Article Text

Abstract
Objective To describe the clinical and epidemiological characteristics of newborn infants with SARS-CoV-2 infection notified in the Colombian Public Health Surveillance System.
Design This epidemiological descriptive analysis was conducted using the data of all cases of newborn infants with confirmed SARS-CoV-2 infection notified in the surveillance system. Absolute frequencies and central tendency measures were calculated and a bivariate analysis comparing variables of interest with symptomatic and asymptomatic disease was performed.
Setting Population-based descriptive analysis.
Patients Laboratory-confirmed COVID-19 cases in newborn infants (aged ≤28 days of life) reported to the surveillance system from 1 March 2020 to 28 February 2021.
Results 879 newborns were identified, corresponding to 0.04% of all reported cases in the country. The mean age at diagnosis was 13 days (range 0–28 days), 55.1% were male and most (57.6%) were classified as symptomatic. Preterm birth and low birth weight were identified in 24.0% and 24.4% of the cases, respectively. Common symptoms were fever (58.3%), cough (48.3%) and respiratory distress (34.9%). A higher prevalence of symptomatic newborns was seen in individuals with low birth weight for gestational age (prevalence ratio (PR): 1.51, 95% CI: 1.44 to 1.59) and newborns with underlying conditions (PR: 1.33, 95% CI: 1.13 to 1.55).
Conclusions There were a low proportion of confirmed COVID-19 cases in the newborn population. A substantial number of newborns were classified as symptomatic, having low birth weight and being preterm. Clinicians caring for COVID-19-infected newborns should be aware of population characteristics that potentially contribute to disease manifestations and severity.
- COVID-19
- mortality
- epidemiology
- neonatology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Paediatric SARS-CoV-2 infection has shown a lower proportion of disease severity and mortality when compared with adults. Within the paediatric population, children with underlying medical conditions and infants younger than one year of age present with the highest disease burden.
WHAT THIS STUDY ADDS
A low proportion of newborn infants were reported to the Colombian National Surveillance System. Children living in socially and economically deprived environments showed higher frequencies of infection. Clinical variables such as low birth weight and underlying medical conditions were associated with an increased prevalence of symptomatic disease.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Population social and economic characteristics should be taken into account when allocating resources in the context of health emergencies. Specific clinical characteristics in newborn infants with SARS-CoV-2 infection can potentially contribute to disease manifestations and severity.
Background
The severe acute respiratory syndrome coronavirus -2 (SARS-CoV-2) is the aetiological agent of the COVID-19 and was first identified in December 2019. Since its recognition, SARS-CoV-2 showed a rapid spread and on 11 March 2020, the WHO declared the COVID-19 outbreak as a pandemic.1
During the first pandemic year (March 2020–February 2021), the world reported more than 160 million confirmed cases and 3 million deaths that primarily concentrated in the population older than 80 years of age.2 During this period, Colombia confirmed 2 342 278 SARS-CoV-2 cases of which 153 344 were children under 18 years of age.3 Disease incidence and mortality concentrated in adults, with fewer cases affecting children and adolescents, but with considerable numbers to merit adequate analysis.
Younger populations, especially those under 18, have carried a milder disease burden, with decreased severity and mortality. Most COVID-19 cases in the paediatric population fall within the asymptomatic (20%) or mild categories (33%–42.5%).4 5 Severe illness tends to be more frequent in children under 1 year of age compared with other paediatric age groups (14% vs 5%).6 Intensive care unit admission and mortality due to SARS-CoV-2 infection has been reported in 2% and 0.08%, respectively, in a large cohort of infected children.5 Multisystem inflammatory syndrome in children has been a clinical feature that complicates paediatric SARS-CoV-2 infection, being more frequent in school-aged males, increasing paediatric morbidity and mortality related to this infection.7
As a more severe spectrum of the disease seems to concentrate in infants younger than 1 year of age when compared with older paediatric age groups, understanding disease dynamics in highly vulnerable populations, such as newborns is essential. Neonatal SARS-CoV-2 infection is uncommon and mainly occurs in the context of an infected caregiver transmitting the disease to the newborn infant.5 Congenital and intrapartum SARS-CoV-2 transmission has been reported, although the rate, risk and likelihood of this transmission are currently under research.8 When an infection in the neonate occurs, mild disease is the most frequent presentation (48%).5 The most common reported symptoms are dyspnoea, fever and feeding intolerance. Critical disease has been reported to be as high as 12%, which is higher than reported for other paediatric age groups.5
In this report, we sought to describe the population of live-born newborns with laboratory-confirmed SARS-COV-2 infection that were included in the Colombian COVID-19 surveillance system from March 2020 to February 2021. Population and disease characteristics are described, and factors related to developing symptomatic disease are explored.
