Article Text

Abstract
Purpose Oesophageal squamous papilloma (OSP) is a rare epithelial lesion with an unclear aetiology, found incidentally in upper gastrointestinal endoscopy (UGE). We evaluate the epidemiology, general features and endoscopic and histological characteristics of OSP in children in a single centre.
Methods We conducted a retrospective search of 3568 medical records of children under 18 years old who underwent UGE between 2004 and 2022, at Hospital Metropolitano de Quito, Ecuador. We described the general features of 15 patients diagnosed with OSP. Histopathology reports were analysed, including a chromogenic in situ hybridisation (CISH) for human papillomavirus (HPV) 6/11.
Results OSP was diagnosed in 15 patients between 10 and 16 years of age, with an estimated prevalence of 0.4%. The gender ratio male to female was 1:1.1. Most patients (n=14) underwent UGE due to abdominal pain. Lesions were found predominantly in the upper and lower part of the oesophagus; 12 patients had isolated lesions, and none of the lesions tested positive for HPV on CISH 6/11 analysis. Additionally, Helicobacter pylori and eosinophilic oesophagitis (EoE) were diagnosed in one patient each.
Conclusion Our study describes the clinical features of paediatric OSP in a single centre. The prevalence was similar to that in the adult population but higher than in other paediatric populations, and none of our patients had HPV.
- Gastroenterology
- Epidemiology
- Adolescent Health
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Oesophageal squamous papilloma (OSP) is an infrequent epithelial lesion with few reports in paediatric population. There is not a clear consensus for its treatment.
WHAT THIS STUDY ADDS
In this single centre, the prevalence in children was similar to adults. More cases of OSP were diagnosed in the last few years. There was no association with human papillomavirus (HPV).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In children with OSP, the HPV screening might not be mandatory.
Introduction
Oesophageal squamous papilloma (OSP) is a rare, asymptomatic, benign tumour mostly found incidentally in upper gastrointestinal endoscopy (UGE). It is mainly a solitary lesion, predominantly located in the middle and lower oesophagus. It is more commonly presented in middle-aged patients, and the male–female ratio is variable.1
The aetiology is still unclear; however, some mechanisms have been proposed, such as chemical, mechanical and infectious causes.1 Human papillomavirus (HPV) positivity varies from 0% to 87.5% in adults with OSP.2 The diagnosis is made by histological confirmation, and no more management is needed other than endoscopic removal. In some cases, malignancy has been associated with OSP, especially in adults.3
The prevalence of OSP ranges from 0.01% to 0.45%,4 and few reports have been made on the paediatric population. There are no studies that evaluate the epidemiological characteristics of OSP and its association with HPV in our population. Therefore, this report aims to determine the epidemiologic, general features, endoscopic and histologic characteristics of OSP in paediatric patients in a single centre in Quito, Ecuador.
Materials and methods
We conducted a retrospective study from 2004 to 2022 of patients under 18 years old evaluated by the pediatric gastroenterology department in Hospital Metropolitano in Quito, Ecuador. All the medical records from patients who underwent a UGE, between January 2004 and June 2022, were reviewed. During this period, a total of 3568 upper endoscopies were performed.
Fifteen children (boys and girls) from 10 to 16 years of age with OSP were included in this study. Clinical manifestations, endoscopic and histological findings were analysed in every patient.
Patient involvement
Patients were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
Epidemiology
Of 3568 children who underwent a UGE, 15 were diagnosed with OSP. The prevalence of OSP in children during 19 years was 0.4%. Most of the cases were diagnosed in 2022 (n=4; 26.6%) (figure 1).
