Article Text

Abstract
Background Mechanisms and patterns of injury in children are changing, with violent mechanisms becoming more prevalent over time. Government funding of services for children and young people has reduced nationally over the last decade. We aimed to investigate the trends in admissions of injured children to a Major Trauma Centre (MTC) and examine the relationship between injuries sustained by violent mechanisms and local authority funding of children and youth services within the same catchment area.
Methods A 10-year observational study included all patients aged<18 years treated at a regional MTC between April 2012 and April 2022. Number of admissions with violent trauma, mechanism of injury, requirement for operative intervention and mortality were compared with published annual local authority expenditure reports.
Results 1126 children were included; 71.3% were boys, with median age 11 years (IQR 3–16). There were 154/1126 (14%) children who were victims of violent trauma; they were more likely to be boys than children injured by non-violent mechanisms (84% vs 69%). The proportion of injuries attributed to violence increased over the study period at the same time as reductions in local authority funding of services for the early years, families and youth services. However, there were insufficient data to formally assess the interdependency between these factors.
Conclusions The proportion of injuries attributed to violence has increased over time, and government spending on specific children and young people’s services has decreased over the same time period. Further work is needed to examine the interdependency between spending and violent injuries in children, and public health interventions to target violence-related injuries should take into account youth service funding.
- adolescent health
- epidemiology
- health services research
- social work
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Violence-related injuries in children appear to be increasing in prevalence. It is reported that trends in reduced government funding of youth services have been associated with increased reports of knife crime, but the relationship between violence-related injuries and children and young people’s services funding requires closer exploration.
WHAT THIS STUDY ADDS
This study demonstrates an increase in the proportion of injured children being admitted to hospital as a result of violence compared with non-violent mechanisms over the last decade. Examination of the relationship between records of such injuries and local authority spending reports identifies possible associations with some of the local authority funding metrics.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
While we are not able to establish causality, the increase in violence-related injuries is a significant public health concern, and the possible role of targeted increases in funding of children and young people’s services in attempting to reverse this trend warrants further investigation.
Introduction
Trauma remains a significant cause of mortality and morbidity in children and young people worldwide, with injury reported as the leading cause of death for children over the age of 1 year.1 2 Mechanisms and injury patterns vary in frequency between countries and age groups,3 with falls, road traffic collisions and interpersonal violence overall representing the most common causes of injuries requiring admission to hospital.4 In recent years, it has been observed that mechanisms and patterns of injury appear to be changing over time. Injuries resulting from interpersonal violence are becoming more prevalent in comparison to non-violent trauma.4 In England, violent injuries are increasing in all age groups, in contrast to a stable or downward trend in the rest of the UK.5
Violent injuries are a major concern at a public health level, affecting health and social outcomes for the individual as well as carrying significant resource implications for health and social care systems,6 policing and the criminal justice systems. Penetrating injuries are a specific subset of violent trauma with particular implications for public safety as well as across systems. While sustained less frequently than other types of violent trauma, penetrating injuries are also being recorded at increasing rates.5 While firearms related mechanisms are rare in the UK in contrast to worldwide data,2 4 knife crime has reached a record high7 and rates continue to increase nationally.
Strategies have been proposed to reduce and prevent knife crime, including multiagency approaches. Testimony from young people directly affected by knife crime emphasises the power of youth services in breaking the cycle and in knife crime reduction and prevention.7 Unfortunately, national data has demonstrated a reduction in government spending on youth services in recent years,8 as well as a strong association between cuts to such services and increased reports of knife crime.6 The current study aims to examine the trends in injuries sustained as a result of all violent mechanisms in children at a large UK Major Trauma Centre (MTC) and the relationship between these injuries and local government youth provisions in the same catchment area.
Methods
Study design and setting
An observational study was undertaken using data available from the prospectively collected Trauma Audit and Research Network (TARN) records for a large MTC in the East Midlands, UK. The East Midlands is a region of 6034 square miles with a population of 4.9 million people, an increase of 7.7% in the last decade (Census 2021). There are two major urban cities (Nottingham and Leicester) and several smaller urban conurbations as well as large areas of rural land across the six counties (Leicestershire, Derbyshire, Lincolnshire, Northamptonshire, Nottinghamshire and Rutland). This centre is a combined adult and children’s trauma centre, and is one of the busiest nationally, caring for approximately 2000 TARN eligible patients each year. The study included all paediatric patients who were seen by the major trauma team between April 2012 and April 2022 following a trauma activation.