Methods
SARS-CoV-2 National Surveillance Programme
Within the SARS-CoV-2 National Surveillance System (led by the Instituto Nacional de Salud (INS)), any symptomatic individual for respiratory disease and its close contacts (regardless of symptom presentation) would be tested for SARS-CoV-2. SARS-CoV-2 screening was also performed for patients who needed hospitalisation regardless of symptom status. Any individual with a positive SARS-CoV-2 test (either RT-PCR or antigen test) would be notified to the surveillance system where epidemiological and clinical information was uploaded to the system.
A descriptive-analytical cross-sectional study was then carried out that included all newborn infants with a positive SARS-CoV-2 test, who were either tested for having symptomatic disease, being a close contact to a positive individual or screened for SARS-COV-2 if needing hospital admission, from 1 March 2020 to 28 February 2021. The newborn population was defined as a live-born infant ≤28 days of life. Adjusted age for preterm infants was not considered. Parental infectious status was not routinely registered in the notification forms and was thus unknown for most cases in this analysis. Relevant demographic and clinical information from newborn infants were abstracted from the notification forms, including infant sex, ethnic group (Native/Indigenous, Afro-Colombian, no ethnic differentiation), socioeconomic stratum (low, medium, high), underlying medical conditions, the timing of symptom onset (first 48 hours of life or after 48 hours of life), age (in days) of SARS-CoV-2 diagnosis, SARS-CoV-2 clinical features, gestational age (GA) at birth, birth weight (median and birth weight category <2500 g and ≥2500 g), need for in-patient care and outcome (dead or alive). Birthweight percentiles for GA and sex were calculated using Fenton growth charts,9 low birth weight for GA was defined as weight ≤10th percentile for GA and sex. In addition, information regarding clinical characteristics of mortality cases in newborns was included.
SARS-CoV-2 genomic surveillance
Since 2020, the INS has performed SARS-CoV-2 genomic surveillance. The spatiotemporal distribution of SARS-CoV-2 lineages circulating in Colombia between March 2020 and February 2021 was determined following the National Programme for the Genomic Characterisation of SARS-CoV-2 based on representativeness and virological criteria for probabilistic sampling.10 Sequences and metadata from the Global Initiative on Sharing Avian Influenza Data for SARS-CoV-2 were obtained, and samples were processed by the National Genomic Characterisation Programme for SARS-CoV-2 in Colombia using Oxford Nanopore Technology.11 The sequence lineage was estimated with Pangolin.12 Other sequence information, such as insertions and deletions (INDELs), single nucleotide polymorphisms (SNPs), Clade and Lineage, was obtained using NextClade.13
Data analysis
A database was constructed including information captured via the national notification forms. Absolute frequencies and central tendency measures were calculated for demographic and clinical variables. A SARS-CoV-2 epidemic curve for the newborn population was constructed; the registered date of case notification was included, as well as the prevalence of circulating SARS-CoV-2 variants in the country. The ratio of SARS-CoV-2 infection in neonates was calculated; the denominators for calculating the prevalence correspond to live births in 2020 reported by the National Administrative Department of Statistics. Finally, a bivariate analysis compared variables of interest (VOI) between the symptomatic and asymptomatic disease groups.
Patient and public involvement
Patient and public involvement was not included in this research as data used in the analysis comes from secondary sources, which originate from Public Health Surveillance activities embedded within national health policy interventions.
