Article Text

Abstract
Adenoids (nasopharyngeal tonsils), being part of Waldeyer’s ring, are masses of lymphoid tissues located at the junction of the roof and the posterior wall of the nasopharynx. Adenoids play an important role in the development of the immune system and serve as a defence against infections, being the first organs that come into contact with respiratory and digestive antigens. The causes of adenoid hypertrophy are not fully known. They are most likely associated with aberrant immune reactions, infections, environmental exposures and hormonal or genetic factors. The aim of this review is to summarise the current knowledge of adenoid hypertrophy in children and associated diseases. Adenoid hypertrophy has many clinical manifestations that are frequent in the paediatric population and is accompanied by various comorbidities.
- Molecular Biology
- Audiology
- Adolescent Health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
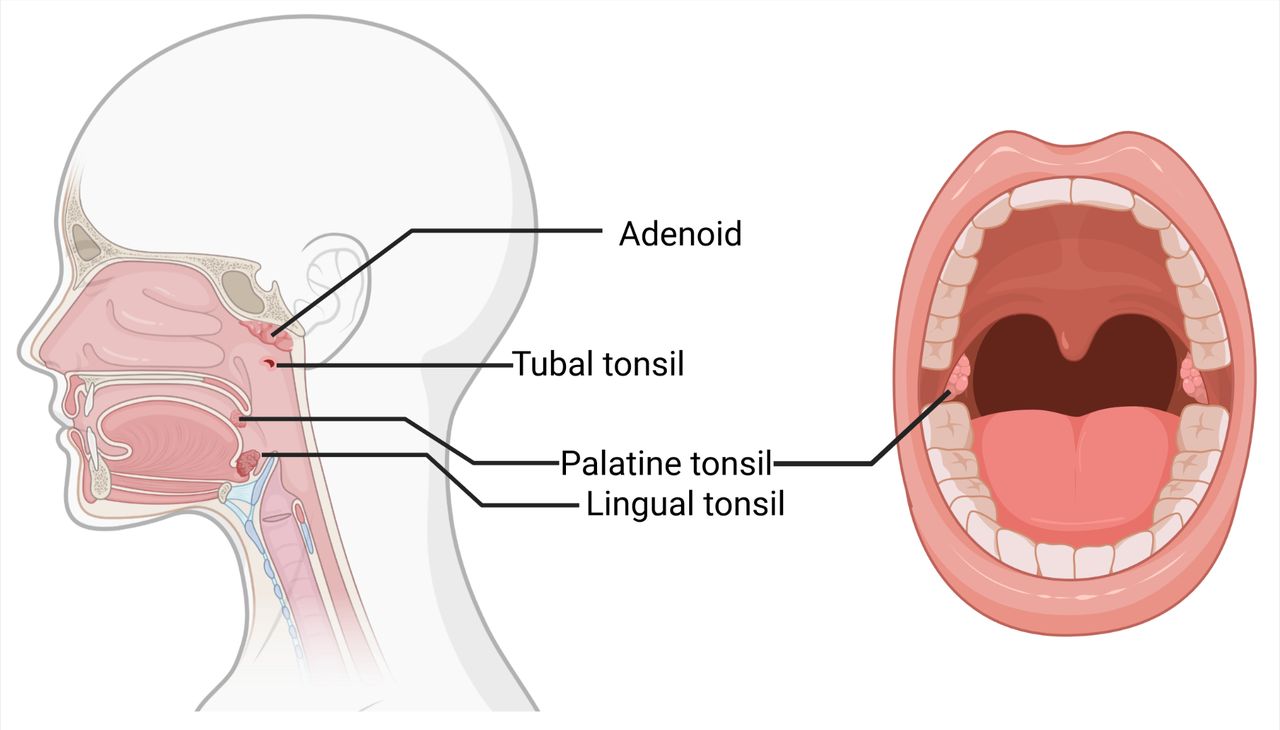
Waldeyer’s lymphatic ring is collectively composed of lymphoid tissue in the pharynx. The ring consists of the following four structures: adenoid, the tubal tonsils around the openings of eustachian tubes, the palatine tonsils (located between the anterior and posterior tonsillar pillars) and the lingual tonsils, located along the base of the tongue adjacent to the palatine tonsils at glossotonsillar sulcus1 2 (figure 1). The adenoid (also known as the nasopharyngeal tonsil) is centrally located in the nasopharynx attached to the area bordering the roof and the posterior wall of the nasopharynx. It lies posterosuperior to the border with the posterior nasal apertures (choanae) and to the side of lymphoid clusters located around the nasopharyngeal orifices of the eustachian tube.3 In 1661, the German anatomist Conrad Victor Schneider described this anatomical structure for the first time, which is now called the adenoid. However, the term ‘adenoid vegetations’ was not introduced until 1868 by the Danish physician Meyer. Meyer described these adenoid vegetations in an original research paper as ‘soft tumour masses of the nasopharynx that fill the room above the soft palate’.4 He also realised the relationship between nasal obstruction, mouth breathing, snoring, hearing impairment and adenoid hypertrophy (AH). Additionally, Meyer proposed a method of surgically treating adenoid hyperplasia by using a special knife inserted through the anterior nostrils into the nasopharynx.5

The anatomy of Waldeyer’s ring. Adenoids, palatine, lingual and tubal tonsils are lymphoepithelial tissues that make up the components of Waldeyer’s ring. Created with BioRender.
Anatomy and physiology of the adenoids
