Article Text

Abstract
Introduction Direct oral anticoagulants (DOACs) are direct inhibitors of coagulation factor Xa and are frequently used in adults for different indications such as deep vein thrombosis or non-valvular atrial fibrillation. Paediatric patients might benefit as well from DOACs because the simplicity and convenience of their use is likely to decrease physical and psychological stress related to invasive procedures associated with phenprocoumon and heparin therapy. Thus, it is expected that the future use of DOACs will ultimately improve compliance and overall safety of anticoagulant therapies in paediatric populations. To assure safe and effective use the clinical pharmacology and pharmacokinetics (PK) of these drugs need to be evaluated in children.
Methods and analysis This study is a single-centre, open-label, clinical trial in a paediatric population with non-cyanotic congenital heart defects. After having obtained informed consent from the parents, each participant will receive a single oral administration of a drinkable solution of a microdose cocktail of three FXa inhibitors consisting of apixaban (12.5 µg), rivaroxaban (12.5 µg), edoxaban (50 µg), plus a microdose of the two probe drugs midazolam (10 µg) and yohimbine (25 µg). Serial blood samples (n=up to 20) will be collected at specified time points before and up to 25 hours after cocktail administration. The primary PK endpoint will be the area under the plasma concentration time curve of apixaban, rivaroxaban and edoxaban. Secondary PK outcomes will be Cmax, tmax, t1/2, Cl/F and Vss/F. Safety and tolerability of the microdose cocktail will be evaluated as well by a collection of adverse events.
Ethics This study has been approved by the responsible Ethics Committee of the Medical Faculty of Heidelberg University.
Dissemination Study results will be presented at international scientific meetings and published in peer-reviewed journals.
Trial registration number EudraCT 2019-001759-38 16, DRKS00021455.
- Cardiology
- Pharmacology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Current anticoagulation regimens in children with congenital heart defects consist of phenprocoumon, (low molecular weight) heparin or antiplatelet agents. Disadvantages of these regimens comprise invasive monitoring (phenprocoumon) or invasive administration techniques (heparin).
Direct oral anticoagulants (DOACs) are a relatively new class of anticoagulants which have been approved and are widely used in adults.
There are no data available regarding the pharmacokinetics of DOACs in paediatric heart patients.
The expression of drug-metabolising enzymes involved in the eliminations of DOACs varies during human development and growth, but might be influenced by genetic polymorphisms of drug-metabolising enzymes as well.
WHAT THIS STUDY HOPES TO ADD
Evaluation of the pharmacokinetics of three DOACs: rivaroxaban, edoxaban, apixaban simultaneously in children with congenital heart defects aged 6 months to 6 years using a microdose-cocktail approach.
Evaluation of CYP3A and CYP2D6 metaboliser status using the microdosed probe drugs midazolam and yohimbine in paediatric heart patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The pharmacokinetics of rivaroxaban, edoxaban and apixaban will be evaluated regarding their interindividual variability and their potential for drug–drug interactions.
The DOAC with the most favourable profile will be selected and a subsequent study using therapeutic doses will be conducted.
The overall goal of this study is to pave the way for better paediatric anticoagulation.
Introduction
Congenital heart defects (CHDs) are the most common major congenital anomalies. CHDs are defined as a structural abnormality of the heart and/or great vessels that is present at birth. Reported birth prevalence of CHD varies between 8 and 12 per 1000 live births.1 2 The prevalence of complex CHD is reported to be 0.8–2.2 per 1000 live births depending on the demographics of the study population, the inclusion criteria and the study era. Severe CHDs account for most of the morbidity and mortality attributable to CHD.3
A recent German analysis which focused on patients with CHD born between 1996 and 2015 showed that the number of patients with severe CHD had increased significantly since 2008/2009. About 9.4% of patients in this cohort had complex CHD classified as univentricular heart.4 Certain patients with severe CHDs require temporary or lifelong anticoagulation. This applies especially to patients after biological (temporary anticoagulation) or mechanical (lifelong anticoagulation) heart valve replacement or patients after Glenn or Fontan palliation, when the blood flows passively through the pulmonary circulation at low velocity.
The currently used anticoagulants in children are either oral phenprocoumon or warfarin, heparin continuous infusion and subcutaneously injected low-molecular-weight heparins, the latter often limited to short-term therapy.
Since 2008, direct oral anticoagulants (DOAC) including the drugs dabigatran, rivaroxaban, apixaban and edoxaban have been approved for adults in Europe and the USA, and efficacy, safety and pharmacokinetic (PK) data have been obtained in adults.
