Article Text

Abstract
Objective Evaluating safety, feasibility and effects on physiological parameters of skin-to-skin contact (SSC) from birth between mothers and very preterm infants in a high-income setting.
Design Open-label randomised controlled trial.
Setting Three Norwegian neonatal units.
Patients Preterm infants at gestational age (GA) 280–316 weeks and birth weight >1000g delivered vaginally or by caesarean section (C-section).
Intervention Two hours of early SSC between the mother and the infant compared to standard care (SC) where the infant is separated from the mother and transferred to the neonatal unit in an incubator.
Results 108 infants (63% male, 57% C-section, mean (SD) GA 30.3 weeks (1.3) and birth weight 1437 g (260)) were included. Median (IQR) age at randomisation was 23 min (17–30). During the first 2 hours after randomisation, 4% (2 of 51) and 7% (4 of 57) were hypothermic (<36.0°C) in the SSC and SC group, respectively (p=0.68, OR 0.5, 95% CI 0.1 to 3.1). Significantly fewer infants in the SSC group had hyperthermia (>37.5°C) (26% (13 of 57) vs 47% (27 of 51), respectively, p=0.02, OR 0.4, 95% CI 0.2 to 0.9). No infant needed mechanical ventilation within the first 2 hours. Median (IQR) duration of SSC was 120 (80–120) min in the intervention group. There was no difference in heart rate, respiratory rate and oxygen saturation between groups during the first 24 hours.
Conclusion This study from a high-income setting confirmed that SSC from birth for very preterm infants was safe and feasible. Physiological parameters were not affected by the intervention. The long-term effects on neurodevelopment, maternal–infant bonding and maternal mental health will be collected.
Trial registration number NCT02024854.
- Neonatology
Data availability statement
Data sharing is not applicable for this study as data was collected before January 2019 and are not compatible with the Norwegian Health research act and privacy.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Early skin-to-skin care in the delivery room for very preterm infants has been shown to improve mother–infant bonding and improve survival in low-resource settings.
Immediate skin-to-skin contact in very preterm infants following delivery has shown improved cardiorespiratory stability.
Studies on early skin-to-skin care for preterm infants in high-income settings are scarce.
WHAT THIS STUDY ADDS
This study demonstrated that skin-to-skin contact between mothers and very preterm infants was feasible and safe both in the delivery and operating room.
Physiological parameters were similar in the groups receiving skin-to-skin contact and standard care.
Very preterm infants receiving skin-to-skin contact with the mother in the delivery room/operating room had better thermoregulation than infants who had standard care in an incubator.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Data from this study supports a change in clinical practice for very preterm infants in line with the recent WHO recommendations where skin-to-skin contact between the mother and infant should be initiated as soon as possible following birth.
Introduction
Skin-to-skin contact (SSC) or Kangaroo Mother Care between mothers and preterm infants is strongly recommended by the WHO,1 2 and has been shown to have positive effects on neonatal as well as maternal outcomes.3–8 The most recent Cochrane review7 supports SSC as an effective and safe alternative to standard care (SC), especially in resource-limited settings. A recent randomised controlled trial (RCT) of more than 3000 infants with a birth weight between 1.0 and 1.8 kg from Ghana, India, Malawi, Nigeria and Tanzania reported a reduction of mortality of 25% when SSC between the mother and infant was initiated shortly after delivery.6 However, research from high-income settings is scarce.