The adenoid develops relatively early in embryonic life, in the 12–14th gestation week.6 When fully mature, it has a quadrilateral shape with rounded edges weighing from 1.5 to 3.3 g.7 Its surface area is enlarged by having 3–6 folds separated by furrows that grow from the basal connective tissue sheath and constitute a support for the lymphatic tissue. The epithelium covering the surface of the adenoid is composed of pseudostratified ciliated columnar epithelium and is characteristic of the respiratory tract containing cell types that are necessary to mount a cellular and humoral-type immune response. Lymphoid follicles (small masses of tissues that involve aggregations of inflammatory cells, mainly B cells surrounded by a smaller number of T cells and dendritic cells) are arranged throughout these mucosal folds.6 The crypts of adenoid tissue look like tubular diverticula. Its fibrovascular core is surrounded by lymphoid tissue and the epithelial surface is comprised of non-keratinized stratified squamous epithelium along the luminal surface of the epithelium. The crypts are lined by stratified squamous epithelium and reticulated crypt epithelium. The reticulated epithelium contains both epithelial and non-epithelial cells, especially lymphoid cells.8 9
There are three major types of lymphoid cells: B cells, T cells and natural killer (NK) cells. B cells (or B lymphocytes) originate and mature in the bone marrow. When activated by antigens to proliferate and mature into effector cells, they form plasma cells that secrete immunoglobulins. T cells (or T lymphocytes) undergo their maturation in the thymus. One class of T cells differentiate into cytotoxic T cells which kill targeted cells, infected with viruses. The second class of T cells (helper T cells) help activate other cells, such as macrophages, B cells and cytotoxic T cells. Effector helper T cells secrete cytokines—signal proteins which act as local mediators. A third type of lymphoid cells, NK cells, can identify and attack some abnormal cells, that is, virus-infected cells. They are considered to be an important part of the innate immune defence against intracellular pathogens, as they lack antigen-specific receptors.10 11
Together with the diffuse lymph nodes within the nasopharyngeal mucosa, adenoid forms part of the nasal-associated lymphoid tissue (NALT) system, which is the site of first contact with respiratory and digestive antigens. It comprises lymphocytes, plasma cells, macrophages and dendritic cells which are responsible for first-line defence in a healthy individual, affording protection against microbial invasion and prevention of autoimmunity. These lymphoid tissue cells allow the adenoid to recognise antigens and thereby elicit an immune response.12 13
Apoptosis, or programmed cell death, is an important phenomenon that helps in maintaining homeostasis as the adenoids constantly contact with new antigens. This process also aims to eliminate autoreactive or non-specific immune cells within the organs. In normal conditions, apoptosis protects from autoimmune diseases or pathologic lymphoid organ hyperplasia.14 Abnormal immune activation or regulation of the lymphoepithelial tissue may potentially result in several medical complications. Some patients develop pathologic immune-related processes, such as chronic adenoiditis or rhinosinusitis. Other patients develop conditions associated with enlarged adenoid that causes anatomic obstruction of the nasopharynx, for example, obstructive sleep apnoea.8 Enlarged adenoid tissue can also mechanically obstruct the eustachian tube orifice, which in consequence leads to middle-ear negative pressure. Furthermore, pathogens may migrate from the adenoid surface to the middle ear space. This can result in serious middle-ear conditions, such as otitis media with effusion (OME).15