An oral microdose DOAC cocktail (µ-FXaI) containing apixaban (25 µg), edoxaban (50 µg) and rivaroxaban (25 µg) has been successfully used in adults to study drug–drug interactions.5 6 Comparing the PK of these 3 µ-FXaI, obtained after simultaneous administration, with the PK after therapeutic DOAC doses from the literature showed DOAC clearances always in the same range (dose-proportional PK).7–9 In addition, an already published drug–drug interaction study using ketoconazole in18 healthy adults (>18 years) and µ-FXaI revealed quantitative comparable effects on the clearances of µ-FXaI and therapeutic DOAC doses.5
These drugs so far have not yet been adequately studied in children and are currently not approved for the use in children with CHDs. For children and adolescents, there are ongoing studies on rivaroxaban and apixaban, but most of them are not yet completed or published10 11 (see online supplemental file 1).
Supplemental material
Only few studies focusing on DOACs in children have been carried out so far, or are still ongoing.10 12 Currently, there are only limited data published for edoxaban or apixaban in children.13 The few results from studies of rivaroxaban PK report a favourable safety profile and PK comparable to those already known for adults.12
There are body weight-adjusted treatment recommendations available for rivaroxaban in children with venous thromboembolism. Children with a body weight of 10 kg or more should be treated with a daily dose of 9 mg or higher, depending on the actual body weight.14 A safety assessment of 92 children aged <6 months to 17 years with weight-adjusted rivaroxaban after previous therapeutic treatment with common medication such as low-molecular-weight heparin because of venous thromboembolism was performed. No major bleeding was observed during the clinical trial in 92 children aged <6 months to 17 years.
Therefore, it is important to generate PK data of DOAC in children of young age with CHDs without an increased risk of bleeding, which would be harmful to this vulnerable group. The simultaneous PK assessment of three molecules within the same study is an elegant, modern, ethically adequate design, allowing to limit discomfort to both participants and their families.
In order to obtain data of CYP3A and CYP2D6 activity in young children, microdosed co-administration of the CYP3A substrate midazolam (MDZ; 10 µg) and the CYP2D6 substrate yohimbine (YOH; 25 µg) as probe drugs along with the µ-FXaI will be carried out. These both drugs were proven to function as microdosed probe drugs for phenotyping these enzymes by showing dose linearity.15 16 Pharmacogenomics of further enzymes, transporters, etc could influence the PK of the respective drugs as well, however including more substrates into this first microdose approach in children seems not feasible yet. Thus, the microdose cocktail to be used in the study contains a total of 5 different drugs which will be administered simultaneously by oral route.
Methods and analysis
Study design
This is an open-label, single-centre, single-dose clinical trial in a paediatric population with non-cyanotic CHDs at the Department of Paediatric and Congenital Cardiology of the Heidelberg University Hospital in cooperation with the paediatric Clinical Pharmacological Trial Centre (paedKliPS). This protocol was designed following the Standard Protocol Items: Recommendations for Interventional Trials guidelines.17
Study population
Infants and children aged 6 months up to 6 years with a body weight >7 kg who are admitted to the paediatric cardiology wards for the surgical correction of a non-cyanotic CHD will be eligible for study inclusion. Children who are treated with anticoagulants, who have a coagulopathy or lesions or conditions which are associated with a significant risk for major bleeding are excluded, as well as children who have kidney or liver insufficiency, or are treated with drugs known to be relevant inducers or inhibitors of drug-metabolising enzymes. Detailed inclusion and exclusion criteria are listed in table 1.
Detailed inclusion and exclusion criteria of DOAC-Child
For the purpose of surgery, all patients are under routine continuous cardiorespiratory monitoring (Intellivue, Philips Healthcare, Eindhoven, The Netherlands) and have central vascular access. Depending on the age and the clinical condition, most patients have a feeding tube as well.
Primary objective
Assessment of the PK of rivaroxaban, apixaban and edoxaban, when co-administered as a microdose cocktail (apixaban 12.5 µg, rivaroxaban 12.5 µg, edoxaban 50 µg) in children with CHDs, aged 6 months to 6 years.
Secondary objectives
To compare the PK of the FXaI in children with those reported in healthy adults and patients from literature.
To characterise the CYP3A activity by means of a MDZ microdose in children.
To characterise the CYP2D6 activity by means of a YOH microdose in children.