Results
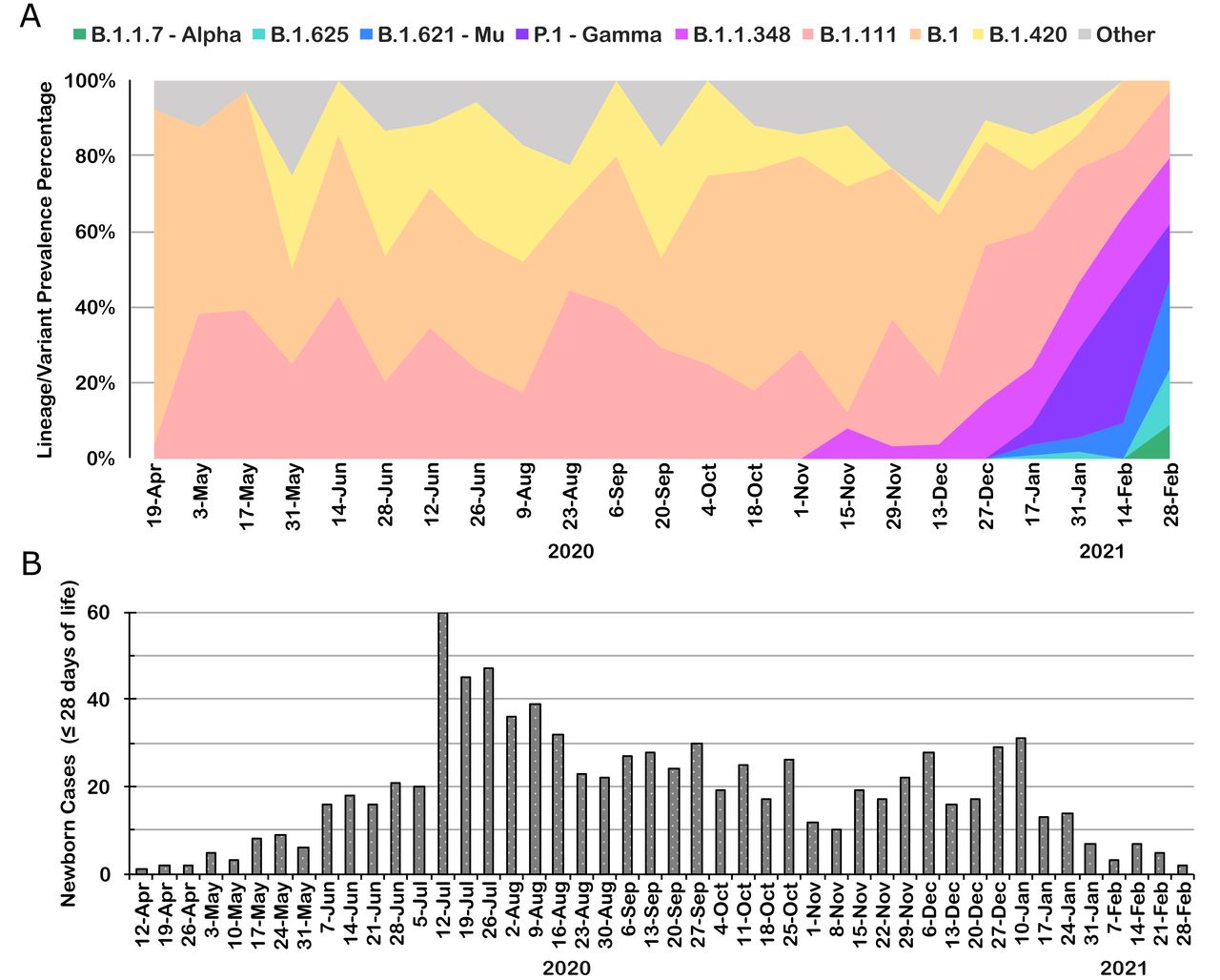
From 1 March 2020 to 28 February 2021, the Public Health Surveillance System reported 2 119 272 confirmed cases of SARS-CoV-2 in Colombia, of which 153 344 (7.2%) were paediatric cases (aged under 18 years) and 879 (0.04%) were newborn infants. The highest number of confirmed SARS-CoV-2 cases in newborns was seen on 11 July 2020, with 23 cases (figure 1B). During this period, B.1, B.1.420 and B.1.111 were the most prevalent variants circulating in Colombia (figure 1A).