The availability of human and technical resources and drugs contributes to low mortality among preterm infants in high-income countries. It is unlikely that SSC after delivery in these settings influences mortality or major prematurity-related complications. However, parent–infant bonding,9 10 cardiorespiratory stability and breastfeeding11 12 may all improve with early SSC regardless of resources.11–14
Current delivery room practice for very preterm infants (gestational age (GA) 280–316 weeks) is to stabilise and place the infant in an incubator before transfer to the neonatal intensive care unit (NICU). After caesarean section (C-section), the mother and infant can be in separate departments for many hours. In one recent qualitative study, mothers who had their infants skin-to-skin described how they were immediately comforted by the infant’s vitality, while mothers who were separated from their infant described feelings of fear, guilt, and frustration.15 A study comparing 60 min delivery room SSC with 5 min of visual contact between mothers and infants born at GA 25–32 weeks, found an improved mother–child interaction at 6 months corrected age and less maternal depression in the SSC group.8
There has been a shift towards family oriented neonatal intensive care, and the family is now considered a central part of the NICU team.16 Whether this translates into improved long-term outcomes has not been established, but another intervention to enhance parental coping in the NICU has shown a significant increase in IQ points at five years of age.17
There is a need to identify barriers to early SSC for very preterm infants in high-resource settings as well as any harm or benefit. This study presents outcomes on feasibility, safety, and the effects on physiological parameters in very preterm infants randomised to early SSC in the delivery/operating room or SC in an incubator.18
Methods
Design
This was a prospective, open-label RCT comparing 2 hours of early SSC between mothers and very preterm infants with SC in an incubator following vaginal delivery or C-section.18 The study was initiated at St. Olavs Hospital, Trondheim University Hospital (Norway) in February 2014, and the protocol was published in 2016.18 Two additional Norwegian hospitals (Drammen hospital and Sørlandet hospital, Kristiansand) started recruiting infants in January 2017.
Participants
We included preterm infants born at GA 280–316 weeks with birth weight >1000 g. At one of the participating hospitals, twins were included and randomised to the same intervention, and at the other two hospitals, only singletons were included. Exclusion criteria were respiratory distress requiring more than 0.4 FiO2(fraction of inspired oxygen) to maintain oxygen saturation above 90% after 20 min of life, the need for intubation and mechanical ventilation in the delivery/operating room, major congenital malformations and maternal general anaesthesia.
The randomisation was conducted using sealed envelopes organised by the Unit for Applied Clinical Research at the Norwegian University of Science and Technology. Infants were stratified by centre, and GA (280–296 or 300–316 weeks) and randomly assigned to treatment group in a 1:1 ratio with block sizes of 4 and 6.
Intervention
Before delivery, eligible pregnant women (and their partner if available) received oral and written information about the study, followed by the giving of written consent. Following delivery, all eligible infants were placed on a prewarmed resuscitation unit (Giraffe OmniBed Incubator and warmer, Avante Health solutions) for initial assessment and stabilisation before randomisation (checkpoint 1, figure 1). Shortly after randomisation, the infants were either placed in a skin-to-skin position on the mother’s chest or transferred to the NICU in the incubator. Checkpoint 2 was completed after the infant was settled in a skin-to-skin position in the delivery/operating room or transferred to the NICU. Further details on the interventions are given in online supplemental. After a maximum SSC time of 2 hours, the infants were transferred to the NICU in an incubator.
Supplemental material

Flow chart of the procedure. BW, birth weight; GA, gestational age; NICU, neonatal intensive care unit, FiO2; fraction of inspired oxygen, ABC; airway, breathing and circulation.
Outcomes
The primary outcome was a neurodevelopmental outcome at 2 years corrected age which was evaluated using Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III)18 and will be published when completed. This paper describes the secondary outcomes from birth until discharge from the NICU including feasibility, safety, and physiological parameters during the first 24 hours. The main safety outcomes were the incidence of hypothermia (temperature <36°C) and the need for mechanical ventilation during the first 2 hours after randomisation. Other adverse events leading to a prolonged hospital stay were registered irrespective of the casual relationship with the study participation. The physiological parameters assessed were heart rate, respiratory rate and oxygen saturation. Physiological parameters were monitored continuously but collected at 15, 30, 60, 90 and 120 min, and then hourly.18
Patient and public involvement
Parents or the public were not directly involved in the design, conduct or plans for the dissemination of our research.
Sample size
Based on the primary outcome, a sample size of 136 infants was calculated as described elsewhere.18 Based on the number of very preterm births at the three Norwegian hospitals, the estimated sample size was expected to be achieved by the end of 2018. After 6.5 years, inclusion was stopped in October 2020 after the enrolment of 108 infants.