Immunological role
Contact between antigens and immunocompetent cells is possible thanks to microfold cells (M cells).16 Their characteristic feature is the presence of surface microfolds and cytoplasmic cavities forming crypts. Within these crypts are lymphocytes, macrophages and neutrophils. The primary function of M cells is to capture and transport antigens to the subepithelial layers. When there is a chronic inflammation within the epithelium, the number of ciliated and M cells may become reduced.17 18 Once the antigens cross the epithelium, they are processed by antigen-presenting cells (APCs). Among these APCs, there are macrophages, dendritic cells and B lymphocytes. Lymphocytes have the ability to recognise an antigen and to respond to a specific immune response. This is possible as a population of T and B cells collectively bear on their surface multiple antigen receptors that vary in their antigen-binding sites and are capable of recognising a wide range of antigens.10 11
The action of the immune system can be classified into two distinct parts: the primary and the secondary immune response. If the encountered antigen is novel, the primary immune response is activated. If the organism is re-exposed to antigen, a secondary immune response is stimulated by T cell proliferation and/or secondary antibody production by B cells.19 During primary response, activation, proliferation and differentiation into a T cell-specific to this antigen ensue after a successful recognition of the antigen by a helper T cell. These T cells stimulate naïve B cells, which then migrate to germinal centres and differentiate into antigen-specific plasma cells and memory B cells. Plasma cells produce antibodies specific to the antigen, while memory cells remain to protect against successive contact with the same antigen. Plasma cells and memory B cells are able to leave the germinal centres through high endothelial venules and migrate to further mucosal sites, for instance, the nasal mucosa, where they can differentiate into specific immunoglobulin-producing cells (figure 2).20–22 Plasma cells are capable to produce all five immunoglobulin classes, with predominant production of IgA in nasopharyngeal mucosa.2

{kind=link}
{kind=link}
The diagram of the structure and immune cell composition of different human palatine tonsil compartments. The maturation and differentiation of B cells in the germinal centre (GC) of the lymphoid follicle. Activated precursor B cells differentiate into short-lived extrafollicular plasma cells or migrate to GC where in the dark zone they differentiate into centroblasts. After clonal expansion and somatic hypermutations, centroblasts differentiate in the light zone into centrocytes. Next, apoptosis is activated in these cells or they are selected by T cells (follicular helper T) in the presence of follicular dendritic cells (FDCs) and undergo further differentiation into long-term memory or plasma cells B. Created with BioRender.