To evaluate tolerability (and safety regarding laboratory parameters) of this microdose cocktail in children.
Study outcome
Primary outcome is the area under the concentration-time curve (AUC0-∝) of the three DOACs apixaban, edoxaban and rivaroxaban. Secondary outcomes include standard PK parameters (Cmax, tmax, t1/2, Cl/F and Vss/F) of each FXaI and YOH, as well as the metabolic clearance of MDZ by means of AUC2–4h.18
Recruitment
Recruitment takes place at the Department of Paediatric and Congenital Cardiology. Prior to the surgical intervention, parents of potential participants will be addressed by a study physician regarding the study which serves as short information about the clinical trial. After the surgery detailed information will be given and discussed with both parents. After full explanation of the purpose, the procedures involved, the expected duration, the potential risks and benefits and any discomfort related to the clinical trial both parents will be asked whether they agree to participate and, in that case, to sign the informed consent form before any study procedures are carried out.
Screening
The screening visit is defined as accurate check of all diagnostic findings which were made in course of the preoperative assessment to evaluate eligibility. This is done after the surgery by a trial team physician in order to check inclusion and exclusion criteria.
Interventions
The intervention begins as early as on postoperative day 3 (about 72 hours after surgery) with the oral administration of the study drugs. They are dissolved in 110 mL drinking water to ensure comfortable oral application. If the patient has a feeding tube, this will be used for administration and will afterwards be flushed with 5 mL drinking water. All patients have as a clinical routine measure due to cardiac surgery a central venous line in place. Vital parameters and other clinical or laboratory assessments which are necessary to ensure patients' safety are extracted from the daily documentation during clinical routine.
Sample collection
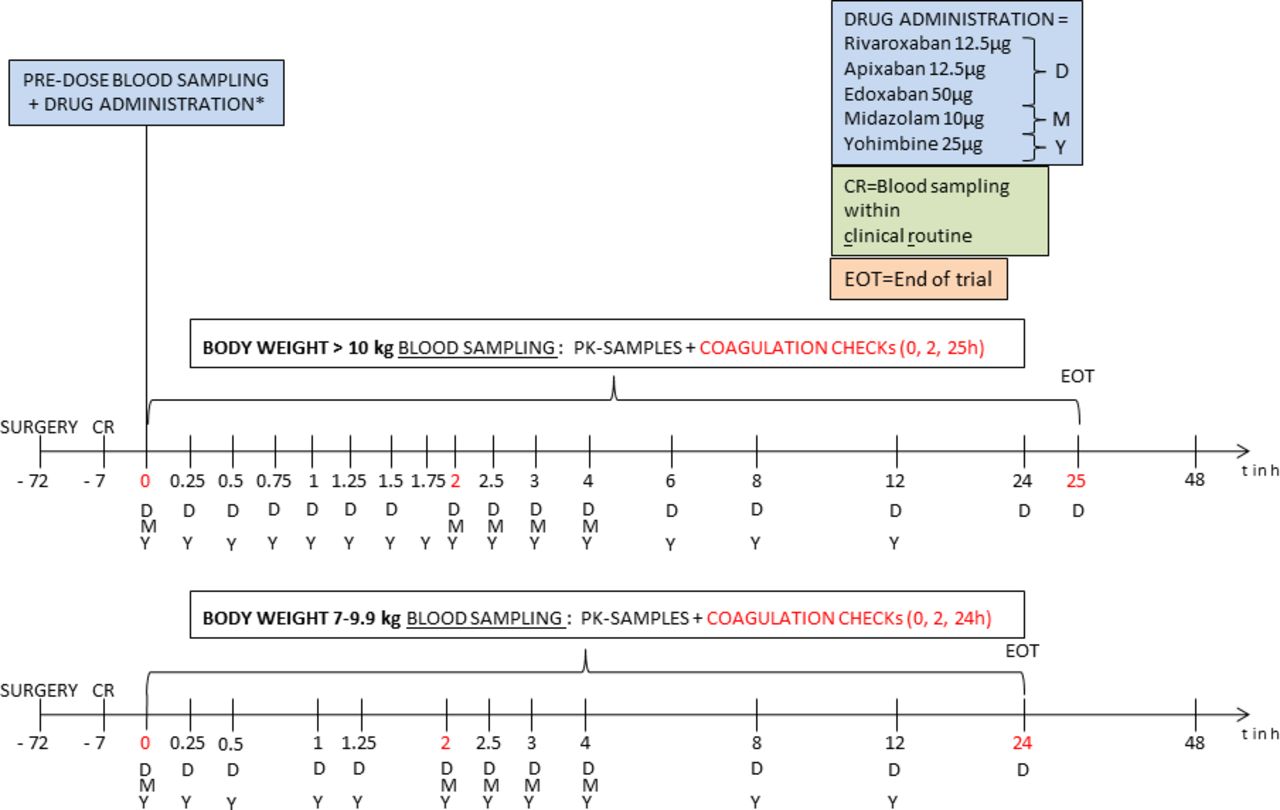
PK blood samples will be collected via a central venous line and time points are dependent on body weight (figure 1). The total amount of blood drawn will be 25 mL over 25 hours for children with a body weight of at least 10 kg. This includes 17 samples to evaluate PK parameters (S-Monovette® 1.2 mL lithium heparin collection tubes, Sarstedt, Nümbrecht, Germany) and three safety checks by which the coagulation parameters will be observed (S-Monovette® 1.4 mL citrate collection tubes, Sarstedt, Nümbrecht, Germany). Blood samples for the DOAC PK-analysis (Li-Hep) will be obtained before and 0.25, 0.5, 0.75, 1, 1.25, 1.5, 2, 2.5, 3, 4, 6, 8, 12, 24 and 25 hours after intake of the oral solution. This is equivalent to a loss of blood volume of 3.28% of a child weighing 10 kg. For children weighing 7–9.9 kg a reduced sampling scheme (12 PK samples and three coagulation samples, specific timepoints are before and 0.25, 0.5, 1, 1.25, 2, 2.5, 3, 4, 8, 12 and 24 hours after intake of the oral solution.) will be performed to limit the blood loss (18.6 mL in 24 hours equivalent to 3.54% for a child weighing 7 kg).19 All PK samples will be quantified by ultraperformance liquid chromatography-tandem mass spectrometry methods in the Clinical Analytical Laboratory of the Department of Clinical Pharmacology and Pharmacoepidemiology at the University Hospital Heidelberg.