Statistical analysis
The data were analysed with the intention to treat. Demographic factors and clinical characteristics were summarised with counts (percentages) for categorical variables and means (SD) or medians (IQR) for continuous variables. The differences between the SSC and SC groups for continuous variables were analysed using two-sample t-tests or Mann-Whitney U-tests, and categorical variables using the Pearson χ2 test or Fisher’s exact test, as appropriate. P values <0.05 were considered statistically significant. The statistical analysis was conducted using IBM SPSS V.28 (IBM).
Results
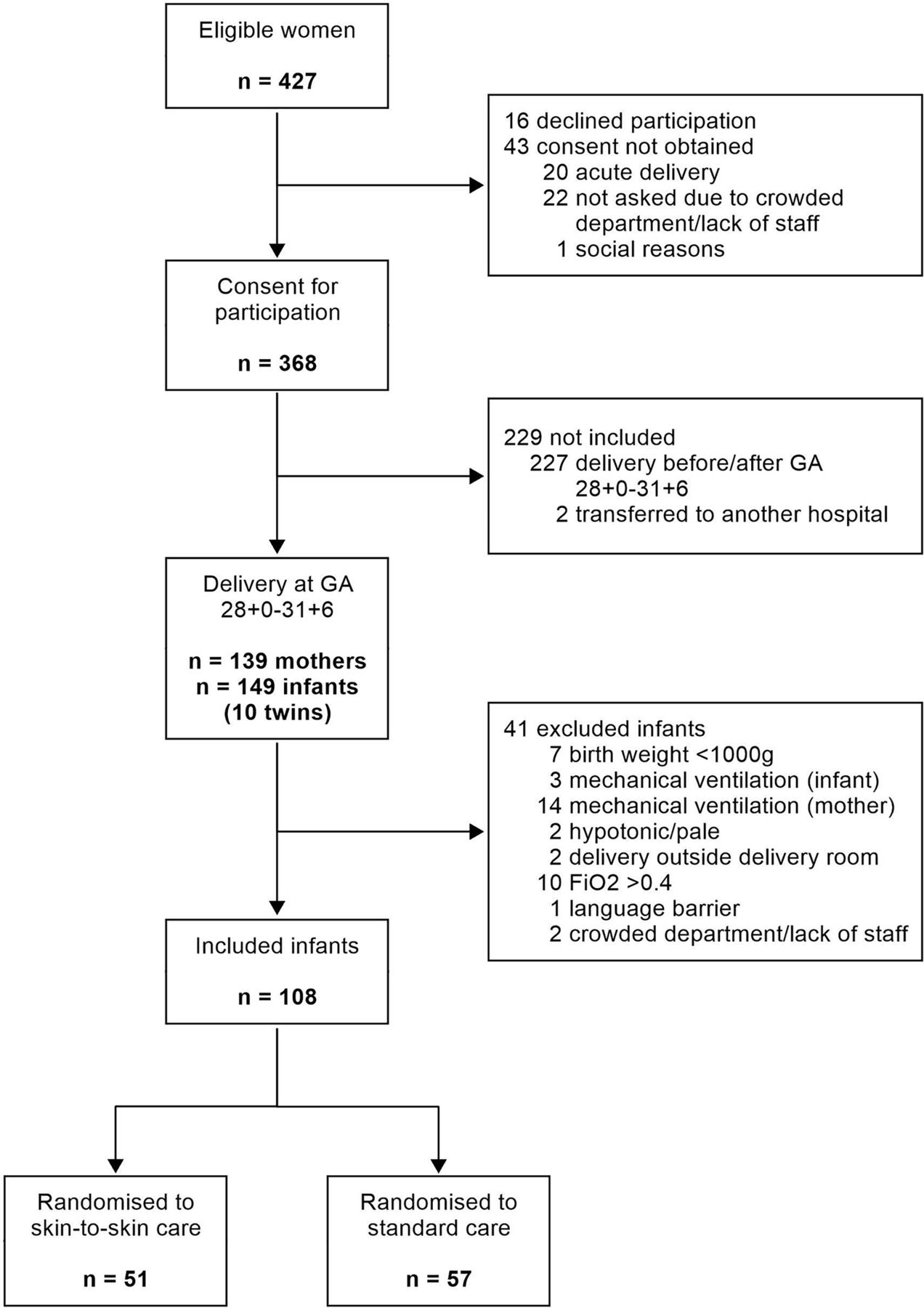
Of the 427 eligible women, 108 infants were included and randomly allocated to SSC (n=51) or SC (n=57) (figure 2). This included seven pairs of twins (four in the SSC group and three in the SC group). The majority (62%) of those who were not included despite consenting were delivered after 316 weeks of gestation. Twenty-two women were not asked for consent due to a crowded department and/or a shortage of staff.