Pathogenesis of AH
Experimental studies summarised in a review by Kuper et al show that the adenoid plays the earliest immunological role in the NALT system.23 The immunological functions of the adenoids lead to their rapid growth during the early years of life. During childhood, its shape and size alter significantly where dynamic growth is seen between ages 3 and 6 years, which may be related to relatively slower growth of the nasopharyngeal cavity. After the age of 6, the growth of the adenoid becomes inhibited under normal conditions, while the nasopharyngeal cavity grows and widens the respiratory tract.8 Later in life, the lymphoid tissue undergoes involution (due to the fibrous tissue expansion and fatty atrophy),8 so that in most adults, the adenoid appears in a residual form, but it never completely disappears.24 Macroscopic changes accompany microscopic and functional changes therein. These adenoids are most immunologically active between 4 and 10 years of age in humans and their involution begins after puberty.20 As a result, the B cell population decreases and the ratio of T cells to B cells increases. When the adenoids become infected, inflammation of the crypts leads to the inactivation of immunologically active cells where the ability to transport antigens decreases, which in turn leads to metaplasia into a multilayered squamous epithelium. Such changes lead to inefficient antigen uptake and impaired cell functions.25
The causes of AH in children are not fully known. They are most likely associated with immune reactions, hormonal factors or genetic factors.8 Among immune disturbances, altered production of cytokines is described. For example, upregulation of interleukin (IL)-32 in adenoid tissue was shown, which might have a potential effect on AH progression through stimulation of proinflammatory cytokines production as well as pyroptosis in human nasal epithelial cells mediated by NOD1/2/TLR4/NLRP3 pathway (nucleotide-binding oligomerization domain-containing protein/toll-like receptor/nucleotide-binding oligomerisation domain, leucine-rich repeat and pyrin domain-containing proteins).26 Moreover, elevated levels of proinflammatory cytokines such as high-sensitivity C reactive protein, IL-1 and IL-10, interferon-γ (IFN-γ), TNF-α (tumor necrosis factor α) as well as intercellular adhesion molecule-1 in children with AH have been observed.27 Genetic factors include, among others, polymorphisms in genes coding: SCGB1D4 (IFN-γ stimulated cytokine regulating chemotaxis of immune cells), TLR2 and TLR4 (play a key role in the regulation of the immune system through recognition of molecular patterns commonly found on pathogens (pathogen-associated molecular patterns)).28 29
Normally, there is a well-established balance between the natural flora of the adenoid and the immune response, however, this can be disturbed by recurrent viral and bacterial infections and colonisation by pathogens. Frequent infections or allergies in the upper respiratory tract often give rise to hypertrophic processes.30 31 The most common bacteria isolated from adenoid tissue are Haemophilus influenza, Streptococcus pneumoniae, Streptococcus pyogenes and Staphylococcus aureus. In chronic infections, anaerobic bacteria pathogens are also present.32
Exposure to gastric juice during gastro-oesophageal reflux disease may also contribute to AH, especially in newborns and younger children.33 Passive smoking is another risk factor for AH.8 30
Clinical aspects of AH
Adenoid becomes enlarged in the early years of life due to their involvement in the body’s immune mechanisms. Some patients can develop an abnormal immune response, which in turn leads to chronic inflammation of the adenoid, which may then spread to adjacent areas of the mucosa, for example, of the nose, sinuses and middle ear.34 Chronic adenoiditis develops in cases when foreign antigens elude immune response, become trapped in the crypts and proliferate before an effective immune response can be activated.20 Recurrent acute or chronic infection of the adenoid often coexists with its hypertrophy, which may additionally cause obstruction of the nasopharynx and/or at the mouth of the eustachian tubes. Hypertrophy of the adenoid reduces or blocks passages in the upper respiratory tract and usually leads to long-term consequences if the condition is left untreated.35 36 The estimated prevalence of this condition in the paediatric population is 34%.37
The most common form of the adenoid disease is recurrent acute or chronic inflammation associated with hypertrophy. The inflamed adenoid is usually covered with a mucopurulent discharge with a characteristic flow of secretions running down the back of the pharynx.38
The mucus found in the respiratory tract acts as a protective barrier against the ingress of bacteria and viruses. When the mucosa makes contact with pathogens then the production of pro-inflammatory cytokines increases and there is an enhanced immune response.39 Whenever long-term chronic inflammation arises, this barrier is damaged and may contribute to there being bacterial superinfection. Microorganisms present in inflammatory secretions are able to rapidly multiply and produce biofilm, which makes them difficult to be removed by the host’s immune system.40 Bacterial superinfections lead to increased symptoms associated with AH, including elevated levels of pathological secretions with the nasal cavities. It has also been demonstrated that the coexistence of allergic rhinitis with AH is also associated with more severe symptoms and longer persistent symptoms, including persistent runny nose.41 Some variability was also noticed during the year, where in winter the adenoid is to a greater extent covered with pathological discharge compared with summer.42
Symptoms accompanying chronic adenoiditis are chronic runny nose, nasal obstruction, snoring, an altered breathing pattern from nasal to oral and bad breath. Due to the distinct connections with the middle ear, nose and paranasal sinuses, a clinical evaluation of the adenoid should be based on a comprehensive otolaryngological examination.8
Adenoids causing airway obstruction can lead to43 44:
Obstructive sleep apnoea syndrome (OSAS).