(A) SARS-CoV-2 lineage prevalence during the first pandemic year in Colombia—March 2020 to February 2021. (B) confirmed SARS-CoV-2 cases in newborn infants (≤28 days of life) during the first pandemic year in Colombia—March 2020 to February 2021.
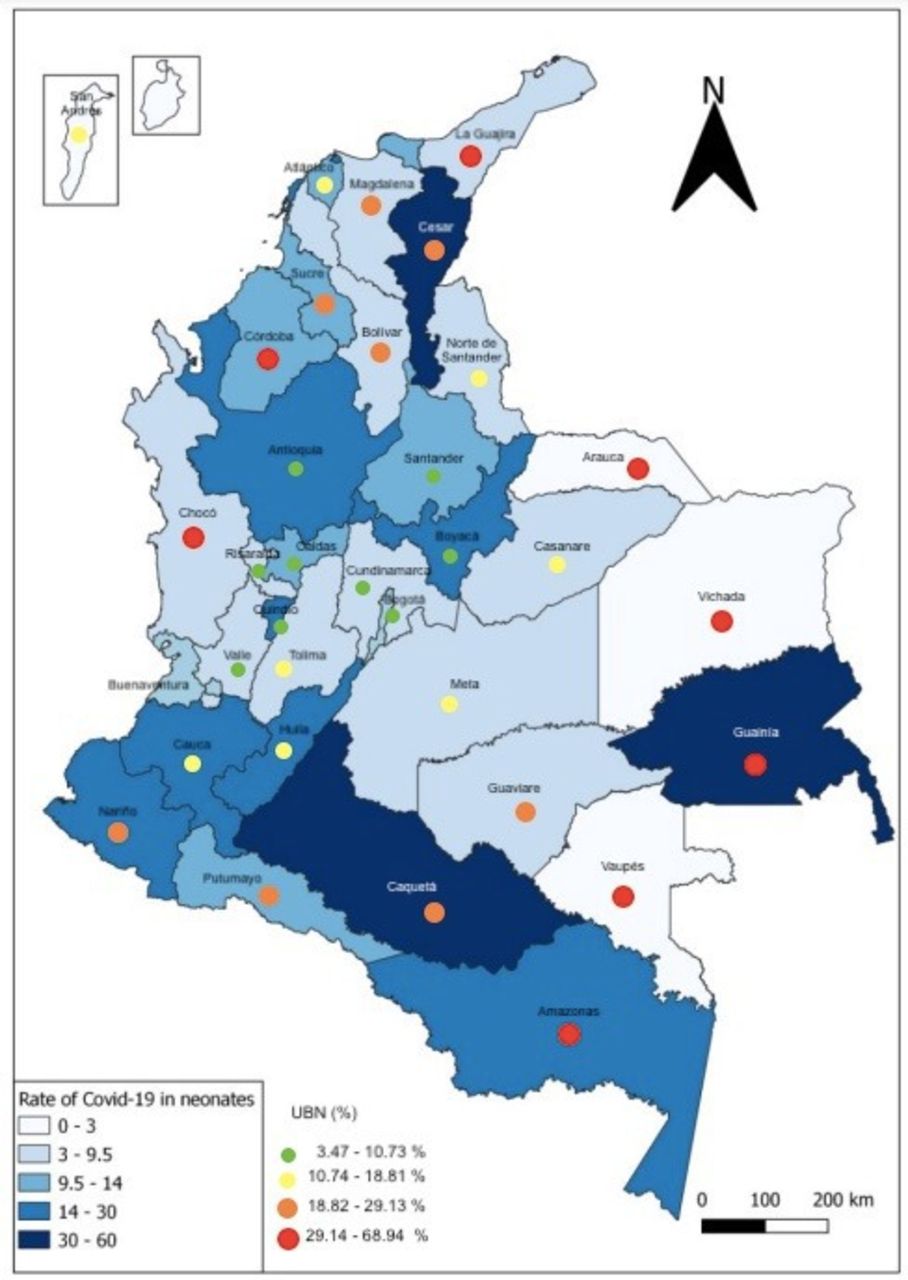
The rate of SARS-CoV-2 neonatal infection was estimated at 14.4 cases per 10 000 live births, 15.0 cases in males and 12.9 cases per 10 000 live births in females. The territorial entities with the highest rate per 10 000 live births were Guainía with 57.1 cases, Caquetá with 39.8 cases, Cesar with 34.5 and Bogotá with 26.2 cases per 10 000 live births (figure 2).