Flow chart of study participants. G; gestational age, FiO2; fraction of inspired oxygen.
The demographic and neonatal characteristics are presented in table 1. Among infants randomised to SSC, the age at initiation of SSC did not differ between vaginal and caesarean delivery (median (IQR) 23 (17–30) min and 24 (20–28) min, respectively). The exact age in minutes at randomisation was missing for the first 23 infants (10 in SSC group and 13 in the SC group). However, data on whether infants randomised to SSC were placed in SSC at 30 min of age was available. Infants in the intervention group were in a skin-to-skin position for a median (IQR) of 120 (80–120) min. In 14 mother–infant pairs, SSC was interrupted before 2 hours. Four of these were due to the increased oxygen requirements of whom three received surfactant in the NICU (two with the INtubation-SURfactant-Extubation (INSURE) procedure at 60 and 90 min of age and one by less invasive surfactant administration (LISA) at 19 hours of age). In the remaining 10 cases with premature cessation of SSC, 8 had maternal causes (pain, pre-eclampsia, mother’s need to refresh or eat), 1 infant was moved from the mother to the father in the delivery room after 90 min and 1 infant was transferred to the NICU at 100 min of age for a central line insertion.
Demographics and neonatal characteristics according to intervention group
No infant needed mechanical ventilation during the first 2 hours after randomisation. There was a small difference in the incidence of hypothermia (<36.0°C) between the SSC and SC group (4% vs 7%, respectively; p=0.68, OR 0.5, 95% CI 0.1 to 3.1) (table 1). A smaller proportion of infants in the SSC group had hyperthermia (>37.5°C) during the first 2 hours after randomisation compared with the SC group (13 (26%) of 51 vs 27 (47%) of 57, respectively; p=0.02, OR 0.4, 95% CI 0.2 to 0.9). Five infants (all in the SC group) had at least one temperature >38.0°C, of which two had a temperature >38.5°C. The mean body temperature, heart rate, respiratory rate, oxygen saturation and supplemental oxygen in the two groups during the first 24 hours are shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
Line plot with mean (±1 SD) values during the first 24 hours in SSC versus SC-group: (A) body temperature (B) heart rate (C) respiratory rate (D) oxygen saturation (E) supplemental oxygen. SC, standard care; SSC, skin-to-skin contact.
Neonatal morbidities and outcomes during hospitalisation are shown in table 2. Twenty (18.5%) infants received surfactant in the first 24 hours of life, of whom two received surfactant by LISA in the delivery room before randomisation (one in each group).
Neonatal morbidities/outcomes during hospitalisation
More infants in the SSC group were discharged early to home care with a feeding tube (table 2).
Discussion
The main finding in this study is that early SSC initiated shortly after birth in the delivery or operating room is feasible and safe for very preterm infants born vaginally or by C-section. Physiological parameters during the first 24 hours of life were not improved by the treatment group, and neonatal morbidities during the NICU stay did not differ between groups.
Hypothermia is an important safety concern at preterm deliveries, but hyperthermia has received less attention. We found a higher occurrence of hyperthermia with SC than SSC which is in accordance with a similar study including infants born at 280–326 weeks of gestation.19 On the other hand, Mehler et al reported that infants receiving 1 hour of SSC with the mother in the delivery room compared with those receiving SC had a mean skin temperature at admission to NICU of 36.6°C vs 36.1°C, respectively.8 All these studies support the theory that early SSC is safe and does not compromise, but rather improves, thermoregulation in the preterm infant.