Chronic sinusitis.
OME.
Formation of malocclusions and developmental anomalies in the craniofacial area.
Speech disturbances and articulation errors.
Disorders in physical and intellectual development.
Obstructive sleep apnoea
The first report of sleep disturbances in children was dated to Hill, who noticed that snoring, mouth breathing and restlessness at night may cause ‘backwardness and stupidity’.45 Nearly 100 years later, in 1973, Guilleminault described sleep apnoea for the first time as: ‘A new clinical syndrome, with repeated episodes of cessation of breathing and frequent arousal at night that leads to insomnia and tiredness next day’.46 Three years later, the first case series of obstructive sleep apnoea in the paediatric population was reported.47
Epidemiology, pathogenesis, diagnostic criteria and treatment methods of OSAS in adults differ from paediatric OSAS.48 Its prevalence is estimated at about 1%–5%48 of the paediatric population with symptoms peaking between the ages of 2 and 8 years due to the adenotonsillar hypertrophy.48 49 Child OSAS forms by a multifactorial mechanism as indicated by its pathophysiology. It is associated with the collapse and narrowing of the upper respiratory tract, leading to complete or partial obstruction of patency during sleep. The aetiopathological factors of this syndrome include craniofacial anomalies, Down’s syndrome, obesity, neuromuscular disorders and laxity/tenuity.48 49 However, its most common cause in children is the overgrowth of lymphoid tissue within the Waldeyer’s ring.50 Genetic alterations in children with AH accompanied by OSAS were also analysed using whole-genome microarrays. Disturbances in the expression of numerous genes in adenoid tissue samples from children with OSAS were revealed, among which the greatest changes were observed for phosphoserine phosphatase (PSPH). PSPH, an enzyme encoded by the gene PSPH, is responsible for the last step in L-serine biosynthesis. PSPH deficiency is thought to cause facial abnormalities, growth and psychomotor retardation. This protein was expressed in children with OSAS, but almost never in children with recurrent tonsilitis. Interestingly, pharmacological inhibition of this enzyme led to the inhibition of T and B lymphocyte cells proliferation, increased programmed cell death in tonsillar cell cultures and stimulate apoptosis.51
Collapsing and narrowing of airways during sleep is the main cause of OSAS. The main difference between a clinical picture of OSAS in children and adults is the presence of permanent impairment of airflow in children, while in adults these disorders are often variable in time.52 It is established that the presence of Waldeyer’s ring lymph hypertrophy does not necessarily cause apnoea, even in patients with large tonsils reaching each other and extending to the midline. The number of apnoea episodes was found not to increase with tonsil size, but their duration increased with a deeper impairment to oxyhaemoglobin saturation.50 The hallmarks of OSAS are multiple shortnesses of breath, sleep apnoea, desaturation and awakening during sleep. Additionally, symptoms such as excessive sweating, restless sleep, bed-wetting, drooling, sleepwalking and nightmares may occur. During the day, children may become drowsy, and suffer from headaches, dry mouth, problems with swallowing, as well as bad breath. The consequences of hypoxia and the lack of proper rest at night relate to complications in the psychophysical development of the child. Such children may present with various behavioural disorders such as hyperactivity, concentration disorders, learning problems and aggression. Sleep is an important element in the development and adolescence of children, especially during their intense brain development. The central nervous system intensively develops from childhood to adolescence and is thus most vulnerable to damage during this time. Studies have confirmed disorders of neurocognitive development whenever breathing disorders occur during sleep. Studies of neurocognitive functions in snoring and non-snoring children showed that the former resulted in decreased levels of concentration, memory, learning abilities and intelligence.53 54
Otitis media with effusion