Data collection
Data were collected in May 2022 from Performance Review Indicators reports for the East Midlands MTC, produced by TARN. This data includes all submissions made to the centre up to April 2022, for patients who arrived at the centre between April 2012 and April 2022 and who met the research network eligibility criteria. Patients were identified from the database as being injured due to violence according to mechanism coding such as ‘blow(s) with weapon’, ‘blow(s) without weapon’, ‘stabbing’ or ‘shooting’. These data were then cross-referenced with a local prospectively collected database held by the major trauma department at the MTC to identify patients who had been readmitted to the major trauma department since 2016. Readmission data was not available for admissions prior to 2016.
Social funding data
Data regarding social funding were recorded using publicly available records from the UK government for the East Midlands, and included the following specific domains (taken verbatim from the public records, and terms have not been changed or interpreted): local authority expenditure on children and young people services; Sure Start children’s centres and early years; family support services; services for young people; youth justice; and other children’s and families’ services; safeguarding children and young people services, and children looked after. Funding values were taken directly from the public records, and adjusted to values for 2021 using the Bank of England’s inflation calculator.9 The funding was calculated per population according to the same public records.
Data analysis
All data are summarised using median and IQR for continuous data and number and percentage in parentheses for categorical data. Simple pairwise comparisons were undertaken using Mann-Whitney U tests for continuous data and χ2 analysis for categorical data. For modelling the association between the (a) proportion of injuries attributed to violence and time and (b) the proportion of funding per population and time (for each of the individual funding domains), beta regression was used to model time as a non-linear function to allow a flexible shape for the association between time and each measurement. For modelling the association between pounds spent per person for each of the funding services and the proportion of injuries attributed to violence, each variable was modelled as a time series. The interdependency between pairs of time series was explored using a transfer function model. If no suitable model could be identified, the stationarity of each time series was assessed using an augmented Dickey-Fuller test. Non-stationary time series were differenced to remove any underlying time trend and create stationary time series. Cross-correlations of pairs of stationary time series were calculated. In a secondary analysis, the time series are not adjusted for potential time trends. In all such analyses, Pearson correlations between the two time series are calculated at a lag of 0. The estimated correlations, associated 95% CIs and p values are reported. A p value of <0.05 was considered statistically significant. Analyses were performed using GraphPad Prism V.9.410 and R (R Foundation for Statistical Computing, Vienna, Austria) using the packages: betareg, forecast, GGallay, ggeffects, ggplot2, rms, scales, tfarima and viridis.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this study.
Results
Patient characteristics
There were 1126 patients, with a median age of 11 (IQR 3–16) years, and 804/1126 (71%) were boys. There were 154/1126 (14%) injuries caused by violence. Table 1 summarises the patient characteristics for all injured children, with comparison between violent and non-violent injuries. Table 2 summarises the total adjusted spending for each service throughout the study period, as well as the numbers of injuries attributed to violence.
Study patient characteristics with comparison between those with violent and non-violent injuries
Adjusted funding for each service and number of violent injuries during the study period
Injuries caused by violence
When compared with the children with injuries not attributed to violence, those with violent injuries were more likely to be boys, and their pattern of injury was different; they were more likely to have injuries to the torso (thorax and abdomen) but less likely to have spine or limb injuries and their mechanism of injury was significantly more likely to be penetrating (table 1). In addition, children with injuries attributed to violence had a significantly lower length of stay but higher risk of readmission than non-violently injured children (table 1).