{kind=link}
Study design assessing the pharmacokinetics of rivaroxaban, apixaban, edoxaban as well as the CYP3A and CYP2D6 enzyme activity in children with congenital heart defects. Upper timeline: Sampling schedule for children weighing 10 kg and more, lower timeline: sampling schedule for children weighing 7–9.9 kg. CR, clinical routine; EOT, end of trial.
MDZ will be measured in 5 samples (before and 2, 2.5, 3 and 4 hours after administration) using an established limited sampling strategy18 and YOH20 in the samples taken up to 12 hours after administration.
Three coagulation checks (quick, international normalised ratio (INR), activated partial thromboplastin time (aPTT)) are obtained before, 2 and 24/25 hours after drug administration.
End of trial
After the last blood sample, the end of trial visit includes reviewing the last clinical examination and laboratory assessment, which both are performed at least once during 24 hours by clinical routine.
Concomitant medication
Any necessary medication (judged by a responsible physician) for the best clinical care and/or emergency treatment is permitted. Concomitant medication will be documented (date, time, dose, route of administration) by a member of the trial team. For safety reasons simultaneous administration of anticoagulants, thrombolytics, platelet inhibitors such as GPIIb/IIIa-inhibitors and P2Y12 inhibitors, and thienopyridine (clopidogrel) are prohibited for the duration of the trial.
Sample size calculation
Since no PK data in young children are available for the microdosed FXaI cocktail, no formal sample size calculation could be performed. It is planned to enrol up to 20 children with CHDs. This number of patients is consistent with sample sizes of similar exploratory PK studies, which is expected to provide sufficient information on PK, safety regarding laboratory parameters and tolerability of the µ-FXaI cocktail and the suitability of this methodology in future clinical paediatric drug development. In addition, it is expected that robust single-dose PK data of 3 FXaI in a young paediatric population will be generated to provide the first guidance for dose adjustment in clinical use.
Data management
Clinical routine data are also documented for this clinical trial. Vital signs (ie, blood pressure, heart rate) are documented at screening, prior to the drug administration, at any specific PK timepoint, and at end of trial. Concomitant medication and adverse events (AEs) are also recorded. Printed source data sheets are used for the primary data collection and documentation. All source data information are timely transferred to the clinical trial management database (Promasys, OmniComm Systems, Fort Lauderdale, USA).