OME is defined as a condition where fluid in the tympanic cavity accumulates when there are no features of acute otitis media present. It occurs while the continuity of the eardrum membrane is preserved.55 Local inflammation leads to metaplasia of the epithelium lining the tympanic cavity and to an accumulation of fluid within the middle ear. The exudate is mucinous or serous-mucous.56 Persistent OME refers to a situation when symptoms last for at least 3 months.57 OME may be asymptomatic, or patients may experience various forms of ear discomfort, hearing loss, tinnitus, dizziness or a feeling of fullness in the ear. The otoscopic picture may vary depending on the nature and duration that the fluid is present. Its most common symptoms are a thickening of the eardrum with a yellowish or amber tint, or bruising to the eardrum with a bright white colouration.55 58 Persistent ear effusion leads to permanent changes in the tympanic membrane structure which intensify due to being exposed to prolonged negative pressure. Untreated exudate may lead to irreversible consequences, such as calcification and/or atelectasis of the tympanic membrane, the formation of retraction pockets, tympanosclerosis and cholesteatoma. Permanent conductive hearing loss, which may occur due to the presence of middle ear fluid, usually leads to delayed or impaired speech development, communication difficulties, limited vocabulary, disturbances in attention and lower academic performance.59
The pathophysiology of OME in children is complex. It includes specific host, environmental, genetic and social risk factors.60 The relatively higher prevalence of OME in children compared with adults is thought to be related to the immaturity of the eustachian tube (ET). The eustachian tube is shorter and more horizontal in children. Additionally, its cartilage is more dense with less elastin in children compared with adults. Moreover, the mucosal lining of the children’s ET is thicker and more folded. Also, lymphoid tissue aggregation that built the tubal tonsil is more developed in children.61 Bacteria accumulating in the nasal cavity explains the increased risk of ear infections,62 nevertheless, conventional microbiological tests on middle ear exudates do not always show bacterial growth. The sensitivity of bacterial detection in middle ear infections has been improved thanks to the introduction of the PCR technique. This method is useful in detecting slowly growing pathogens that are difficult to culture in a diagnostic lab.63
It is therefore suspected that OME is a complex immune process within the tympanic cavity, influenced by persistent respiratory viruses interacting with impaired defence responses. Recent studies have shown increased amounts of IL-4, IL-11 and INF-gamma but decreased levels of IL-1, TNF-α and TGF-beta (transforming growth factor) in purulent and mucous exudates of the middle ear, pointing to the role of humoral defence responses in the pathogenesis of OME.64–66
Performing surgery on an enlarged adenoid is believed to remove infected tissue that is the source of infection, equilibrate middle ear pressures and improve ventilation.67 It is proven that the size of the adenoid does not influence the viscosity of middle ear secretions.68 Adenoidectomy should thus be considered in children with OME with associated nasal symptoms of airway obstruction, children with persistent OME aged ≥4 years or children aged <2 years with recurrent acute otitis media.69
Chronic sinusitis
The criteria for diagnosing chronic rhinosinusitis (CRS) in children are when two out of the following symptoms are present: nasal obstruction, nasal discharge (anterior or posterior runny nose), cough and headache where the symptoms persist for at least 12 weeks.70 The prevalence of CRS is estimated at 2%–4%,70 with two age groups most affected (5–10 year olds and 10–15 year olds).71 Chronic adenoiditis is however a separate disease and is often difficult to differentiate from chronic sinusitis. Over the last several decades, there have been many studies confirming a relationship between these two pathologies.72–75 A detailed discussion of the link between AH and CRS is beyond the scope of this paper and is detailed in a review by Bulfamante et al.75 The results of some studies regarding microbiology, biofilm and host immunity are briefly summarised in table 1.