{kind=link}
{kind=link}
Rate of laboratory-confirmed SARS-CoV-2 cases in newborns (per 10 000 live births) during the first pandemic year—March 2020 to February 2021, and Unsatisfied Basic Needs (UBN) distribution in Colombian departments.
Regarding the socioeconomic characteristics, a higher proportion of cases was found in the lowest stratum, with 574 reported cases (65.3%) (table 1). The distribution by ethnicity is shown in table 1, with a higher proportion of cases in populations without ethnic differentiation (96.5%), followed by Afro-Colombian (2.2%) and Indigenous (1.1%).
Sociodemographic characteristics of Colombian newborns with confirmed SARS-CoV-2 infection
Population characteristics
Information regarding GA at birth and birth weight was available for a limited number of cases (27.4%). Of the cases with information on GA at birth, 75.9% were classified as term newborns, with a GA equal to or greater than 37 weeks. Among the preterm newborns with known GA (n=58, 24.0%), most (n=55) were between GA 28and 36 weeks (table 2). As for information regarding birth weight, the median weight for this population was 3020 g (range: 526–4225 g); 24.4% (n=59) of the population were classified as having low birth weight (<2500 g) (table 1).
Clinical characteristics of Colombian newborns with confirmed SARS-CoV-2 infection
Regarding the registry of underlying medical conditions, 67 infants (7.6%) were found to have one or more underlying conditions. The most frequently reported conditions were prematurity (n=65), followed by congenital heart disease (n=10) and birth defects (n=8) (table 1).
COVID-19 clinical features
The mean age at COVID-19 diagnosis was 13 days (range: 0–28 days) (table 2). In 27.3% of the cases (n=240), a close contact positive for SARS-CoV-2 was identified. In nine cases, the infection was considered to be early as the diagnosis was established during the first 48 hours of life (table 2). Of these nine cases, seven were receiving in-patient care at the moment of diagnosis, four were born prematurely and five had low birth weight; none had a known positive contact for COVID-19 (data not shown).
SARS-CoV-2 infection was classified as symptomatic in 57.6% of the cases (n=507). The most frequently reported symptoms were fever 58.3% (n=296), cough 41.6% (n=211) and respiratory distress 34.9% (n=177). The proportion of hospitalised and non-hospitalised cases at the time of notification was 48.4% (n=426)) and 51.5% (n=453), respectively, although the reason for hospitalisation or if the newborn was hospitalised for other causes when diagnosed with SARS-CoV-2 infection is unknown. When hospitalised, the median duration of inpatient care was 8 days (range: 0–66). Regarding outcome, 98.8% (n=869) were reported as alive, and 1.1% (n=10) were deceased.
Prevalence ratios (PRs) were calculated for symptomatic versus asymptomatic disease and selected clinical variables (table 3). A higher prevalence of symptomatic newborns was seen in individuals with low birth weight for GA (PR: 1.51, 95% CI: 1.44 to 1.59) and newborns with underlying conditions (PR: 1.33, 95% CI: 1.13 to 1.55). No differences were seen in variables such as sex or prematurity.
Bivariate analysis of selected clinical and demographic variables and SARS-CoV-2 case classification (symptomatic vs asymptomatic) in newborns with confirmed SARS-CoV-2 infection during the first pandemic year in Colombia—March 2020 to February 2021
Mortality cases
Among the 10 mortality cases registered in this cohort, only 2 were considered to be caused by SARS-CoV-2 infection.
One case was a male newborn of indigenous ethnicity. His mother had poor prenatal care, and thus, there was no record of any pregnancy complications. He was born at 37 weeks with low birth weight (2030 g) in a rural region in Colombia. At birth, the infant was admitted for inpatient care due to low birth weight and shared a hospital room with his mother. At 5 days of age, he presented with jaundice, respiratory symptoms and hypoxaemia, which evolved to multilobar pneumonia (requiring mechanical ventilation), sepsis, multiorgan failure and death at 11 days of age. A nasopharyngeal swab done at 6 days of age was positive for SARS-CoV-2 RT-PCR. A maternal nasopharyngeal swab taken at the same time revealed a positive result as well.
