Meanwhile, microcirculation biomarkers change more slowly due to hypoxia in shock, while the USCOM device is used to obtain VRI value and assesses macrocirculation in real-time. Disturbances in macrocirculation influence microvascular and related organ dysfunction. Thus, VRI can be used to detect organ dysfunction earlier than PELOD-2. The haemodynamic monitoring is also crucial in making appropriate decisions for the management and prognosis of paediatric septic shock. Therefore, USCOM is very useful because it is a non-invasive procedure in assessing haemodynamic components such as preload, contractility and afterload.19 20 Dhanani et al21 confirmed the reliability of intraobserver and interobserver about cardiac output measurement for the paediatric by using USCOM. Intraobserver reliability was considered by the coefficient of Lin concordance correlation of 0.92 and 0.85. The average differences±in SD by interobserver were 0.16±0.59 L/min/m2 and the coefficient of Lin’s concordance correlation was 0.87.21 22
This study has several limitations especially in relation to the retrospective method used which relies on medical records. However, all management algorithms were based on Indonesian Pediatric Society guidelines which referred to Surviving Sepsis Campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children, thereby minimising subjectivity in determining management. In addition, there are not a lot of studies on VRI in children with septic shock. The current meta-analysis study only conducted at adult populations, and there are insufficient data to quantitatively evaluate the relationship between vascular reactivity and multiple organ failure development.10
Conclusion
The VRI is a good predictor of mortality in children having septic shock with a cut-off point of ≤32.1 and its predictive ability is as good as PELOD-2. The assessment of VRI is faster and easier than PELOD-2.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Committee for Health Research, University of Indonesia, Faculty of Medicine KET.608/UN2.FI/ETIK/PPM.00.02/2021.
Acknowledgments
The authors would like to thank all those who assisted in the study.
References
Footnotes
Contributors IY, UKS, SOP, MK, ATPI and YP conceived the study. IY, UKS and SOP collected and analysed data. IY and UKS drafted the manuscript. UKS as guarantor. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.