Article Text

Abstract
Objective To investigate whether effects of antenatal corticosteroids on neonatal outcomes in preterm infants with very low birth weight were different by plurality.
Design Nationwide prospective cohort study.
Patients Twins and singletons with very low birth weight (<1500 g) who were born between 23+0 and 33+6 weeks of gestation and registered in the Korean Neonatal Network from January 2014 to December 2019.
Main outcome measures Morbidity and mortality before discharge from neonatal intensive care unit.
Results Among a total of 9531 preterm infants with very low birth weight, there were 2364 (24.8%) twins and 7167 (75.2%) singletons. While 83.9% of singletons were exposed to at least one dose of antenatal corticosteroids, so were 87.9% of twins.
Interaction analysis demonstrated that there was no significant difference in the effect of antenatal corticosteroids on morbidities or mortality between twins and singletons in either gestational age group (23–28 weeks or 29–33 weeks).
Antenatal corticosteroids significantly decreased the risk of surfactant use (adjusted relative risk (aRR): 0.972 (95% CI: 0.961 to 0.984)), high-grade intraventricular haemorrhage (aRR: 0.621 (95% CI: 0.487 to 0.794)), periventricular leucomalacia (aRR: 0.728 (95% CI: 0.556 to 0.954)) and mortality (aRR: 0.758 (95% CI: 0.679 to 0.846)) in the gestational age group of 23–28 weeks. In the gestational age group of 29–33 weeks, antenatal corticosteroids significantly decreased the risk of surfactant use (aRR: 0.914 (95% CI: 0.862 to 0.970)) and mortality (aRR: 0.409 (95% CI: 0.269 to 0.624)) but increased the risk of sepsis (aRR: 1.416 (95% CI: 1.018 to 1.969)).
Conclusion This study demonstrates that effect of antenatal corticosteroids on neonatal outcomes of preterm infants with very low birth weight does not differ significantly by plurality (twin or singleton pregnancy).
- mortality
- twins
- neonatology
Data availability statement
Data are available upon reasonable request. The Korean Neonatal Network (KNN) Publication Ethics Policy adheres to the following research data management and access guidelines: all information about patients and participating NICUs is confidential and may be used by individuals for approved research purposes. If an individual or institution that is not affiliated with KNN wants to use the data, it must make an official request to the KNN publication-Ethics Committee and obtain approval from the network.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Antenatal corticosteroids (ACS) administered before preterm delivery can decrease neonatal morbidity and mortality in singleton pregnancies. However, data about such effects of ACS in multiple pregnancies are still limited.
WHAT THIS STUDY ADDS
The effect of ACS administered before preterm delivery on neonatal morbidity and mortality does not differ by plurality (twin or singleton pregnancy).
Infants exposed to ACS were more likely to survive and require less surfactant therapy in both 23–28 weeks and 29–33 weeks gestational age groups.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights the need for further investigation to fully understand effects of ACS on multiple pregnancies, given the increasing prevalence of multiple pregnancies worldwide.
Introduction
Antenatal corticosteroid (ACS) has been established as the standard therapy for pregnant women at risk of preterm delivery within 7 days between 24+0 and 33+6 weeks of gestation.1 Currently, ACS is equally recommended for twin and singleton pregnancies with the same regimen based on previous studies.2–4 A recent study has shown that a complete course of ACS administered before preterm twin delivery is associated with a significant decrease in neonatal mortality, short-term respiratory morbidity and severe neurological injury in a magnitude similar to those observed for a singleton pregnancy.3 However, data that demonstrate comparable effects of ACS therapy in twin pregnancies are limited.
As a result of increasing childbirth age and use of assisted reproductive technology, twin pregnancies are increasing in many countries, including Korea.5 6 However, twin pregnancies are more likely to have preterm birth, low birth weight and longer hospital stays than singleton pregnancies.7 8 In addition, mono-chorionicity, birth weight discordance and obstetric complications associated with multiple pregnancies may result in adverse perinatal outcomes.9–11
Recently, the mortality of extreme preterm multiplets has decreased to a level comparable with that of singletons born at the same gestational age along with increased use of ACS therapy.12 However, many studies have reported conflicting results regarding equivalent effects of ACS on neonatal outcomes of twins and singletons.3 13–18 To date, there have been no clinical trials designed to investigate the effect of ACS in twins. A meta-analysis on ACS therapy has also highlighted the need for additional studies on multiple pregnancies.4
Thus, the purpose of this study was to investigate whether effects of ACS administered before preterm delivery on neonatal outcomes of twins and singletons were comparable.