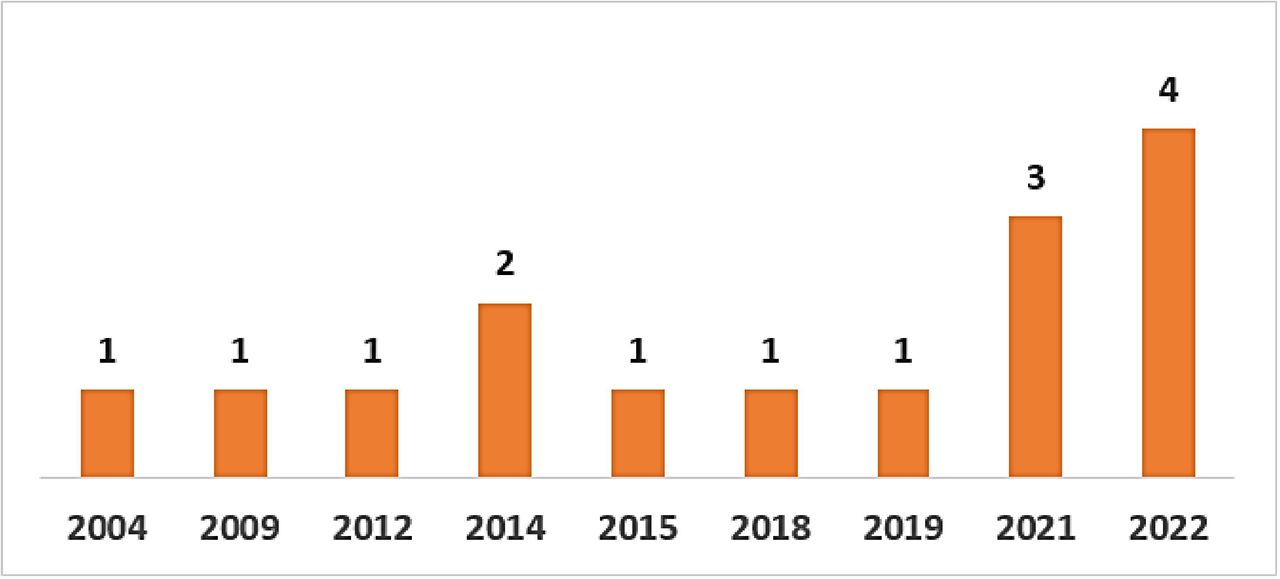
Number of cases of OSP in children per year, in a single centre in Ecuador.
General features
The mean age at diagnosis of OSP was 13.8 years±1.65. The gender ratio of males to females was 1:1.1, with eight boys and seven girls.
The indications for UGE were abdominal pain (n=14), nausea (n=2); additionally, reflux, vomiting and rumination presented in one patient each.
Endoscopic and histopathological findings of the oesophagus in OSP
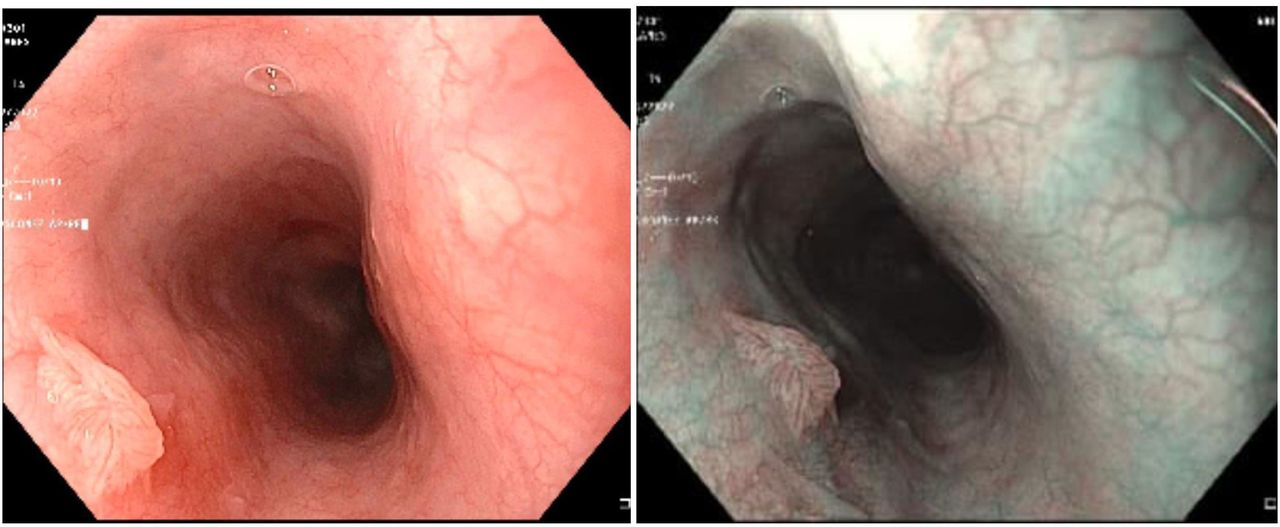
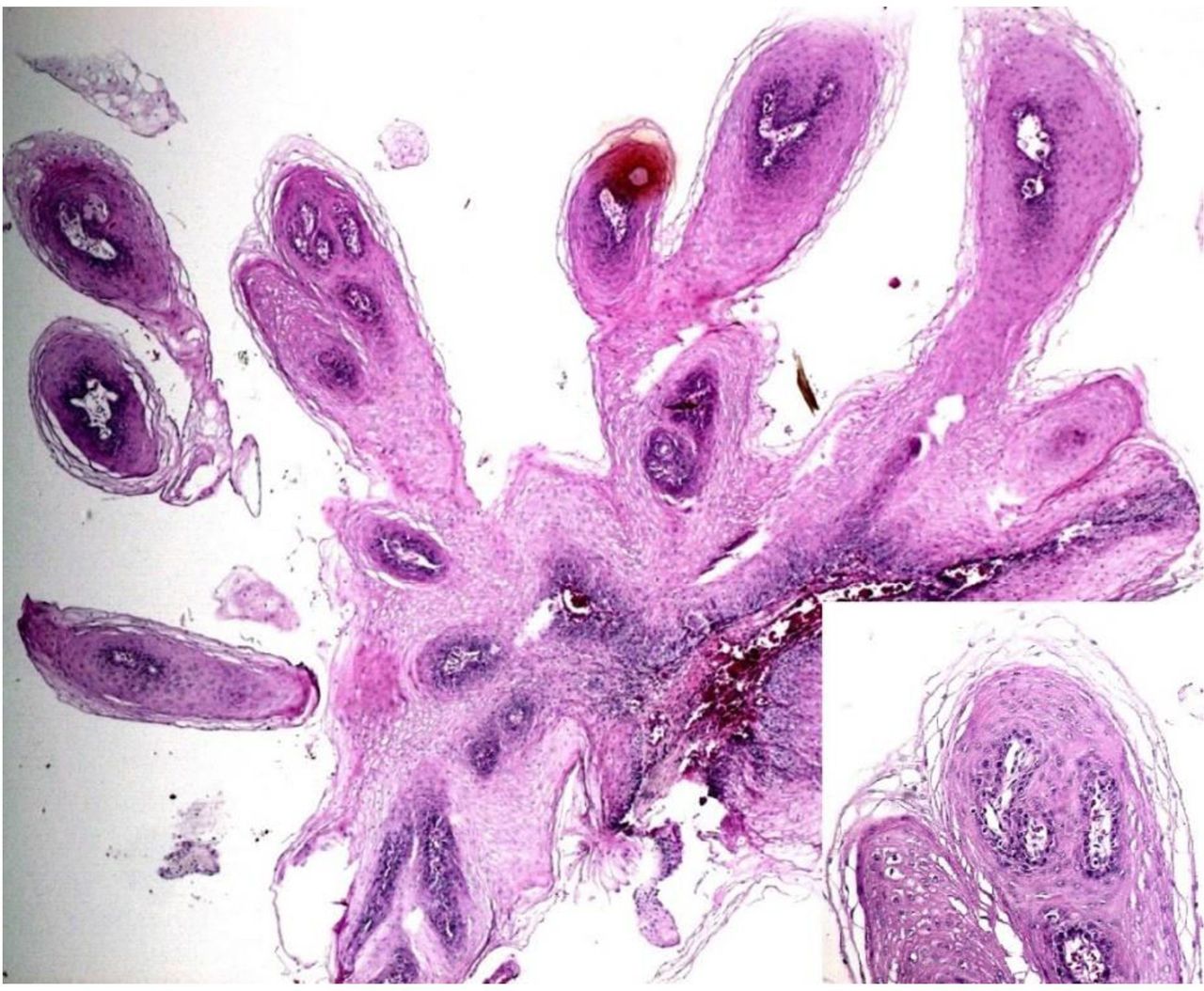
We found 15 children with macroscopic findings suggesting OSP (figure 2). The oesophageal mucosa lesions were formalin-fixed paraffin embedded and cut at 4 µm, and then stained with H&E (figure 3). Histological diagnosis of OSP was confirmed. The HPV 6/11 study was conducted using the chromogenic in situ hybridisation (CISH) technique by Zytovision (Bremerhaven/Germany).

Oesophageal squamous papilloma on upper endoscopy.

{kind=link}
{kind=link}
{kind=link}
Squamous papilloma at low magnification. An exophytic tumour with papillary proliferation of non-dysplasticsquamous epithelium (Insert H&E 20×).
The lesions were predominantly found in the upper (n=6) and lower (n=6) parts of the oesophagus; four lesions were detected in the middle oesophagus. Twelve patients had isolated lesions, and only three had multiple lesions; the mean size of the lesions was 2.46±0.98 (varied from 1 to 4 mm). None of the lesions tested were positive for HPV on CISH 6/11 analysis.