Relationship between adenoid hypertrophy and chronic sinusitis
Adenoid tissue can contribute to paediatric CRS development by several different mechanisms, including nasal obstruction and being a bacterial reservoir.34 75 A study that focuses on the assessment of bacterial colonisation of adenoids and sinuses shows a significant presence of the same bacterial strains in both locations.73 Biofilm concentration is significantly higher in samples taken from patients with CRS compared with patients with OSAS.72 Biofilms have been shown to support pathogen subsistence and further impair the immune function of the adenoids.34
Reduced amounts of IgA and APCs were found in the adenoid tissue of patients diagnosed with CRS, which favours the development of bacterial infection. The proliferation of bacteria activates the inflammatory response and hypertrophy of the adenoid. There is a vicious circle in which the frequency of infections increases, leading to an enlarged volume of the adenoid and the emergence of clinical symptoms typical of CRS.74 Treating CRS surgically is reserved for those patients who failed maximal medical therapy (nasal lavage with a saline solution, corticosteroid nasal spray, antibiotic therapy in case of acute bacterial infection).70 Adenoidectomy (without tonsillectomy) is often the first surgical treatment option in children with CRS due to the strong relationship between these conditions; its effectiveness is estimated at 47%–58%.76 Younger children (<12 years of age) in particular, may benefit from this procedure.70 Treating CRS by adenoidectomy is justified because both the obstructive tissue of the airways and the bacterial biofilm are reduced during the procedure.77
Influence of AH on craniofacial development if untreated
The shaping of the face, occlusion and the development of temporomandibular joints is a complex process, dependent on the surrounding soft tissues, especially the muscles that pull the jaw down and forward as it grows. Craniofacial growth is also stimulated by a number of physiological processes such as biting and chewing food, swallowing, breathing and speech; breathing being of particular importance in shaping the face. The nasal respiratory tract is considered to be the normal means of breathing in humans. During physiological nasal breathing, the muscles of the cheeks, lips, tongue, palate and floor of the mouth are in a state of functional equilibrium.78
AH obstructs patency of the upper respiratory tract and causes the breathing path to shift from nasal to oral.79 For such patients, breathing is possible via the lifting of the soft palate and lowering of the root of the tongue. A permanent ‘adenoid facies’ is observed in the structure and appearance of the craniofacial face when there is long-lasting nasal obstruction caused by the overgrowth of adenoid tissue. Characteristic features of this condition include a relatively short upper lip, receding hyoid bone, lowered and retracted chin, a recessed lower dental arch in relation to the upper, narrow upper dental arch and an elongated face. Such patients tend to have an oversize bite/occlusion, an open bite and a unilateral or bilateral crossbite.80
Constant breathing through the mouth and a lowering of the lower jaw causes the tongue to change its physiological position from being on the roof of the palate to a flat position on the bottom of the mouth. The jaw is deprived of the shaping effect of the tongue and consequently, the jaw bones become elongated and narrowed by the action of the cheek muscles. Oral respiration reduces the atmospheric air pressure acting on the palate from the nasal cavity, leading to the formation of a high hard palate.80 81 Such changes of maxillofacial dysmorphism occur in cases of severe, non-treated AH.82
When patients are qualified sufficiently early for surgery to remove the hypertrophic adenoid and to restore the physiological path of nasal breathing, then this enables the growth pattern of the facial part of the skull be modified. Studies on patients undergoing adenoidectomy demonstrate that they have an increased vertical size to the lower part and to the total height of the face after the procedure.81
Summary
The adenoid, being part of Waldeyer’s lymphatic ring, is an important place of contact with foreign antigens entering the body through the respiratory and digestive tracts. Understanding the physiology of adenoid tissue and the role the adenoid plays in the body’s immune processes allows an appropriate diagnostic and therapeutic procedure to be chosen. Further studies are needed to examine the relationship between environmental risk factors and comorbidities (such as gastro-oesophageal reflux disease, allergy, passive smoking), immune reactions, biofilm formation and AH. Recognition of these causes is crucial for patient-tailored treatment. Unsurprisingly, a collaboration between physicians from different medical specialties (otolaryngologists, paediatrics, allergologists, dentists) is very important for evaluating these alternative disease etiologies. A better understanding of the pathophysiology of this condition is essential to develop novel preventive and treatment strategies. Knowledge of the immunological processes that lead to AH (role of proinflammatory cytokines, ie, IL-32, IL-14) potentially could be used to prevent this disease.
Summary box
The causes of adenoid hypertrophy in children are not fully known. They are most likely associated with immune reactions, hormonal factors or through genetic factors.
Waldeyer’s ring tissue serves as a defence against infection and plays an important role in the development of the immune system.
Hypertrophy of the pharyngeal tonsil reduces or blocks passages in the upper respiratory tract and usually leads to long-term consequences if the condition is left untreated.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors AN contributed to conceptualisation, writing (original draft preparation), guarantor. LPC contributed to supervision. AK contributed to writing (original draft preparation). GM-N contributed to writing (review, supervision). JB contributed to conceptualisation, resources.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.