Materials and methods
Study design and participants
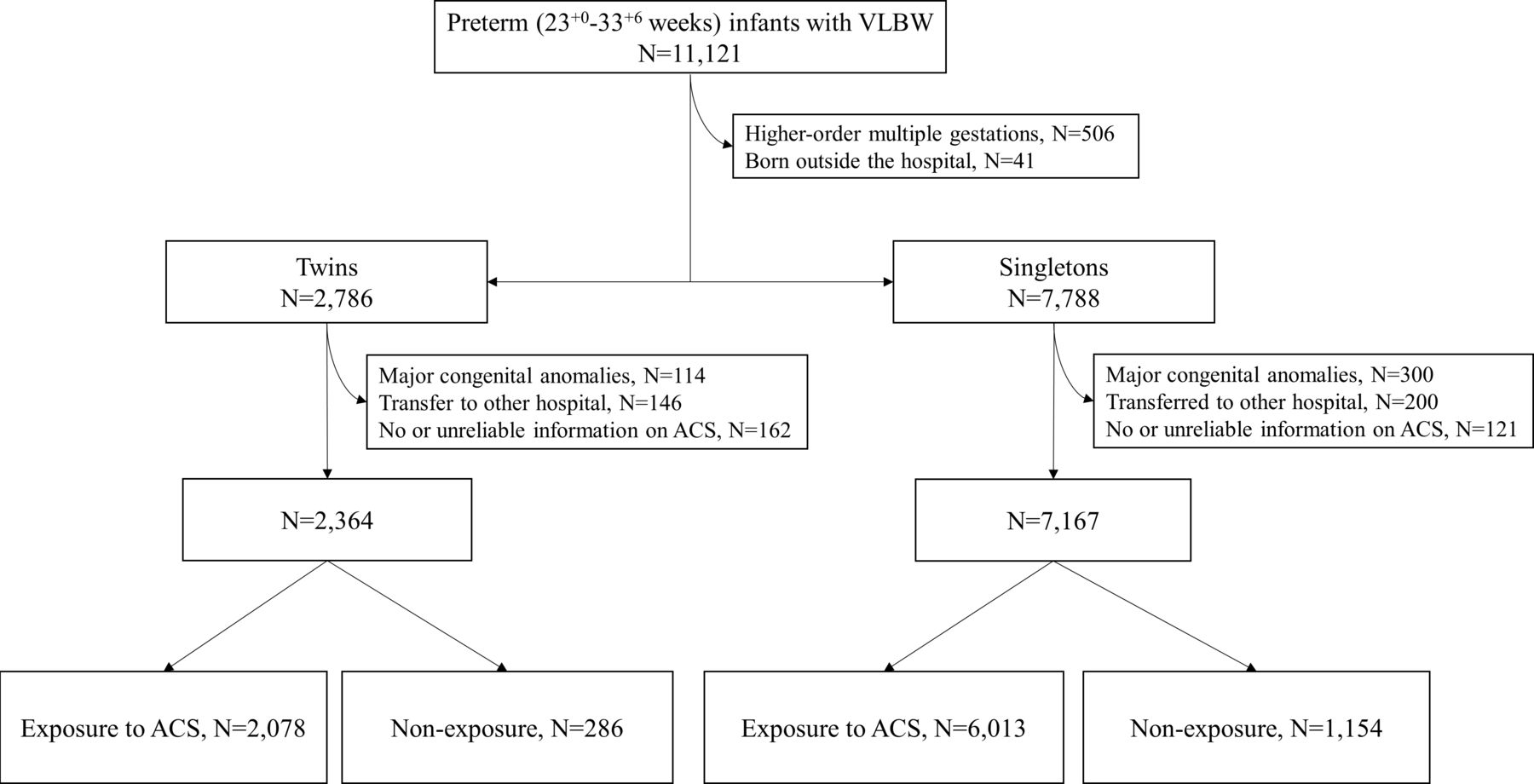
Information on the study population is presented in figure 1. Data collected prospectively through the Korean Neonatal Network (KNN), a nationwide very low birthweight (VLBW, <1500 g) infant registry participated by 61 neonatal intensive care units across South Korea,19 were used for this study. A total of 11 121 infants with VLBW born preterm (between 23+0 and 33+6 weeks of gestation) between January 2014 and December 2019 were enrolled. Exclusion criteria were: high-order multiple gestations (≥triplets), birth outside the hospital, major congenital anomalies, transfer to other hospitals, no or unreliable information on ACS. Finally, 2364 twins and 7167 singletons were analysed. ACS therapy was defined if the pregnant women had received at least one dose of any kind of corticosteroids before preterm delivery. Variables collected included gestational age, birth weight, small for gestational age, sex, maternal age, maternal diabetes mellitus (DM), maternal hypertension, chorioamnionitis, premature rupture of membrane, caesarean section, in vitro fertilisation (IVF), surfactant use, sepsis, high-grade intraventricular haemorrhage (IVH), periventricular leucomalacia (PVL), surgically treated patent ductus arteriosus, bronchopulmonary dysplasia (BPD), advanced retinopathy of prematurity (ROP) and mortality. Definitions for different variables are provided in online supplemental materials. The analysis of neonatal morbidity was performed for infants who survived before discharge, while the analysis of mortality was performed for the total population.
