Article Text

Abstract
Objective To determine the effect of continuous wound infusion of local anaesthetic drug (bupivacaine) on total amount of systemic opioid use in the first 72 hours in newborn infants undergoing laparotomy.
Design A two-arm parallel, open-label randomised controlled trial.
Setting A quaternary newborn intensive care unit.
Patients Infants>37 weeks of gestation undergoing laparotomy for congenital or acquired abdominal conditions.
Interventions Continuous wound infusion of local anaesthetic (bupivacaine) for the first 72 hours along with systemic opioid analgesia (catheter group) or only systemic opioid analgesia (opioid group).
Main outcome Total amount of systemic opioid used within the first 72 hours post laparotomy.
Results The study was underpowered as only 30 of the expected sample size of 70 infants were enrolled. 16 were randomised to catheter group and 14 to opioid group. The two groups were similar at baseline. There was no significant difference between the groups for the primary outcome of median total systemic opioid use in the first 72 hours post laparotomy (catheter 431.5 µg/kg vs opioid 771 µg/kg, difference −339.5 µg/kg, 90% CIhigh 109, p value 0.28). There was no significant difference between the groups for any of the secondary outcomes including pain scores, duration of mechanical ventilation, time to reach full feeds and duration of hospital stay. There were no adverse events noted.
Conclusion Continuous wound infusion of local anaesthetic along with systemic opioid analgesia is feasible. The lack of a difference in total systemic opioid use in the first 72 hours cannot be reliably interpreted as the study was underpowered.
Trial registration number ACTRN12610000633088.
- Pain
- Neonatology
Data availability statement
Data are available upon reasonable request. If individual level data are required for a meta-analysis, that will be provided on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In adult and paediatric patients, the administration of continuous infusion of local anaesthetics through catheters placed into the surgical wound has become increasingly popular due to its simplicity, efficacy and safety.
There are no randomised controlled trials (RCT) directly comparing continuous wound infusion of local anaesthetic with current standard of care (opioids) in newborn infants.
WHAT THIS STUDY ADDS
This RCT found that continuous wound infusion of local anaesthetic along with systemic opioid analgesia is feasible.
The lack of a difference in total systemic opioid use in the first 72 hours after abdominal surgery cannot be reliably interpreted as the study was underpowered.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study provides feasibility data for a large multicentre RCT.
Introduction
Systemic opioids are commonly used to provide analgesia post surgery in newborn infants; however, they may cause respiratory depression, hypotension, withdrawal syndrome and possible harmful effect on the newborn brain.1 2 Intravenous paracetamol often used for its opioid-sparing effects after major abdominal surgery may cause hepatic and renal impairment in addition to its potential effect on neurodevelopment.3–5 Continuous infusion of epidural chloroprocaine in infants following abdominal surgery provides adequate analgesia, shortens time to tracheal extubation and may limit exposure to systemic opioid medications.6 However, the risk of procedure and drug-related complications to the developing neural structure remains a serious concern.7
In adult and paediatric patients, the administration of continuous infusions or intermittent boluses of local anaesthetics through catheters placed into the surgical wound has become increasingly popular due to its simplicity, efficacy and safety.8 In two phase 1 prospective studies in newborn infants, the authors reported plasma levels of levobupivacaine well below potentially toxic levels, adequate wound healing and pain scores consistent with adequate analgesia.9 10 In both these studies, all the babies had continuous wound infusion of levobupivacaine and intravenous opioids combined. There are no randomised controlled trials (RCTs) directly comparing continuous wound infusion of local anaesthetic with current standard of care (opioids) in newborn infants. This trial was designed to determine the effect of continuous wound infusion of local anaesthetic (bupivacaine) on total amount of systemic opioid use in the first 72 hours in newborn infants undergoing laparotomy.
Methods
Setting
This is a two-arm parallel, open-label RCT conducted in a quaternary surgical neonatal intensive care unit in Australia between 1 September 2017 and 31 December 2021. The trial was registered with the Australia New Zealand Clinical Trials Registry, ACTRN12610000633088.
Subjects
All infants>37 weeks of gestation (if born preterm then after reaching 37 weeks post menstrual age) who underwent laparotomy for congenital or acquired abdominal conditions and who were likely to be admitted for at least 72 hours were included.