Data analysis and missing data
Standard PK parameters (Cmax, tmax, AUC0-∝, t1/2, Cl/F, and Vss/F) of each FXaI and YOH will be calculated by non-compartmental analyses (Monolix 2021R2, Lixoft SAS, Antony, France) and its results will be presented by descriptive statistics (GraphPad Prism V.8.0.0 for Windows, GraphPad Software, San Diego, California, USA). CYP3A activity will be quantified using the estimated metabolic clearance of MDZ by means of AUC2–4h.
Individual missing or inconsistent data will be subject to a simple edit query process. Eventually missing data will not be imputed.
Patient and public involvement
Patients and/ or the public were not involved in any stages of this clinical trial: study design/ conduction/ analysis.
Ethics and dissemination
Ethics approval
The study protocol (V.4.0), patient information and informed consent form were approved by the ethics committee of the Medical Faculty of Heidelberg University (AFmo-606/2019) and the German competent authority (BfArM).
To enable the participation for children younger than 2 years and with a weight lower than 10 kg a protocol amendment was submitted and approved (Protocol V.5.1). For these patients, a reduced sampling scheme was introduced to keep the relative loss of blood volume below 5% in 24 hours.19
Study monitoring
A trained clinical trial monitor is assigned from the Department of Clinical Pharmacology and Pharmacoepidemiology at the University Hospital Heidelberg to perform the monitoring of this clinical trial.
Safety considerations
All medications will be administered as a subtherapeutic microdose. Although it is unlikely that the achieved concentrations of the administered trial medications confer any pharmacological effect or adverse drug reaction, a maximum degree of safety is essential in this vulnerable population. Clinical monitoring as per standard of care after cardiac surgery will be used.
Benefit and risk assessment
There is no direct benefit to the patients or their parents. Because of the clinical setting in which the study will be carried out, no additional invasive procedures have to be performed. All participants are admitted as inpatient to the paediatric cardiac wards, where continuous cardiorespiratory monitoring and central vascular access, etc are already provided.
In order to reduce additional burden of study procedures to the patient in the postoperative phase, after having signed informed consent, the patients’ medical history, findings during the clinical examination and other parameters routinely assessed and documented during the treatment for these patients will also be completely recorded for this clinical trial. Due to the sensitive drug assay, the amount of blood taken for the PK analyses is minimised.
All study drugs will be given as single microdoses only which do not elicit any pharmacological effects or AEs.5 The combination of microdoses of apixaban, rivaroxaban, edoxaban has been used in adults and at FXaI peak concentrations, INR increased just by 3.9% and aPTT by 3.1%, which was clinically not relevant.5 No bleeding complications occurred. Clinically relevant non-major bleeding (menorrhagia and gingival bleeding) has been observed in four children with venous thromboembolism taking therapeutic rivaroxaban within the Einstein-Jr phase III study.21
Due to very sensitive analytical assay for apixaban and rivaroxaban, the dose of apixaban and rivaroxaban is halved to 12.5 µg each compared with the adult study. Microdosed MDZ and YOH were used frequently in adults and no relevant AEs were observed at all.
Thus, the risk for AEs or toxicity is minimal. We do not expect any bleeding complications by µ-FXaI. If bleeding complications occur the effects of rivaroxaban and apixaban can be reversed by andexanet alfa. It also inhibits the function of all heparins.22 We have summarised the case reports describing children exposed to rivaroxaban or edoxaban,23 intentionally or unintentionally, in table 2.
Case reports about children who were exposed to direct oral anticoagulants (DOAC)
In summary, potential risks of participation in this clinical trial are small and predictable. The trial drugs are administered at subtherapeutic microdoses on one occasion, so that no type A adverse drug reactions are expected. The participant’s suitability will be carefully evaluated, and their health will be closely monitored during the trial.
Publications and data access
The results of this investigation will be published in an international scientific peer-reviewed journal. It is not planned to make the data publicly available.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of the Medical Faculty of Heidelberg University Reference Number of the ethics approval: AFmo-606/2019. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @VZieseHD
Contributors SAH: writing of trial protocol and manuscript, subinvestigator, conduct of the trial. GM: conception of the trial, writing of trial protocol, biostatistician. KC-J: conception of the trial, writing of trial protocol, deputy investigator. MG: conception of the trial, writing of trial protocol, principal investigator, conduct of the trial. VZ: conception of the trial, writing of trial protocol, deputy investigator, conduct of the trial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme "Open Access Publikationskosten" as well as by Heidelberg University.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.