Article Text

Abstract
Background Norepinephrine (NE) is recommended for children and full-term neonates (born at >37 gestational weeks) with septic shock. Meanwhile, data on the effectiveness of NE in preterm neonates are still limited. This study aimed to evaluate the clinical efficacy of NE in preterm neonates with dopamine-resistant shock compared with that in full-term neonates.
Methods This was a single-centre, retrospective (January 2010–December 2020) cohort study of neonates with persistent shock despite adequate fluid resuscitation and dopamine or dobutamine administration at ≥10 μg/kg/min. Medical records of neonates treated with NE were retrospectively reviewed to collect respiratory and haemodynamic parameters and results of arterial blood gas (ABG) tests before and 8 hours after NE infusion. The effectiveness of NE was assessed using changes in clinical parameters and multiple regression models for mortality among subgroups of preterm and full-term neonates.
Results Ninety-two neonates (76% preterm) who received NE infusion were included in the study. NE infusion was started after a median of 7 hours (IQR 2–19 hours) after shock onset. Among the preterm neonates, the maximum dose of NE infusion was 0.5 (IQR 0.3–1.0) µg/kg/min with a median duration of 45 (IQR 24.0–84.5) hours. Haemodynamic dysfunction was ameliorated with increased blood pressure, decreased heart rate and improved ABG results. Preterm neonates with septic shock tended to have a reduced response to NE; however, preterm neonates with persistent pulmonary hypertension of the newborn tended to have a better response. Thirty-four (37%) neonates died in our cohort. The timing, dose and duration of NE use were not associated with neonatal mortality.
Conclusions Although using NE effectively improves clinical parameters in preterm neonates with dopamine-resistant shock, our study is underpowered to identify the association between NE infusion and mortality in preterm neonates with dopamine-resistant shock.
- Neonatology
- Resuscitation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Norepinephrine (NE) is recommended as the first-line vasoactive medicine for the management of septic shock in adults, children and full-term neonates.
Evidence of NE effectiveness in managing shock among preterm neonates is limited.
WHAT THIS STUDY ADDS
NE is similarly effective in preterm and full-term neonates with dopamine-resistant shock.
Preterm neonates with septic shock tended to have a reduced response to NE; however, preterm neonates with persistent pulmonary hypertension of the newborn tended to have a better response.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The present study provides initial evidence for future prospective investigations comparing NE to other commonly used vasoactive agents in the treatment of shock among preterm neonates.
Introduction
Shock is a critical condition characterised by impaired circulation and insufficient oxygen delivery to vital tissues, and it occurs commonly among neonates in newborn intensive care units (NICUs).1 2 Despite various causes of shock, prompt correction of circulation and tissue perfusion improves its prognosis.1 The treatment for neonatal shock commonly involves inotropes and vasopressors such as dopamine, dobutamine, milrinone, epinephrine and norepinephrine (NE).3 NE is recommended as the first-line vasoactive agent to treat septic shock in adults, children and full-term neonates (≥37 weeks of gestation at birth).4 5
There are controversies surrounding the most effective vasoactive agent for managing shock in preterm neonates. Dopamine has been suggested as the initial management of hypotension and is the most studied vasoactive medicine in neonatal shock.3 6–8 However, occasionally, high dopamine doses fail to sustain adequate tissue perfusion.9 In addition, previous studies in adults showed that dopamine administration might be associated with increased mortality in shock10 or similar outcomes but higher adverse events.11 Preterm neonates born less than 37 gestational weeks are often selected against NE because they are evidenced to present the following: (1) a higher catecholamine level, indicating a presumably weaker response to NE12 13; (2) increased risk of pulmonary hypertension after NE14; (3) an increased vascular resistance and decreased organ perfusion (previously reviewed15 16); and (4) risk of extravasation and skin injury with NE infusion.17 NE is currently used in less than 5% of preterm neonates with shock3 as a second-line or third-line treatment.18
Recent studies have suggested that the adverse events of NE are generally tolerated, and improved haemodynamics after NE can be observed in preterm neonates with septic shock or cardiovascular compromise.19 20 Nevertheless, there is insufficient evidence in the literature to support the clinical relevance regarding the effectiveness and safety of NE in preterm neonates with shock. In the current study on a retrospective cross-sectional cohort of preterm neonates with shock treated with NE, we aimed to summarise the response to NE in preterm neonatal shock and factors associated with mortality.
Methods
Study population
This retrospective study was undertaken in the NICU of Shanghai Children’s Hospital, China, to include neonates who received NE infusion to manage shock between 1 January 2010 and 31 December 2020. NE infusion was based on physician preference when shock persisted despite adequate fluid resuscitation and a high dose of dopamine or dobutamine (≥10 ug/kg/min). Full-term neonates (born after 37 weeks of gestation) were included as a comparison group during the study period.