Exclusion criteria were abdominal surgeries performed laparoscopically, newborns who were enrolled once in the study but who are undergoing another laparotomy for the same or different surgical condition, any absolute contraindication to wound catheter placement and documented severe liver dysfunction, that is, International Normalised Ratio (INR) >2.5, liver enzymes>3 times the normal.
Randomisation
Random sequence with variable block sizes of 2,4,6 was generated using a random number generator with ‘R’ statistical software. The random allocations were each written on a sheet of paper and kept in sequentially numbered sealed opaque envelopes. After obtaining consent, the research team allocated the baby to one of the groups by selecting the least numbered envelope. The envelope was opened prior to the infant going to the operating room.
Intraoperative management of both groups
Anaesthesia was conducted according to current standards of care. Muscle relaxation (vecuronium or cisatracurium), ventilation and intraoperative opioid analgesia were administered at the discretion of the anaesthetist.
Intervention
Catheter group
At the conclusion of surgery, when the incision was closed, the transversus abdominis muscle with/without the peritoneum was closed first. The multiorifice 19-gauge wound catheter (Halyard On-Q Silver soaker catheter) was placed superficial to this layer but deep to the internal oblique so that the local anaesthetic delivered can come in close contact with the nerve endings.9 The ‘drug delivery length’—either 2.5 or 6.5 cm—was selected according to the length of the surgical incision. The internal oblique and external oblique muscles were closed in one layer on top of the wound catheter. A transparent dressing was applied on the skin. Immediately after skin closure, following a negative aspiration test to confirm that the tip of the catheter was not inserted intravenously, a bolus dose of bupivacaine (0.3 mL/kg 0.25% bupivacaine) was administered through the wound catheter in babies who were randomised to the treatment group.
The catheter was capped until return to the unit and was connected to a continuous infusion of bupivacaine (0.125%) after 4 hours from the surgery at the rate of 0.2 mg/kg/hour (0.16 mL/kg/hour) for 72 hours. The wound catheter was removed at the end of 72 hours at the bedside by the nursing staff.
Control group
There was no catheter inserted and no wound infusion in the control group.
Management of postoperative pain for both the groups
Newborns in both groups were started on an intravenous morphine infusion at the rate of 10 µg/kg/hour or intravenous fentanyl infusion at the rate of 1 µg/kg/hour. The modified Pain Assessment Tool (mPAT) was used to score the infant’s level of discomfort (table 1). The frequency of assessment was every 2 hours for first 24 hours, every 4 hours for next 48 hours and every 2 hours after a change in dose of analgesia. The pain scoring was continued until opioids had been ceased for at least 48 hours. The adjustment of opioid infusion was based on the infant’s mPAT Score. If mPAT Score was >10, a bolus of 50–100 µg/kg was administered and/or morphine infusion was increased by 2 µg/kg/hour or as felt clinically appropriate. If the baby was on fentanyl infusion, a bolus of 2 µg/kg was administered and/or fentanyl infusion was increased by 0.2 µg/kg/hour or as felt clinically appropriate. If score was <5 for more than or equal to 2 hours, then morphine infusion was decreased by 2 µg/kg/hour. If the baby was on fentanyl infusion, fentanyl infusion was decreased by 0.2 µg/kg/hour.
Modified Pain Assessment Tool (mPAT)
Outcome
The primary outcome included cumulative amount of intravenous opioid per patient per kg of body weight during the first 72 hours following the surgery. If the baby received a fentanyl infusion and/or intermittent boluses, they were converted to an equivalent dose of morphine using the conversion ratio of 10:1 .11
The secondary outcomes included pain scores in the first 72 hours after laparotomy, number of babies requiring rescue opioid boluses, the cumulative amount of oral morphine received during the hospital stay, the need for oral morphine at the time of discharge home, the cumulative amount of enteral/parenteral paracetamol given for analgesia, duration of mechanical ventilation, duration of hospital stay, number of babies with hypotension (defined as the mean arterial pressure less than gestational age of the baby) requiring inotropic support, number of babies who required reintubation after extubation in the operating room, number of babies still ventilated at the end of 72 hours postoperatively and time (in hours) to reach feeds of 120 mL/kg/day from the time of surgery. Long-term neurodevelopmental outcomes will be collected at 1 and 3 years and will be published separately.