Supplemental material
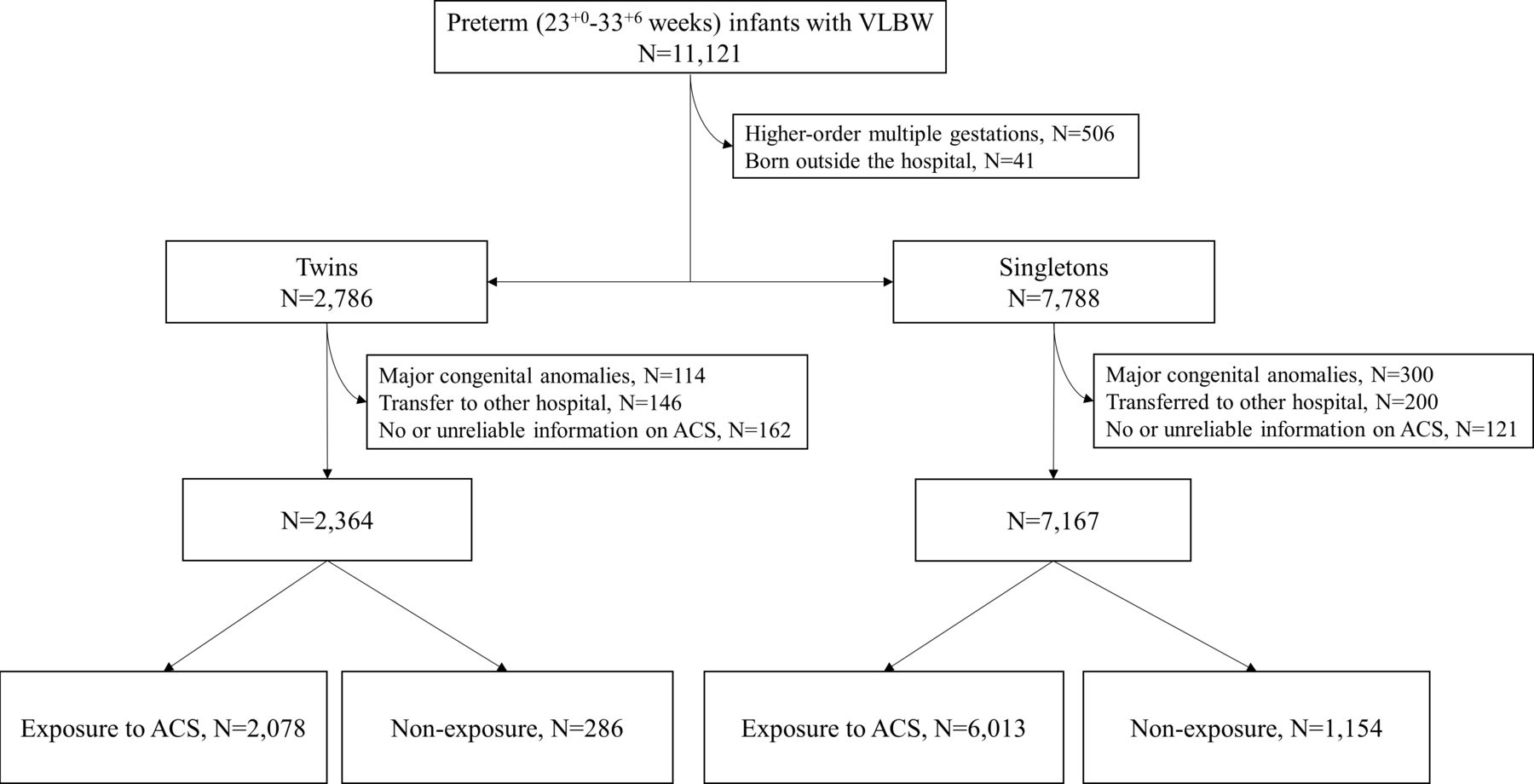
Flow chart showing the selection of study population. ACS, antenatal corticosteroid; VLBW, very low birth weight.