Shock was defined as hypotension (mean blood pressure (MBP) <10th percentile of the normal range for birth weight (BW) and postnatal age)21 with at least three of the following criteria for impaired perfusion: (1) tachycardia (heart rate >160 beats/min), (2) abnormal peripheral pulses, (3) discolouration in the extremities, (4) prolonged capillary refill time of >3 s and (5) urine output of <1 mL/kg/hour.14 22 The neonates were further divided into shock subtype groups according to the following criteria: (1) septic shock: neonates with proven infection, symptoms highly suggesting infection, or laboratory tests showing a systemic inflammatory response (increased leucocyte count or C reactive protein, leucopenia <5×109, thrombocytopenia <80×109/L or procalcitonin ≥0.5 mg/L)23 24; (2) persistent pulmonary hypertension of the newborn (PPHN): neonates with labile hypoxaemia, differential cyanosis or echocardiogram-confirmed pulmonary hypertension.25 26
Treatment of shock
The newborns received NE through either a central catheter or peripheral venous access when a central venous catheter was unavailable,4 at an initial infusion rate between 0.2 µg/kg/min and 0.5 µg/kg/min. The rate of NE infusion was adjusted every 30 min until the MBP was normalised (>10th percentile of the normal range for BW and postnatal age). In the first 8 hours after NE infusion was initiated, no change in the dopamine/dobutamine infusion rate was performed; however, the neonates were weaned gradually from milrinone/epinephrine. The ventilator settings were adjusted to maintain peripheral capillary oxygen saturation between 90% and 94% during NE infusion.
Data collection
General clinical data were collected, including gestational age, BW, postnatal age of shock presentation, and mortality at hospital discharge. Ventilation parameters (fraction of inspired oxygen (FiO2), mean airway pressure, peak inspiratory pressure (PIP) and positive end-expiratory pressure), haemodynamics (heart rate, systolic blood pressure (SBP), MBP and urine output) and arterial blood gas (ABG) results (pH, pO2, pCO2 and base excess) were recorded before and 8 hours after NE infusion. Characteristics of NE infusion (time of initiation, maximal doses used, duration of infusion and adverse events related to disruption in NE infusion) were collected. During hospitalisation, intraventricular haemorrhage (IVH) was assessed by cranial ultrasound or cranial MRI and neurological examination. The effectiveness of NE is presented as an change in variables (ventilation parameters, haemodynamics, and ABG results) and was further evaluated using regression analysis to explore their association with mortality.
Statistical analysis
Data were analysed using R V.4.1.1 (www.r-project.org). The results are expressed as the median and IQR. Comparisons between groups were made using the Wilcoxon signed-rank test. Locally estimated scatterplot smoothing and linear regression models were used to display prematurity-related changes in clinical parameters after 8 hours of NE infusion. We conducted stepwise multivariate linear regression with mortality as the dependent variable to identify predictors significantly associated with neonatal death (R2 >0.2). A p value of less than 0.05 was considered statistically significant.
Results
General characteristics, NE infusion and response to NE infusion of neonates
Ninety-two neonates (among them, 70 were preterm) who received NE infusion were included in the study. Among these preterm neonates were 11 extremely preterm, 24 very preterm and 35 moderate to late preterm neonates. When comparing baseline characteristics with full-term neonates, preterm neonates presented a delayed shock onset (4.5 days after birth vs 0.6 days after birth in full-term neonates), prematurity-related complications (higher rate of IVH and NEC) and treatment features (lower rates of inhaled nitric oxide and extracorporeal membrane oxygenation), lower ventilation parameters (FiO2 and PIP) and increased urine output (table 1).