The incidence of side effects of opioids was collected including the need for bladder catheterisation to assist urine drainage, incidence of postoperative ileus, defined as bilious aspirates with failure to pass meconium/stools after surgery, incidence of postoperative vomiting, need for oral opiates at the time of discharge.
The incidence of side effects of the presence of a wound catheter included laparotomy wound infection, defined as erythema of wound edges where the surgical team/neonatologists started antibiotics, accidental removal of wound catheter, leakage of bupivacaine out of the laparotomy wound, local irritation/redness at the laparotomy site and catheter obstruction necessitating removal.
Incidence of side effects of bupivacaine including cardiac arrhythmia and seizures.
Parent and public involvement
Parents or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Sample size
The mean intravenous morphine infused over a period of 72 hours in 182 babies post laporotomy in our unit was 416 µg/kg with an SD of 326 µg/kg. A difference of 83 µg/kg (20%) or lower was not considered clinically relevant. A sample size of at least 35 per group will have 80% power at 10% one-sided alpha to rule out a difference in means of 83 µg/kg or lower, assuming the true difference was at least 250 µg/kg (60%) and an SD of 326 µg/kg. A one-sided test was used as the intervention arm also included the same starting dose of systemic opioids as the control arm and we were interested if the intervention arm was effective at lowering overall opioid amount.
Statistical analysis
All continuous data are described as medians (IQR) and categorical data are expressed as counts and percentages. All analyses were performed following the intention-to-treat principle. Comparisons for continuous variables were made with a two-sample t-test or Wilcoxon rank sum test, and for categorical variables X2 test or Fisher exact test, as appropriate. Differences are described as median differences with 90% CIs for continuous variables and risk ratios 90% CIs for binary variables. Regression analysis to investigate confounders of the treatment effect was not considered due to the small sample size. A post-hoc analysis investigating the effect of local wound analgesia based on the underlying diagnosis (congenital diaphragmatic hernia (CDH) vs no CDH) and cumulative use of opioid per day over the first 3 days between the two groups was performed. Statistical analysis was conducted using ‘R’ and Stata V.14.2 (StataCorp). A p value of <0.1 was considered statistically significant for all analyses.
Results
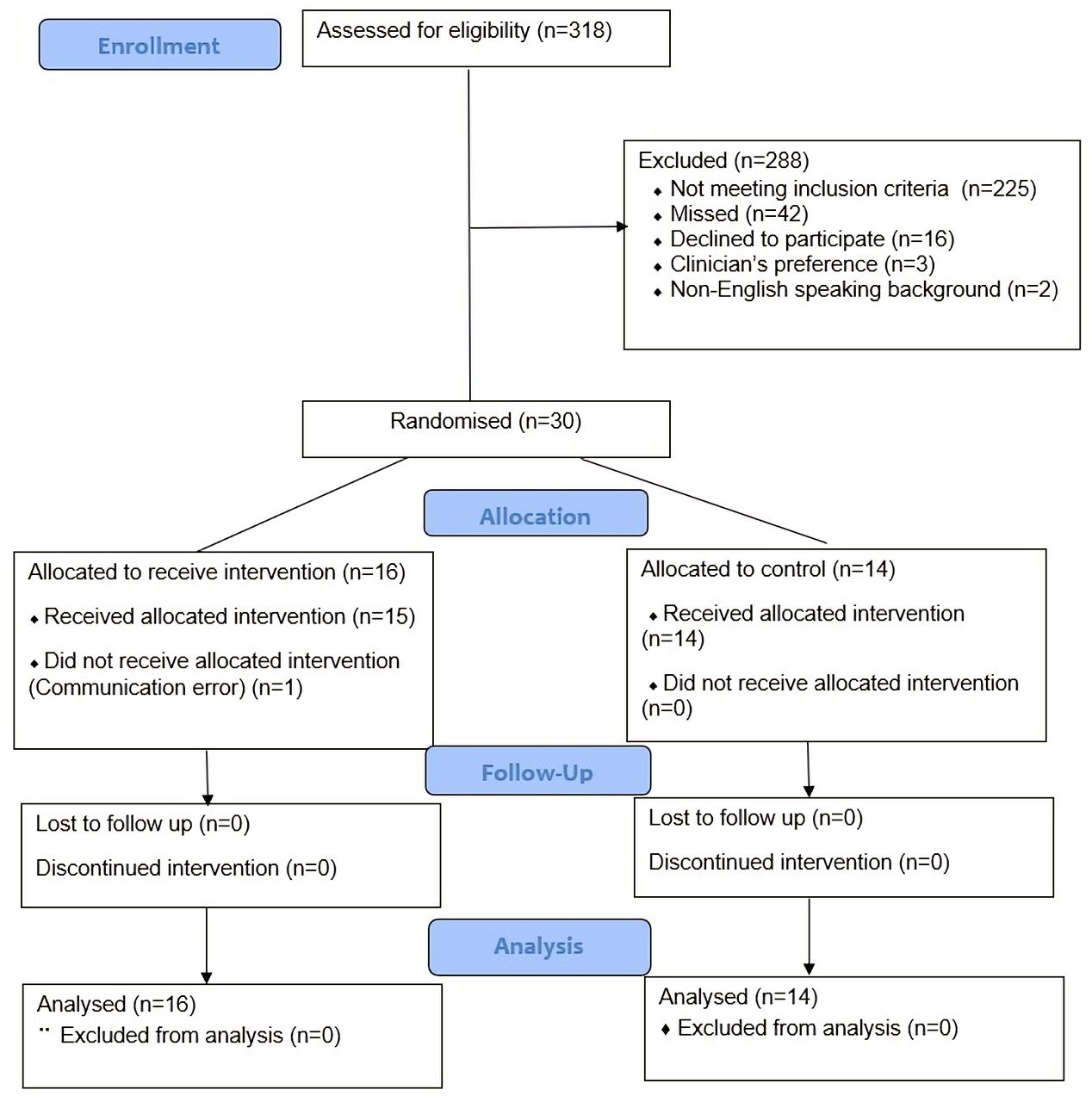