Patient and public involvement
Patient and/or the public were not involved in the design, or recruitment, or conduct, or reporting, or dissemination of plans of the study.
Statistical methods
Rates of neonatal outcomes between infants exposed to ACS and infants without such exposure are presented along with risk difference and 95% CIs. To investigate whether associations between ACS and neonatal outcomes were altered by plurality (twins vs singletons), the interaction effect between ACS and twin pregnancies on neonatal outcomes was evaluated by adding interaction terms (ACS×twins) in Poisson regression models. The crude and adjusted relative risks (aRRs) and 95% CI for the individual effects of ACS and twins were obtained in the second model without the interaction term.
All models were fitted with generalised estimating equations approach for the correlation between a pair of twins from a mother. Covariables in regression models were gestational age, birth weight, sex, maternal age, maternal DM, maternal hypertension, premature rupture of membrane, caesarean section and IVF. Chorioamnionitis was excluded from the analyses due to substantial missing values (17.6% in twins and 14.5% in singletons).
For each outcome, a backward-stepwise method was used to remove the variable with the highest p value, and variables in final model were selected that showed minimal quasi-likelihood under the independence model criterion value.20–22 To confirm multicollinearity, variance inflation factor values were checked for all covariates, which were all less than 5, indicating no significant multicollinearity (1.002~2.989). The level of significance was set at p<0.05. All statistical analyses were performed using SPSS V.25.0 (IBM Corp) and ‘geepack’ and ‘car’ package R V.4.1.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Exposure to ACS
Among 2364 twins, 2078 (87.9%) infants were exposed to at least one dose of ACS before preterm delivery. Among 7167 singletons, 6013 (83.9%) infants were exposed to at least one dose of ACS before preterm delivery (figure 1).
Comparisons of perinatal baseline characteristics between infants exposed to ACS and infants without ACS exposure
Twins exposed to ACS were born at a later gestational age (mean (SD), 28.08 (2.19) vs 27.75 (2.50) weeks) compared with those without ACS exposure (table 1). However, there was no difference in gestational age (mean (SD), 28.49 (2.52) vs 28.39 (2.78) weeks) or birth weight (mean (SD), 1060 (281) vs 1073 (289) g) between singletons exposed to ACS and those without ACS exposure. Singletons exposed to ACS had higher rates of maternal DM (9.9% vs 7.7%; p=0.019), maternal hypertension (29.1% vs 24.8%; p=0.003) and caesarean section (77.1% vs 69.9%; p<0.001) than those without exposure. In both twins and singletons, infants exposed to ACS were more likely to have higher rates of premature rupture of membrane and be conceived through IVF from older mothers than those without exposure.
Comparisons of perinatal baseline characteristics between infants exposed to ACS and infants without ACS exposure
Interaction between ACS and twin pregnancies on neonatal outcomes
We investigated whether effects of ACS on neonatal outcomes differed between twins and singletons. Because neonatal outcomes are substantially dependent on gestational age, comparison of ACS effects on neonatal outcomes by plurality was performed by stratifying the study population into two gestational age groups: an gestational age group of 23–28 weeks and an gestational age group of 29–33 weeks.
Interaction analyses within 23–28 weeks (table 2) and 29–33 weeks (table 3) gestational age groups found no significant difference in the association of ACS therapy with any neonatal outcomes between twins and singletons (p>0.1 for all).