The safety of SSC was also supported by the fact that no infants needed mechanical ventilation during the first 2 hours. We could not offer early SSC for infants on mechanical ventilation because that would require a consultant to be present during the 2 hours in SSC. LISA was not foreseen in the study protocol, but the two infants who received LISA were clinically stable and could be randomised at 60 and 30 min of age in SC and SSC respectively.
Physiological parameters during the first 24 hours were not affected by the randomisation group in our study, and this is in accordance with Mehler et al.8 A recently published study reports improved cardiorespiratory stability in very preterm infants randomised to 6 hours SSC compared with SC after birth.11 However, subgroup analysis showed that this difference was only seen in one of the including centres, and the clinical relevance of the identified difference in SCRIP-score is also uncertain.
Based on our experience, it is feasible to offer SSC to more immature and fragile infants than those included in this study. It can be speculated that more fragile infants with less self-regulatory capacity may benefit even more from early SSC, but this has, to the best of our knowledge, not been studied. The time period for initial SSC in the delivery/operating room is also a question of resources and organisation of birth and neonatal units and may have to be individualised based on the severity of sickness. However, more mature infants who are spontaneously breathing with or without continuous positive airway pressure can probably be safely cared for in SSC for more than 2 hours as shown by Linnér et al.11
Facilitating SSC in the delivery and operating room required a redistribution of resources and extended cooperation between more healthcare professionals than usual. A recent paper underlines the importance of close collaboration between departments in order to prevent separation of infants and mothers from birth and throughout the hospital stay.20 This is also in accordance with the framework by WHO on holding health professionals accountable for facilitating a supportive environment at birth for preterm and low birthweight infants.21 More than 50% of infants in our study were born by C-section, and it is, therefore, important to include them both in clinical studies and practice.
This study was stopped prematurely after 6 years of recruitment. A majority of parents expressed a strong wish to hold and touch their infant as soon and as much as possible after delivery,15 and it became increasingly difficult for the staff to withhold early SSC. We find it unlikely that increasing the number of participants would have altered the results of this study, but the study may be underpowered for the primary outcome.
Interventions in the NICU should be evidence based, and any intervention must be proven safe and free from harm. However, questions may be raised about the level of evidence needed to offer interventions that are considered emotionally sound for healthy, full-term-born infants and their parents, as well as for preterm infants in an NICU environment. The experiences during the present study led to the implementation into clinical practice in two of the three participating units immediately after inclusion was stopped.
A limitation of the present study is that data on physiological parameters were collected intermittently and not continuously, and possible events between data collection may be unrecorded. Data on randomisation before 30 min after delivery was not reported in 23 cases, and this is reported as missing data. Registration of the total duration of SSC during hospital stay was not collected, and this would have strengthened the study. The multicentre design is a strength that gave us the opportunity to evaluate the implementation of SSC at three sites with different facilities and resources. This makes the results more generalised.
Conclusion
This study demonstrates that SSC for very preterm infants following delivery is safe and feasible both for vaginal and caesarean deliveries. Our results also suggest that SSC may improve infants’ thermoregulation. A non-separation strategy between the mother and infant from birth is recommended by the WHO,2 and this study supports such a change in clinical practice for very preterm infants.
Data availability statement
Data sharing is not applicable for this study as data was collected before January 2019 and are not compatible with the Norwegian Health research act and privacy.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Committee for Medical and Health Research Ethics in central Norway (2013/638/REK). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Thank you to the project group at NICU and the Delivery Department at St. Olavs Hospital, Sørlandet hospital, Kristiansand and Drammen Hospital for their invaluable contribution in the study. A special thanks to all the families included in the study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LK: project leader of the study. Contributed significantly to the study design, data management and collection, ethics considerations, and implementation strategies, and drafted the manuscript. RS: significantly contributed to the study design, development of the intervention, outcomes, sample size calculation, data collection and management. Substantive intellectual contribution in writing the manuscript. HB: significantly contributed to the study design, development of the intervention, outcomes, sample size calculation, data collection and management substantive intellectual contribution in writing, and supervision. KA: contributed significantly to statistical analysis and in writing the manuscript. HE and AB: contributed to implementation of the study and data collection. Participated in writing the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. LK is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.