Overall, 30 infants were enrolled in the CANWIN Study, 16 infants randomised to the catheter group and 14 infants to the control group. The trial was stopped early due to slow recruitment. Numbers and reasons for non-enrolment and losses are given in figure 1. All the infants received the intended treatment except one infant randomised to the catheter group who received only systemic opioid due to a communication error. This baby was analysed in the catheter group.

{kind=link}
Consort Flow Diagram of the CANWIN Study.
The baseline demographic characteristics of the two groups were similar (table 2). Half (15/30) of the infants enrolled had CDH.
Baseline demographics of the study groups
Primary outcome
The median cumulative opioid in the first 72 hours post surgery was 431.5 µg/kg (IQR 241–1174) in the catheter group and 771 µg/kg (IQR 406–1010) in the control group (table 3). The difference between the groups for the primary outcome of cumulative systemic opioid use in the first 72 hours post laparotomy (−339.5 µg/kg (90% CIhigh 109, p 0.28)) was however not statistically significant. A post-hoc analysis looking at the effect of local wound analgesia based on the underlying diagnosis (CDH vs no CDH) did not reveal any differential effect (table 3). Opioid use on day 1, day 2 and day 3 did not differ between the two groups (table 4).
Primary outcome for the two study groups and by underlying diagnosis
Opioid use at 24, 48 and 72 hours between the groups
Secondary outcomes
Table 5 shows the secondary outcomes between the two groups. There were no significant differences in any of the outcome assessed. Pain scores were similar for both groups. There were no significant differences for side effects related to opioids including the need for bladder catheter (catheter group 4 (25%) vs opioid group 5 (36%)) or inotropes (catheter group 4 (25%) vs opioid group 8 (57%)). Only one baby developed wound infection in the opioid group. No babies required reintubation at the end of 72 hours if extubated and there was no postoperative ileus. No babies were discharged on oral morphine. No adverse effects were observed including seizures or arrhythmia related to bupivacaine. There was no accidental removal of a catheter or excessive leakage, wound redness or increased rates of infection in the catheter group.
Secondary outcomes for the study groups
Discussion
Continuous local anaesthetic wound infusion of bupivacaine is feasible. Despite the observed reduction in median opioid dose of almost 340 µg/kg, the lack of statistical evidence for its effect on the amount of systemic opioid use in the first 72 hours post laparotomy cannot be interpreted as the study was underpowered.