Comparisons of neonatal outcomes between infants exposed to ACS and infants without ACS exposure born at 23–28 weeks of gestation
Comparisons of neonatal outcomes between infants exposed to ACS and infants without ACS exposure born at 29–33 weeks of gestation
Independent effects of ACS and twins on neonatal outcomes
In the second model excluding the interaction term, we calculated aRR and 95% CI for individual effects of ACS and twins on each neonatal outcome. In the gestational age group of 23–28 weeks, exposure to ACS was significantly associated with a lower risk of surfactant use (aRR: 0.972 (95% CI: 0.961 to 0.984)), high-grade IVH (aRR: 0.621 (95% CI: 0.487 to 0.794)), PVL (aRR: 0.728 (95% CI: 0.556 to 0.954)) and mortality (aRR: 0.758 (95% CI: 0.679 to 0.846)) (figure 2A). Twins were associated with higher risks of high-grade IVH (aRR: 1.466 (95% CI: 1.178 to 1.825)) and advanced ROP (aRR: 1.193 (95% CI: 1.069 to 1.331)) than singletons.

{kind=link}
{kind=link}
Forest plot showing results of logistic regression for effects of ACS and twins on neonatal outcomes: (A) 23–28 weeks of gestation; (B) 29–33 weeks of gestation. For each neonatal outcome, solid dots represent the adjusted OR and lateral lines represent the 95% CI. Adjusted relative risk and 95% CI were obtained from multivariable Poisson regression models using generalised estimating equations. ACS, antenatal corticosteroid; IVH, intraventricular haemorrhage; PDA, patent ductus arteriosus; ROP, retinopathy of prematurity.
In the gestational age group of 29–33 weeks, exposure to ACS was significantly associated with lower risks of surfactant use (aRR: 0.914 (95% CI: 0.862 to 0.970)) and mortality (aRR: 0.409 (95% CI: 0.269 to 0.624)), but a higher risk of sepsis (aRR: 1.416 (95% CI: 1.018 to 1.969)) (figure 2B). Twins showed a lower risk of BPD (aRR: 0.798 (95% CI: 0.648 to 0.982)), but a higher risk of PVL (aRR: 1.735 (95% CI: 1.256 to 2.396)) than singletons.
Discussion
In this nationwide cohort study, we demonstrated that effects of ACS therapy administered before preterm birth on neonatal outcomes were not significantly different by plurality. Mortality and surfactant use were reduced by ACS exposure in both gestational age groups. ACS exposure was associated with decreased risks of high-grade IVH and PVL in infants born at 23–28 weeks of gestation, but increased the risk of sepsis in infants born at 29–33 weeks of gestation.
ACS therapy for mothers at risk of impending preterm delivery is the most effective evidence-based strategy to reduce the mortality and morbidity of their preterm offspring. However, previous studies that investigated the association between ACS therapy and neonatal outcomes in twin pregnancies not only reported conflicting results but also lacked quantity.
A recent meta-analysis has reported that ACS therapy is associated with decreased neonatal death, respiratory distress syndrome (RDS) and IVH in singleton pregnancies, but not in multiple pregnancies.4 Furthermore, a randomised controlled trial on 311 twin infants who were delivered before 34 weeks of gestation showed that ACS therapy had no association with RDS or composite neonatal morbidity.23 However, large population-based cohort studies from the mid-2000s reported positive ACS effects in multiple pregnancies.24–26 A study of 750 twin infants from France has reported that a complete course of ACS therapy administered within 7 days before birth is associated with decreased rates of brain injury and mortality.24 Another study of 8274 multiplets from Italian Neonatal Network reported that ACS therapy reduced the risk of severe IVH and mortality, although it was less effective in multiple pregnancies than in singleton pregnancies.25 A study of 2516 twin infants from Canadian Neonatal Network has reported that twins can benefit from a complete course of ACS therapy as good as singletons in short-term respiratory morbidity, severe brain injury and mortality.26 Consistent with results of these large cohort studies, our study, using the latest data from KNN, revealed that the effectiveness of ACS therapy in twins was comparable with that of singletons. Moreover, its benefits on mortality and morbidity were shown to be different by gestational age groups.