Trends over time
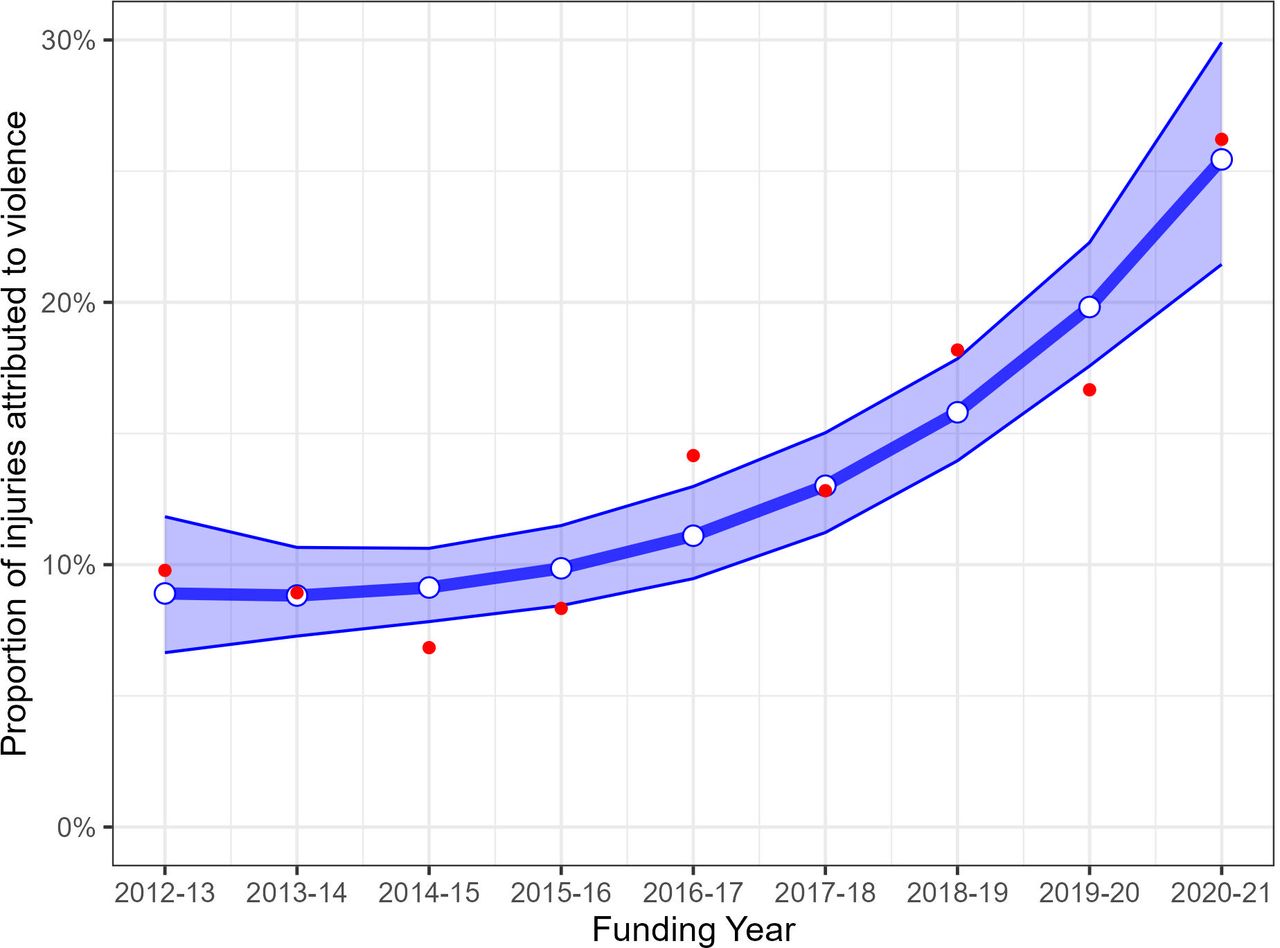
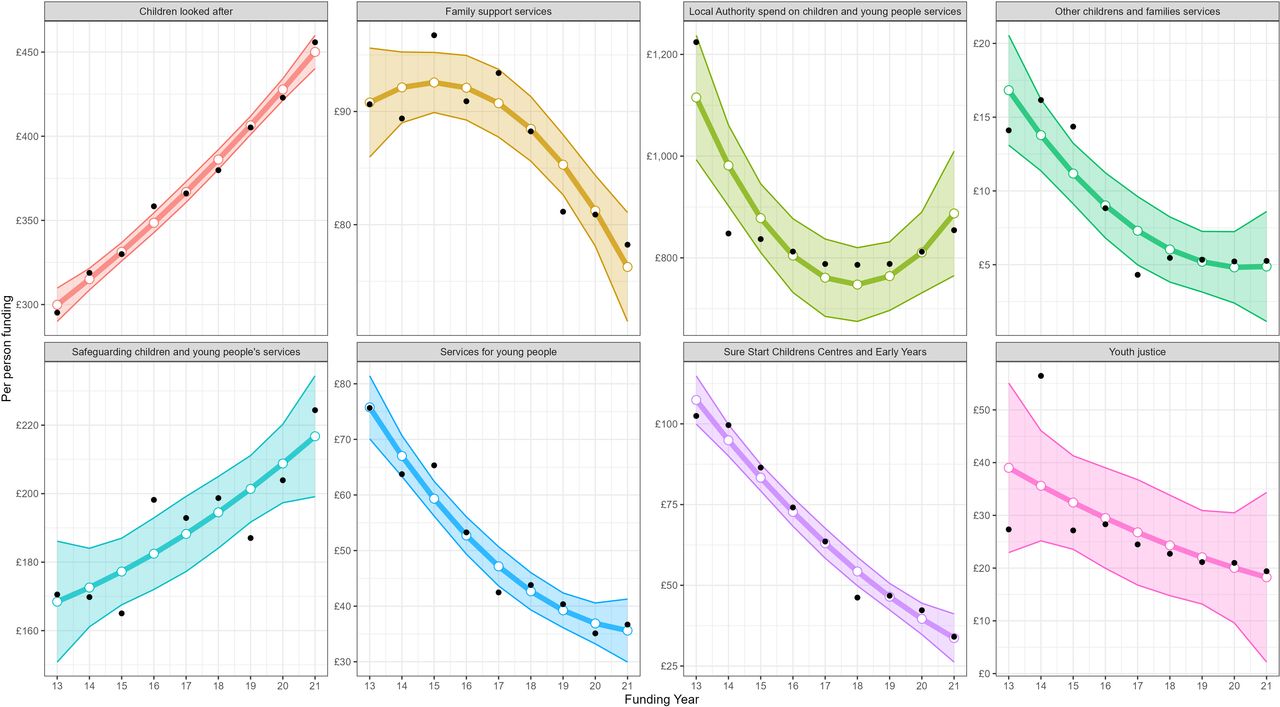
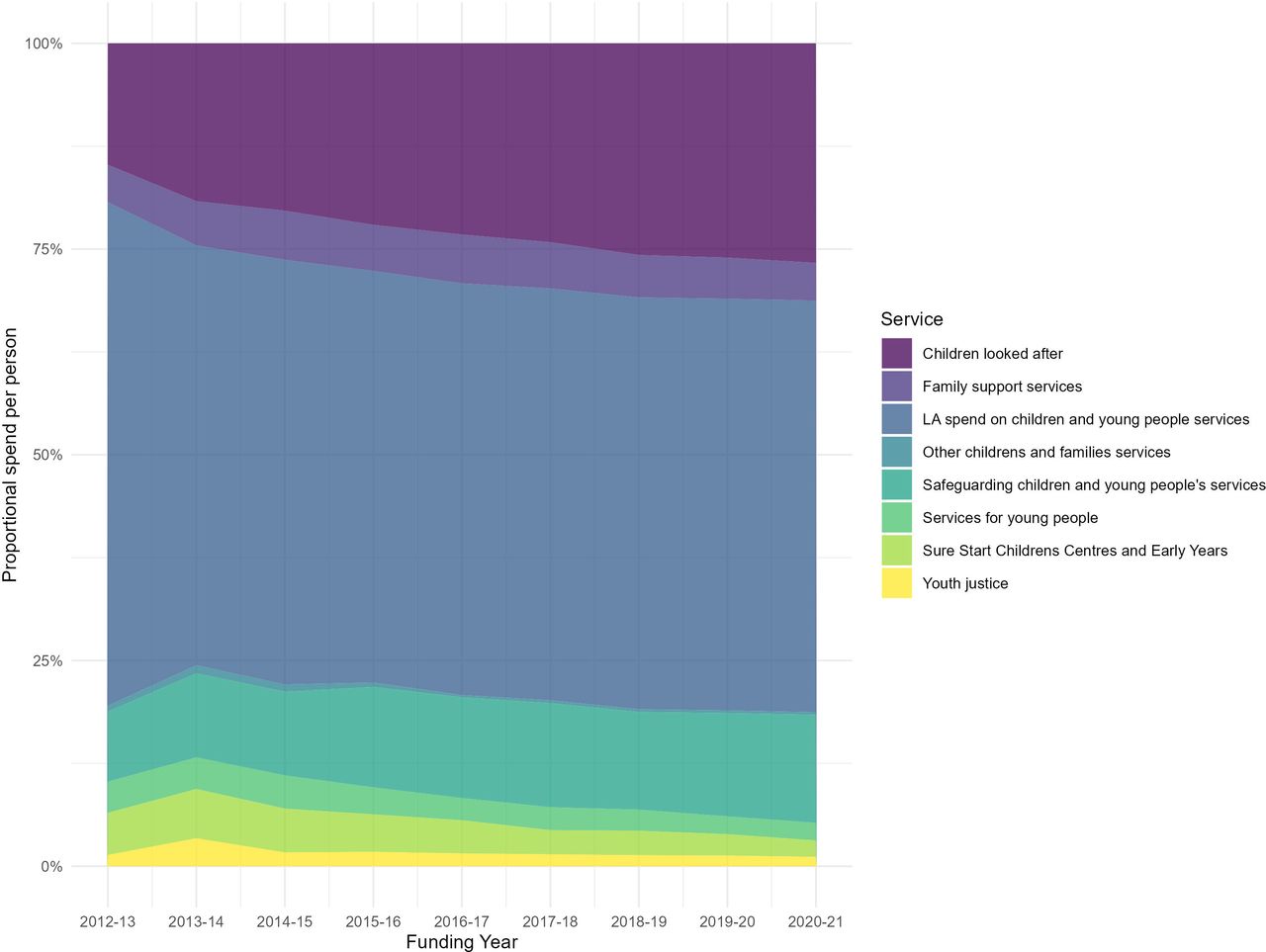
The proportion of injuries attributed to violence significantly increased over the study period (p<0.001) (figure 1). Over the same period there were also significant decreases in funding for Sure Start children’s centres and early years, family support services, services for young people, youth justice and other children’s and families’ services (all p<0.05) (figure 2). There did not appear to be a significant trend in local authority expenditure on children and young people services, and there was a positive trend over time for or safeguarding children and young people services and children looked after (figure 2). Figure 3 illustrates the proportion of funding for each individual service over time during the study period.

The proportion of injuries attributed to violence over the study period using beta regression modelling

Pounds spent per young person for each individual funding domain over the study period using beta regression modelling

{kind=link}
{kind=link}
{kind=link}
Proportion of overall spending for each individual service over the study period.
Associations between violent injuries and social funding
The interdependency between pairs of time series was explored using a transfer function model. If no suitable model could be identified, the stationarity of each time series was assessed using an augmented Dickey-Fuller test. Non-stationary time series were differenced to remove any underlying time