Our findings are similar to one other RCT in 34 older infants, where wound infiltration with bupivacaine had no significant effect on the mean fentanyl requirement (1 µg/kg in bupivacaine arm vs 0.5 µg/kg in control arm, p value 0.25) during the first 24 hours after major abdominal surgery.12 This study, such as ours, could only enrol 34 infants instead of their calculated sample size of 266 infants. The infants enrolled were however older with a mean (SD) age of 3.55 (2.47) months and mean weight of 5.4 (1.7) kg in the intervention arm. The authors used just one bolus dose of bupivacaine intraoperatively rather than continuous infusion in the postoperative period.
It is possible that one of the reasons for the lack of significant difference in the opioid use between the two groups in our study may have been due to babies with CDH making up to 50% of the study population. Opioid use in babies with CDH is dictated not only by postoperative pain but also by the need to provide analgesia for ongoing ventilation and slow weaning to prevent opioid withdrawal. All the babies with CDH were on opioid treatment prior to surgery, and hence the weaning may have been slower to prevent withdrawal as per the local pain policy.13 Future trials investigating local wound analgesia should consider not including babies with CDH.
There were only three babies with malrotation (two in the catheter group and one in the control group) enrolled in the study. Babies with malrotation are often well at birth and present with bilious vomiting in the first few days of life.14 Once the diagnosis is made after birth, surgery is often needed within hours of diagnosis. The emotional and physical distress of the parents complicates the consent process and approaching parents in such a stressful situation is challenging.15 16 There is a risk of babies presenting with surgical emergency being excluded from prospective research as in this study. Alternative consent processes such as deferred consent or waiver of consent such as those used in delivery room intervention trials needs to be explored for intervention trials in newborns with surgical emergencies.17
One could argue that by including systemic opioids along with the local wound analgesic infusion in the intervention arm, we may have diluted the opioid sparing effect of the intervention; however, we found it unethical to withholding opioids from the babies randomised to the catheter group if the local wound analgesic infusion would have proven to be ineffective. There is evidence that nearly three-quarters of the trials for new analgesic treatments for neonates undergoing procedural pain did not supply the necessary analgesia for all subjects.18 There are growing calls to parents, ethics review boards and medical journals to refuse studies that do not provide acceptable analgesia to all babies enrolled in studies.18
The strength of the current study is its design as an RCT. All the babies enrolled received adequate analgesia. There was no loss to follow-up. The study was performed in a surgical setting randomising babies presenting with surgical emergencies. The observed reduction in median opioid dose of almost 340 µg/kg in the catheter group though statistically non-significant is clinically significant. The limitations are the early stopping of the trial due to poor enrolment, and thus lack of power to detect a significant difference. The COVID-19 pandemic impacted enrolment along with the challenge to obtain consent from parents of babies presenting with a surgical emergency. Compliance to the protocol in terms of increasing or weaning of opioid infusion was not measured. Blinding could not be performed due to the nature of the intervention, which has the potential to introduce observer bias. Since it is a single-centre study, the results need to be verified in a multicentre trial for generalisability.
In conclusion, continuous local anaesthetic wound infusion of bupivacaine along with systemic opioid analgesia is feasible in newborn infants; however, the study was underpowered to detect the difference in the amount of systemic opioid use in the first 72 hours post laparotomy. A larger multicentre trial is needed to inform practice.
Data availability statement
Data are available upon reasonable request. If individual level data are required for a meta-analysis, that will be provided on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Sydney Children’s Hospitals Network Human Research Ethics Committee, HREC/16/SCHN/371. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the infants and parents who participated in the study as well as the staff of the neonatal intensive care unit at Grace Centre for Newborn Intensive Care at the Children’s Hospital at Westmead, Sydney.
References
Footnotes
Twitter @himanshu_popat
Contributors HP conceptualised and designed the study, participated in patient recruitment, data analysis, data interpretation, drafted the initial manuscript and responsible for the overall content as the guarantor. RA participated in the study design, patient recruitment and data acquisition. JJ participated in patient recruitment and data acquisition. AW participated in study design, data collection and data analysis. EB participated in study design and data analysis. RH participated in patient recruitment and data acquisition. JdL participated in the study design, patient recruitment and data acquisition. NB participated in patient recruitment and data acquisition. KS provided supervision and participated in the design of the study. GT participated in the study design, patient recruitment and data acquisition. AS participated in study design, patient recruitment and data acquisition. All authors revised it critically for important intellectual content, approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.