Additionally, we found that twins had a higher rate of morbidity than singletons in this study. Twins were associated with higher risks of high-grade IVH and advanced ROP in infants born at 23–28 weeks of gestation and PVL in infants born at 29–33 weeks of gestation than singletons. Although twins are more likely to be delivered preterm than singletons, whether twin pregnancy alone has such adverse effects on neonatal outcomes in preterm infants remains unknown.27 In a large study of infants born between 23 and 35 weeks of gestation, twins and singletons had comparable average birth weights up to 32 weeks of gestation and similar neonatal outcomes.28 One study from Australian and New Zealand Neonatal Network has found higher mortality, but not morbidities, in twins than in singletons.12 Furthermore, two national cohort studies have reported comparable risks for neonatal outcomes except for RDS between twins and singletons.29 30 However, a population-based European cohort study showed that twins had higher risk of mortality and high-grade IVH in infants born at 24–27 weeks of gestation.14 Other studies have revealed disparities in the rate of morbidity such as BPD and ROP between twins and singletons.8 31
Possible reasons for conflicting findings in twins include study design and changes in population characteristics over time.32 We found that twins had lower rates of antenatal complications such as maternal hypertension and chorioamnionitis, and higher rates of obstetric interventions, including IVF, ACS and caesarean section than singletons in both gestational age groups (online supplemental file 2). This trend has also been observed across other recent studies.12 33 The higher rate of IVF in twins reflects the current trend of childbirth in Korea.5 The reason for higher ACS exposure in twins is currently unclear. However, more medical attention for twin pregnancies might be one possible cause.34 One noteworthy result was that the caesarean section rate for twins born between 23 and 28 weeks of gestation was 87.2% in our study, which was higher than that in other countries. For similar gestational age, the caesarean section rate for twins was 74.4% in the USA and 61.8% in Australia and New Zealand.12 15
Supplemental material
Despite the fact that these differences in characteristics between twins and singletons are observed in other studies, an increase in the proportion of the population exposed to ACS along with variation in practice of neonatal care in each country might have complexly contributed to the interaction between ACS and plurality as well as the inherent risk of a twin pregnancy.35 Although we adjusted potential confounders which were different between twins and singletons in the analyses, different population characteristics between twins and singletons and/or between studies should be considered when interpreting our results.
Our study has several limitations. First, the KNN registry had no information about chorionicity in multiple pregnancies. Thus, we were unable to investigate the difference in the effect of ACS therapy on neonatal outcomes according to chorionicity in twins. Second, although we used prospective cohort data of preterm infants with VLBW for this study, antenatal information including ACS administration was collected retrospectively because preterm infants were enrolled after they were born. Therefore, it was unknown why ACS was not or incompletely administered in infants who did not receive a complete course of ACS therapy. Notably, the percentage of singletons without exposure to ACS was higher in this study than in other studies.36 37 Moreover, information on the total amount of ACS administered was not available in the KNN registry database. Information on total amount of ACS administered will enable a more quantitative analysis of effects of ACS therapy on neonatal outcomes. Lastly, in our cohort, 56.6% of twins were conceived via IVF whereas only 7.1% of singletons were conceived via IVF. Although preterm infants conceived via IVF are known to have comparable morbidity and mortality with their peers conceived via natural pregnancy,38 higher proportion of IVF cases among twins should be taken into account when interpreting our results.
Conclusion
Despite differences in demographic and clinical characteristics according to plurality, ACS therapy administered before birth had comparable positive effects on neonatal outcomes of preterm infants with VLBW regardless of plurality.
Data availability statement
Data are available upon reasonable request. The Korean Neonatal Network (KNN) Publication Ethics Policy adheres to the following research data management and access guidelines: all information about patients and participating NICUs is confidential and may be used by individuals for approved research purposes. If an individual or institution that is not affiliated with KNN wants to use the data, it must make an official request to the KNN publication-Ethics Committee and obtain approval from the network.
Ethics statements
Patient consent for publication
Ethics approval
Registration of data in the KNN was approved by the Institutional Review Board (IRB) of each participating centre. Informed consent was obtained from parents of each infant prior to participation in the KNN registry. This study was approved by the IRB of Seoul National University Bundang Hospital (approval number: B-1305-202-005).
Acknowledgments
This research was supported by a research grant (2019-ER7103-02#) funded by the Korea National Institute of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SPB—conceptualisation, methodology, investigation, writing (original draft preparation) and funding acquisition. W-HH—investigation and writing (review and editing). SP—formal analysis and visualisation. YHJ—data curation and writing (review and editing). JYP—writing (review and editing). KJO—writing (review and editing). CWC—conceptualisation, methodology, writing (review and editing) and supervision. CW is responsible for the overall content as the guarantor.
Funding This study was supported by Soonchunhyang University Research Fund (grant number 1021-0032) to cover publication cost.
Disclaimer The funder had no role in the study design, data collection, data analysis, data interpretation, writing of the report or the decision to submit the article for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.