trend and create stationary time series. Cross-correlations of pairs of stationary time series were calculated. The relationship between the proportion of injuries attributed to violence and the adjusted social funding per population in the same catchment area was initially explored using transfer function models, but due to the limited amount of data, no such model converged. Each individual time series was assessed for stationarity, with all series returning p values>0.70 expect for the proportion of injuries attributed to violence and safeguarding children and young people services (p=0.08 and p=0.09, respectively), indicating non-stationarity in each time series. After differencing, the best-fitting autoregressive integrated moving average (ARIMA) model for all time series was a (0,0,0) model. Based on the analyses of these stationary time series, there were no statistically significant associations between violent injuries and funding per population (table 3a).
Associations between adjusted funding per population for individual funding domains and proportion of injuries attributed to violence using stationary and non-stationary models
When non-stationary time series were used to examine the relationship between the proportion of injuries attributed to violence and the adjusted social funding per population in the same catchment area, there were significant associations between violent injuries and lower funding for Sure Start children’s centres and early years, family support services, services for young people and other children’s and families’ services (table 3b). There did not appear to be any association between violence and funding for youth justice or local authority expenditure on children and young people services, and there appeared to be a positive association for safeguarding children and young people services (table 3b).
Discussion
In our study of 1126 paediatric trauma admissions over a decade at a large MTC in the East Midlands, UK, injuries due to violence have been increasing over time, and this has occurred at the same time as reduced funding towards multiple social services for children and young people within the same catchment area. Since there was simultaneously an increase in proportion of violence and decreases in funding, we were unable to determine whether these factors were reliably associated independently of the overall temporal trends. Such trends are nevertheless compelling and worthy of further discussion in the context of the complex relationship between socioeconomic factors and vulnerability to violence.
Our study has captured all children with injuries severe enough to require assessment by the multidisciplinary specialist major trauma team, either via activation of a trauma call or by referral in from a local trauma unit, including all of those meeting criteria for inclusion in the research network database. Use of a prospectively collected department dataset to cross-reference has allowed reliable comparison of admission, mechanism, injury and outcome data over the period since the MTC opened in 2012, with data on readmissions available from 2016 onwards.