Demographics of preterm neonates with dopamine-resistant shock treated by norepinephrine
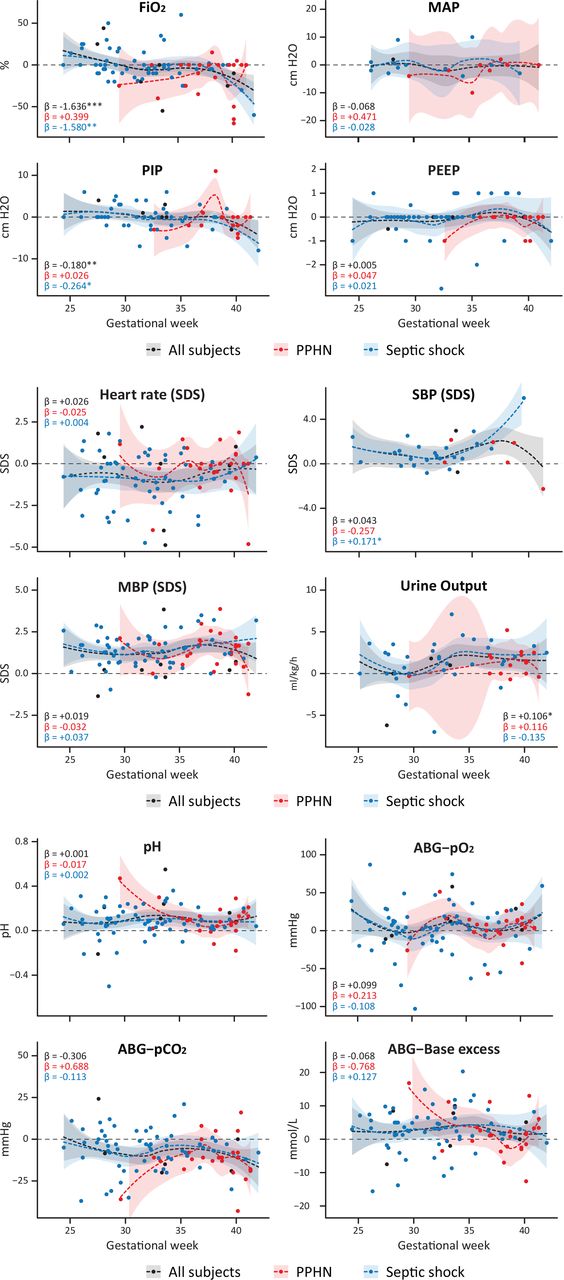
NE infusion was started at a median of 7 (IQR 2–19) hours after shock diagnosis. The dose of NE infusion was started at 0.2 (IQR 0.1–0.3) µg/kg/min to a maximum dose of 0.5 (IQR 0.3–1.0) µg/kg/min with a median duration of NE infusion of 45 (IQR 24–84.5) hours. Changes in clinical parameters (ventilation, haemodynamics and ABG results) before and 8 hours after NE infusion between preterm and full-term neonates are shown in table 2. While ventilation parameters were not improved, 8 hours of NE infusion ameliorated signs of haemodynamic dysfunction with decreased heart rate, increased blood pressure and improved ABG results (table 2). However, these changes were not statistically different between preterm and full-term neonates. In further comparisons among patients with shock subtypes, the duration of NE infusion was significantly longer in preterm neonates with PPHN, probably owing to better improvement (although insignificant) than in full-term neonates in our cohort (table 2). Although the comparison of changes in clinical parameters after NE infusion between preterm and full-term neonates in either shock subtype was not statistically significant (table 2), preterm neonates with septic shock had a significantly reduced response to NE in FiO2, PIP and SBP (figure 1); however, preterm neonates with PPHN tended to have a better response to NE in ventilation and ABG parameters (figure 1). No extravasation or skin injury was observed in any patients during NE infusion, and no interruption in NE infusion was recorded.
{kind=link}
Locally estimated scatterplot smoothing plot and β coefficient (significant level: *p<0.05, **p<0.01, ***p<0.001) of linear regression models of change in clinical parameters before and 8 hours after NE infusion in neonates with dopamine-resistant shock in all subjects (black), subjects with septic shock (blue) and PPHN (red). ABG, arterial blood gas; FiO2, fraction of inspired oxygen; MAP, mean airway pressure; MBP, mean blood pressure; NE, norepinephrine; PEEP, positive end-expiratory pressure; PIP, peak inspiratory pressure; PPHN, persistent pulmonary hypertension of the newborn; SBP, systolic blood pressure; SDS, SD score.
NE use and NE response in neonates with dopamine-resistant shock
Mortality
Among the 92 neonates, 34 (37%) died. The mortality rates of preterm and full-term neonates were 41% and 23%, respectively (table 1). Stepwise multivariate linear regression analysis showed that variables associated with neonates were primary factors of general characteristics (Apgar score and gestational week at birth), disease severity (treated with CRRT, epinephrine, and worse clinical parameters), and response to NE infusion (lower pCO2 and higher FiO2). However, the timing, duration and dose of NE infusion did not significantly contribute to neonatal mortality in our statistical models (table 3). Noteworthily, our data did not fit well in models of preterm neonates, especially in neonates with septic shock (R2=0.52–0.6), suggesting that other factors are involved in the survival of preterm neonates with septic shock (table 3).