The second case was a male newborn, born at 36 weeks to a pregnancy complicated with severe pre-eclampsia. The infant’s birth weight was 2430 g and he was discharged home with his mother at 4 days of age. At 10 days of age, he was readmitted to the neonatal intensive care unit due to jaundice, poor feeding, and respiratory and neurological compromise. He was diagnosed with haemolytic disease due to blood group incompatibility (which responded to phototherapy) and multilobar pneumonia that progressed rapidly and required respiratory support. A nasopharyngeal swab taken at 14 days of life was positive for SARS-CoV-2 RT-PCR. He died at 21 days of age due to respiratory failure and sepsis. His mother and father were tested for SARS-CoV-2 RT-PCR both with positive results.
The other eight mortality cases were attributed to aetiologies other than SARS-CoV-2 infection, mainly sepsis, prematurity, birth defects and perinatal asphyxia.
Discussion
In this analysis, we describe the population of newborn infants with confirmed SARS-CoV-2 infection reported to the surveillance system during the first pandemic year in Colombia. During this year, the country reported 2 119 272 confirmed SARS-CoV-2 cases of which 7.2% were paediatric cases and 0.04% were newborns. This low proportion of paediatric and newborn populations within the reported cases is expected, as higher disease frequencies in adult populations have been consistently reported.14 In a publication that included 149 760 US SARS-CoV-2 cases, 1.7% were children under 18 years of age, of which 15% were infants younger than 1 year, but no distinction of the newborn population was made in this report.6 It is important to note that our analysis was performed when strict pandemic mitigating policies had been established, which could potentially impact the number of infections reported in the neonatal population.
Two peaks that occurred between June–August 2020 and November 2020–January 2021 marked Colombia’s first pandemic year. These peaks were dominated by the SARS-CoV-2 lineages B.1, B.1.111 and B.1.420, before the emergence of the VOI and concern (VOC),15 16 which were prevalent in the second pandemic year.3 To date, no strains have been associated with poorer outcomes in newborns, but pregnant women do seem to be more affected by the Alpha and Delta variants when compared with non-VOI/VOC strains.17 Most of the cases in this cohort were registered in the first peak, with a subsequent persistent decrease in the report of SARS-CoV-2 cases in newborn infants, even when other paediatric and adult age groups showed increased case notification. This behaviour could be reflecting a higher population compliance of preventive measures, especially when caring for vulnerable individuals like newborns.
The highest rates of SARS-CoV-2 infection in this cohort of newborns were seen in Colombian departments with high social and economic vulnerabilities and in newborns belonging to the lowest socioeconomic stratum. A previous SARS-CoV-2 seroprevalence study done in Colombian children and adolescents found that social and economic deprivations were correlated with higher risks of SARS-COV-2 exposure.18 Similarly, other authors have claimed that the pandemic has disproportionately affected economically and racially marginalised individuals, who have carried higher proportions of disease incidence and mortality.19–21 These findings should be considered when allocating efforts for SARS-CoV-2 prevention, testing and vaccination, advocating for an equitable distribution of resources.
Most of the newborn infants from this analysis were male (55.1%). Male newborns usually represent higher proportions when analysing newborn morbidity and mortality.22 23 Specifically, for COVID-19, a higher proportion of disease severity and mortality concentrates in the adult male population24 and some reports have found a higher proportion of male children in paediatric COVID-19 registries,6 including a small cohort of 17 newborns where 75% were male.5 No specific biological factors have been found to explain a higher susceptibility in male infants and children but these findings warrant further research.
Colombia usually reports a prevalence of prematurity between 10% and 12%,25 which is half of what was found in this analysis (24%). Preterm newborns tend to need in and outpatient care more frequently, posing higher exposures to healthcare and other facilities. This fact could potentially increase the risk of infection and the likelihood of being tested for SARS-CoV-2, both of these reasons could explain our high proportion of preterm infants. Also, SARS-CoV-2 infection during pregnancy increases the risk of preterm birth,26–28 and although no complete information on maternal infection was available for this analysis, maternal SARS-CoV-2 infection leading to premature birth and subsequently newborn exposure to an infected caregiver could be another potential explanation for our high proportion of preterm infants.