All the children were screened for Helicobacter pylori, and those with macroscopic findings were tested for eosinophilic oesophagitis (EoE) with oesophageal biopsies. As a result, one patient was simultaneously diagnosed with EoE (OSP lesion in the lower oesophagus), and one patient had H. pylori (OSP lesion in the upper oesophagus).
Treatment
All the OSP lesions were treated by endoscopic removal. No follow-up UGE was performed.
Discussion
Squamous papilloma is a benign oesophageal epithelial polyp composed of squamous epithelium with a papillary growth pattern, and it is commonly diagnosed incidentally by UGE. It was first histologically verified in 1959 by Adler et al as a solitary lesion with a predominant location in the middle and distal oesophagus.5 Our study found lesions mainly in the upper and lower oesophagus. The lesions are usually small, from 2 to 6 mm1; in this study, the size of the lesions varied from 1 to 4 mm.
OSP is most commonly diagnosed in patients between 43 and 50 years, and the male–female ratio is variable.1 In our study, all the patients were under 18 years old, and there was no difference between genders (males to females ratio was 1:1.1).
Its aetiology is still undetermined; however, it has been proposed that chronic inflammatory reactions related to a chemical or mechanical irritant (gastro-oesophageal reflux, smoking, alcohol, direct trauma, food impaction, caustic injury) and HPV and/or EBV infections may be responsible for these lesions.1 6 7
OSP may be subdivided histologically into three types: exophytic, endophytic and spiked types. The exophytic type is the most common. Histologically, squamous papillomas consist of a papillary proliferation of non-dysplastic squamous epithelium with fibrovascular cores of lamina propia and koilocytes can be seen; progression to dysplasia or carcinoma is extremely rare.8 Infection with HPV has been found in apparently normal oesophageal mucosa, squamous papillomas and squamous cell carcinomas of the oesophagus. It has been suggested that HPV has a role in the pathogenesis of squamous cell carcinoma of the oesophagus. In situ hybridisation has demonstrated that 23% of all oesophageal cancer cases contain HPV DNA, particularly types 16 and 18. HPV DNA has also been found in 15% of non-malignant oesophageal biopsies. In addition, several reports have indicated that HPV DNA is often not detectable in OSP.9–11 None of the 15 oesophageal lesions obtained in this study showed evidence of low-risk HPV via CISH analysis or viral cytopathic effect on histopathology; all were HPV 6/11 negative. Our results were similar to other recent studies, which also found no association between HPV and OSP.1 4 12
ESP is most frequently found in adults, with a prevalence of 0.01%–0.45%.3 5 13 Tou and Al-Nimr reported in a 15-year case series a prevalence of OSP of 0.08% among children.4 In contrast, in this report, we found a prevalence similar to the adult population; 0.4%. In a study conducted over 14 years, Pantham et al described an increased incidence of OSP in adults ranging from 0.13% in 2000 to 0.57% in 2013, related to more cases of HPV infections.14 In our study, we found an increase in the number of cases of OSP, especially in 2022 (figure 1); even though, in the last years, fewer UGEs have been performed in children in Hospital Metropolitano de Quito, probably due to the COVID-19 pandemic. We did not find an association with HPVfigure 1
Some cases of OSP in children have reported the presence of H. pylori in the gastric mucosa15 and the simultaneous diagnosis of EoE16; similarly, in this case series, we found one patient of each.
There is no specific management for OSP; currently, the recommended treatment is endoscopic removal.17 18 OSP is a benign lesion, and there have been no malignancies associated with OSP found in the paediatric population; therefore, surveillance is considered unnecessary in children.4 In our study, OSP lesions were removed using excisional biopsies, and no follow-up was performed. In contrast, an endoscopic follow-up in adults is encouraged by some authors, who have found an association with cancer.3 19
Conclusion
The prevalence in our centre was similar to the adult population, but higher than in other paediatric populations; none of our patients had HPV. Multicentre studies are needed to confirm the epidemiology of OSP among children and the cause of its increasing incidence.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed to conduct this study. This was a descriptive study and compromised non-experimental research with secondary data and anonymised patients; authorizedauthorised by Hospital Metropolitano de Quito.
References
Footnotes
Twitter @NMontalvoF
Contributors Planning: FVM. Drafting of the article: PH, AVM and LRA. Collecting and analysis of the data: PH and NM. Interpretation of the data and edition: EAA and FVM. Guarantor: PH
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.