Large-scale investigations of injury patterns for children in the UK have shown that these can vary across different ages.3 The current study also demonstrates that there has been an additional trend in mechanisms and patterns of injury over time. The proportion of children requiring trauma centre assessment with injuries resulting from interpersonal violence has increased from just under one in ten in 2012 to more than one in four in 2021. These children are more likely to have torso injuries, rather than the more common pattern of head and limb injuries seen in children who have sustained injuries from road traffic collisions, falls or other non-violent mechanisms, mirroring the experience reported among injured adolescents in London.11 Children sustaining violent injuries more frequently require readmission to hospital, with a consequent impact on surgical and inpatient children’s services. Victims of interpersonal violence also have unique safeguarding needs11 12 with complex multiagency intervention and discharge planning requirements.
Trauma services have been evolving to try to address these needs. Development of a specialist resuscitative trauma surgery service in our centre has placed experienced and trained trauma surgeons alongside paediatric and other specialty surgeons to jointly manage children with major torso trauma and other complex injuries. In our centre and others, third sector youth workers are now embedded within the healthcare setting to offer early intervention for children and young people affected by violence,13 and there is some evidence of this being an effective intervention for vulnerable young people in the UK.14 However, community and public health interventions are needed to identify and address the root causes of violent trauma and to increase the focus on injury prevention.
In the 10 years since the East Midlands MTC opened, the regional government funding of children and young people’s services has reduced on five out of seven metrics, a concerning trend which mirrors national data.8 Overall spending reduced in the first 5 years (2012–2017) and though this trend has reversed more recently, the only areas in which there is increased funding are safeguarding children and young people’s services. Reduced real-terms funding have been reported in other services such as Sure Start and early years services, looked after children, family support and services for young people in the study region. These spending reductions correlate temporally with the observed increased incidence of violent injuries sustained by children and young people from across the East Midlands. Although the current study lacked sufficient data to formally assess interdependency, there appears to be a compelling case for closer inspection of this relationship. It is unknown why some of the funding sources appear to be associated with violence and others do not, but this question warrants further investigation.
There is strong evidence that social and economic deprivation is linked to knife crime5 7 15 16 and concerning data that rates of physical violence among young people are increasing in all age groups in England.5 Our study adds to the growing body of evidence of the impact of all types of violence on the individual, on the healthcare system and on the need for a comprehensive, appropriately funded social care system for children and young people. Adverse childhood experiences early in life lay the foundation for youth violence. It is also well reported that childhood trauma can result in significant long term morbidity and even increased likelihood of entering the criminal justice system as an offender in later life.17 Interventions to reduce violence must therefore begin in the early years and include proper support of families5; they must also address the specific needs of young people and be targeted to the communities experiencing the greatest deprivation.7 12 While post-trauma interventions can be immensely valuable in breaking the cycle, primary prevention strategies must be developed and prioritised if we are to see a reversal in trends of interpersonal violence and related injuries.
Limitations
The current study is observational, and derived from retrospective data, with all of the usual limitations in such a design. These include risk of selection bias, errors in data collection (with potentially missed patients), and the presence of other changes over time not included in our data. Due to the small number of observations in each time series (only nine time points), we were not able to fit the appropriate statistical models to assess interdependency between the reduction in funding and youth violence within the same catchment area, but instead propose the hypothesis that these are linked in a public health setting based on our data. Further interventional investigations may be warranted to better delineate these relationships. It is unknown whether our results can be generalisable to the remainder of the UK or internationally, and further investigations in other settings would be justified.
Conclusion
In a decade of paediatric admissions to a large trauma centre in the UK, there appears to be a trend towards greater proportions of injuries due to violence. This trend represents a public health concern. Social funding for children and young people reduced in multiple domains within the same catchment area, although formal assessment of the interdependence between the proportions of injuries due to violence and funding cannot be made. Further investigations are required to determine whether increased funding and provision of children and young people’s services might lead to a reduction in the overall proportion of injuries attributed to violence in children.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Institutional approval was granted prior to data collection.
Footnotes
Twitter @DavidNNaumann
Presented at This study was presented at PTS 2022, Portland Oregon (November 2022).
Contributors The study was conceived and designed by LM, DN, J-JR, LB and AB; data collection was undertaken by LM and SK; analysis and interpretation was performed by LM, DN and JB; and the manuscript was drafted by LM, DN and JB. All authors have reviewed and critically appraised the completed manuscript and approved the final version. AB is responsible for the overall content as the guarantor.
Funding There was no funding for the conduct of this study. Open access was funded by the University of Birmingham.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.