Significant predictors of mortality in neonates treated with NE using stepwise multiple linear regression
Discussion
In this retrospective study of neonates receiving NE infusion due to dopamine-resistant shock, we identified that NE could mount similar improvements in haemodynamics in the general population of both preterm and full-term neonates. Premature neonates with septic shock had significantly less improved ventilation parameters after NE, whereas premature neonates with PPHN tended to respond better than full-term neonates after NE infusion. Our results suggest that mortality in our cohort is primarily associated with disease severity, rather than the infusion of NE or clinical response to NE.
Currently, there is minimal evidence on the safety and efficacy of NE in preterm neonates. No evidence supports the selection of NE over dopamine in managing shock in preterm neonates. However, an increasing body of evidence shows that NE can be effective in full-term neonates with septic shock refractory to fluid loading and dopamine or dobutamine,20 and full-term neonates with PPHN.14 In addition, NE can benefit preterm neonates with hypotension due to septic shock19 or pulmonary hypertension.14 Similar to these studies, our results showed that NE effectively improves clinical parameters in preterm and full-term neonates. Nevertheless, whether using NE could improve survival over other vasoactive medications in preterm neonates is yet to be elucidated. The mortality of preterm neonates treated with NE was high (33%–48%) in other studies14 19 and in our study (41%). The high mortality among these studies can be attributed to the selection of subjects with increased disease severity (failure to conventional treatment) and other confounding factors such as signs of poor prenatal care (lower rate of prenatal steroid use) and a higher rate of morbidities (IVH and NEC) when compared with general preterm neonates in China.27
NE is an endogenous catecholamine that acts primarily through the activation of α1 receptors to increase systemic vascular resistance. Preterm neonates have lower levels of NE immediately after birth than full-term neonates.28 29 While dopamine acts mainly through the release of NE from presynaptic vesicles, it’s effectiveness can succumb to the depletion of endogenous NE30 and an increased ratio of pulmonary and systemic artery pressure at high dopamine doses.31 This evidence supports the trial of NE in preterm neonates with compromised haemodynamics, especially when high-dose dopamine fails. Nevertheless, the various underlying aetiologies of shock (and different haemodynamic pathophysiologies) in preterm infants increase the complexity of vasoactive medication selection.32 In our study, although NE was similarly effective in improving clinical parameters in both preterm and full-term neonates, the trend was that NE might be less effective in premature infants with septic shock but more effective in premature infants with PPHN. This trend suggests aetiology-specific treatments in preterm neonates with shock is probably needed; however, it requires further confirmation as previous studies observed controversial effects of NE on ventilation parameters in preterm neonates with septic shock.19 20
Although improvements in haemodynamics are observed with NE infusion, our study is underpowered to detect the true clinical benefits of NE use in preterm neonates with dopamine-resistant shock. Our study is limited by its retrospective design with no predefined protocol to control bias and confounding factors such as shock aetiology, synergistic effect from changes in concomitant treatment along with NE infusion, imprecise methods of assessment (for instance, lack of haemodynamic index measures such as SVRI (systemic-vascular-resistance-index) and O2ER (Oxygen Extraction Ratio)) and data incompleteness. In addition, the relatively small sample size compromised the power to detect associations between the NE use and mortality outcome. Aside from the need for a common definition of shock in premature neonates, there are practical difficulties (for instance, in the acquisition of timely consent and measurement of clinical parameters) in recruiting preterm neonates in clinical trials.33 34 Although there are well-designed ongoing pilot studies endeavouring to establish a better definition of neonatal shock and pharmacokinetics of dopamine/dobutamine in preterm infants (NCT02047916 and NCT03311178) to initiate prospective studies (Neo-CIRC studies), the collection of data from prospective studies with comparative design between vasoactive medicines and predefined outcome measures among shock subtypes in preterm neonates can also be helpful to determine the benefit and risk of NE in preterm neonates at a lower cost.
Conclusions
NE effectively improves clinical parameters in preterm neonates with dopamine-resistant shock. Although NE might be less effective in premature infants with septic shock but more effective in premature infants with PPHN, our study is underpowered to identify the association between NE infusion and mortality in preterm neonates with dopamine-resistant shock.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Shanghai Children’s Hospital (2022R018-F02). The participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Qiu Gang, Cheng Cai (Shanghai Children’s Hospital) and Chengjun Sun (Children’s Hospital of Fudan University) for their valuable suggestions to the study.
References
Footnotes
Contributors XG and WH contributed to the conception and design of this study. PL, WH, YS and ZL contributed to the acquisition, analysis and interpretation of data. PL, ZL and WH drafted the manuscript and revised it critically. WH is acting as guarantor.
Funding This work was supported by Shanghai Children’s Hospital (numbers 2021YLYM11 and 2022YLYM08).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.