Most cases from this analysis were classified as symptomatic (57.6%) with fever and respiratory distress being the two most frequently reported symptoms. Although this finding could partially reflect a bias in favour of reporting symptomatic infants by the surveillance system, other authors have also found high proportions of symptomatic disease in the newborn population, being as high as 68%.5
The fact that a high proportion of our cases were hospitalised when diagnosed with SARS-CoV-2 infection, could to some extent reflect the high need for inpatient care of infected newborn infants. This finding could also be reflecting a higher SARS-CoV-2 testing rate for hospitalised infants. Also, as these cases belong to the first pandemic year where information regarding patient care for high risk populations was not readily available, it is possible that a lower threshold for deciding hospital admission was set for newborns, thus reflecting our high proportion of hospitalised patients.
In our results, a higher proportion of symptomatic disease was seen in infants classified as having low birth weight for GA and underlying conditions, which increased 1.4 and 1.3 times, respectively, the prevalence of having a symptomatic SARS-CoV-2 infection. In addition, other paediatric reports have found that children with comorbidities tend to have more severe clinical presentations of the disease and a higher frequency of hospitalisations, including intensive care unit admission.5 29 These findings underscore promoting disease prevention measures in highly vulnerable paediatric groups.
Only 2 out of 10 deaths were directly related to COVID-19 infection. Low mortality rates are usually reported in paediatric COVID-19 cohorts (0%–0.08%).4 5 Both cases had significant comorbidities emphasising their role in outcomes such as mortality. Also, both infants had caregivers with confirmed COVID-19 diagnoses, reflecting the risk of infection when exposed to close positive contacts. These findings may aid clinicians in adjusting isolation protocols when caring for high-risk newborns during epidemics and pandemics with SARS-CoV-2 and other similar virus-related infections.
Conclusions
The newborn population showed a low proportion of COVID-19 confirmed cases during the first pandemic year in Colombia. A substantial number of newborns in this cohort were classified as symptomatic, preterm and in need of inpatient care, potentially reflecting the higher healthcare needs in this specific population. Factors that pose higher vulnerabilities such as low birth weight and having underlying conditions seem to contribute to disease manifestations. Although mortality cases were low, clinicians caring for newborns should continue educating caregivers in performing adequate disease prevention measures for SARS-CoV-2 to mitigate adverse outcomes in newborns, especially those with pre-existing comorbidities.
Limitations
This study is subject to several limitations. As individuals were identified through the national surveillance system, it is more likely that newborns with symptomatic and more severe disease presentations were more frequently tested and notified to the system. Although the Public Health Surveillance System is of mandatory use across the country, it is possible that regions with restricted healthcare services to have lower notification rates. As information regarding COVID-19 cases was abstracted from notification forms, important clinical data are missing, which limit the comprehension of disease manifestations in this group of newborns. For example, information regarding the caregiver’s infectious status or maternal infection during pregnancy was not captured, leaving essential information about potential disease transmission unknown. In addition, as age adjustment for premature infants is not included in the notification forms, it is possible that infants outside the 28 days of life range but born prematurely and thus still considered newborn infants were left out of this analysis. As preterm infants and infants with underlying conditions tend to need more inpatient care following birth, it is possible that they were more likely to be tested for SARS-CoV-2 when compared with term and ‘healthy’ newborns, thus reflecting a high proportion of infants with these conditions.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This analysis was performed according to the ethical principles of the Declaration of Helsinki. Information comes from sources of data that were previously anonymised and do not represent a risk to individual privacy or the community. As data were abstracted from public use datasets, institutional Review Board approval and the use of informed consent were not deemed necessary as per national and institutional guidelines.30
Footnotes
Contributors Conceptualisation and methodology: MD, DF, GA and NR; Data analysis: DF, GA and NR; Data revision: MD, FP. Writing Original Draft: MD, DF, GA, NR and JO. Writing Review and Editing: MD, MM, FP, DW, AB, MB, MARD, OO, LM, SJ-BH and CG. Guarantor: MD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.