
Abstract
Objectives
Our study aimed to assess differences in the susceptibility to severe acute illness in children with and without chronic health conditions treated in a pediatric intensive care unit (PICU).
Patients and methods
Data on age, gender, need for ventilator support, length of stay, as well as other parameters for the Paediatric Index of Mortality (PIM2) score were collected. Data were analyzed and compared across three patient groups: those with a neurodevelopmental disability, those with a chronic condition other than a neurodevelopmental disability, and those with no chronic condition. Reasons for admission of patients were classified according to the Australia and New Zealand Paediatric Intensive Care Registry (ANZPIC Registry) diagnostic codes. In the multidisciplinary, seven-bed, level I PICU of the Split University Hospital, the admission data were collected prospectively for 591 consecutively admitted patients aged ≤18 years.
Results
Patients with a neurodevelopmental disability had a significantly higher rate of respiratory-related admissions compared to patients with other chronic health conditions and those with no chronic condition (χ 2=33.72, P<0.001). There was a significant difference in the age at admission (f=6.04, P=0.003), median length of stay (f=7.94, P<0.001), need for ventilation during the first hour of admission (χ 2=14.74, P<0.001) and PICU mortality (χ2=9.91, P=0.007) of patients with neurodevelopmental disabilities, compared to the other two groups of patients.
Conclusion
Children with neurodevelopmental disabilities are more susceptible to acute illness compared to children with other chronic health conditions and those with no chronic condition.
Similar content being viewed by others


Introduction
Chronic health conditions are a significant cause of pediatric hospital admissions and contribute greatly to childhood morbidity and mortality. Children with chronic health conditions are hospitalized three times more often than children without chronic health conditions [14], and the majority of children who die in a hospital have at least one chronic health condition [7]. Children with chronic health conditions also form a significant fraction of children treated in pediatric intensive care units (PICU) [8, 17]. It is likely that there are several reasons for this. Chronically ill children may have an increased risk of severe acute illness [5], or PICU admissions may follow scheduled hospitalizations for the treatment of complications of the chronic illness [9]. We hypothesized that susceptibility to severe acute illness would differ between children with and without chronic health conditions, and therefore the present study aims to evaluate the influence of chronic health conditions on the susceptibility to acute severe illness.
Materials and methods
Split University Hospital is a public, university-affiliated hospital that serves a population of approximately 1,000,000 people from southern Croatia. The Pediatric Department has 120 beds, with an average of 3,100 admissions per year, and a separate neonatal ICU (NICU), where inborn patients are treated. The PICU is a seven-bed, multidisciplinary unit with three additional step-down beds, where children who need chronic ventilation are monitored (not included in the present study). The unit admits all children from newborns up to and including children 18 years of age. All medical and surgical (including trauma and burn) patients and newborns transported by “two-way transport” from outside of Split are admitted to the unit. Cardiac surgery is not available in the area serviced by Split hospital, and children with congenital heart diseases are transported to other centers. With the exception of extracorporeal membrane oxygenation, all other modes of management are available in the unit, including conventional ventilation, high-frequency oscillatory ventilation, NO therapy, peritoneal dialysis, venovenous hemodiafiltration, and invasive pressure monitoring. The unit is staffed by full time pediatric intensive care consultants and pediatricians of other subspecialties dedicated to intensive care.
Between June 2002 and July 2004, data were obtained prospectively from 591 consecutively admitted patients aged ≤18 years, but excluding preterm infants. Repeat admissions for an individual patient were considered as independent admissions. Chronic health conditions were defined as ongoing physical, developmental, behavioral, or emotional conditions that required health and related services of a type and amount in excess of that which is usually required by children [12]. Neurodevelopmental disabilities were defined according to the adaptation of Crocker’s categorization of developmental disabilities and mental retardation [4]. These disorders may result from genetic abnormalities, abnormalities of embryonic development or other antenatal or perinatal problems. However, in some patients, no underlying cause may be found [9].
The study protocol was approved by the Hospital’s Ethics Committee. Demographic data, such as age, gender, need for ventilator support and length of stay, were collected. Parameters for the determination of the Paediatric Index of Mortality (PIM2) score were recorded during the first hour of admission, and mortality risk for each patient was calculated according to the equations developed and published by the PIM Study Group [22]. Each patient’s principal reason for PICU admission was recorded as one of six diagnostic categories, in accordance with the Australia and New Zealand Paediatric Intensive Care Registry (ANZPIC Registry) of diagnostic codes [21].
The chi-squared test and ANOVA with the Tukey post-hoc test, together with Kruskal-Wallis test and Mann-Whitney test were used in statistical analysis, with results considered significant at 95% (P<0.05).
Results
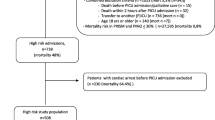
During the study period, 528 children accounted for 591 admissions to the PICU. Thirty-five children died in PICU. Since repeat admissions were considered as independent admissions, there were 248 (42%) patients with chronic health conditions and 343 (58%) patients with no chronic condition. Two admissions of children on long-term ventilation were not included in the study, since they stayed in the step-down unit. No noninvasive modes of ventilation were used in our patients.
For analysis, patients were divided into three groups: no chronic condition, neurodevelopmental disability, and other chronic condition. Table 1 lists the main reasons for PICU admission for each of the three groups. The most common reason for admission to the PICU for those with chronic illnesses (including neurodevelopmental disability) was a respiratory-related illness. However, patients with a neurodevelopmental disability had a significantly higher rate of respiratory-related admissions compared to patients of the other two groups.
Demographic and mortality data of the three groups of patients are shown in Table 2. The majority of admissions to PICU were unscheduled. Children with a chronic condition other than neurodevelopmental disability had a significantly higher percentage of elective admissions compared to children in the other two groups. The duration of PICU stay, number of patients ventilated during the first hour of admission, and observed PICU mortality were all significantly greater in patients with a neurodevelopmental disability compared with patients with other or no chronic condition. Patients with a neurodevelopmental disability were significantly younger at admission than other patients. Bronchopneumonia was the main cause of death.
Discussion
Children with chronic health conditions suffer a diverse range of illnesses. This means that the indications for hospitalization, the severity of their illnesses, the level of care they require, and the outcomes from treatment will vary among individuals.
Previous studies have reported different mortality rates for children with chronic neurodevelopmental disabilities. For example, Graham et al. reported a 3% mortality rate in patients with neurodevelopmental disabilities [9], whereas Glass and colleagues reported a 17% mortality rate for patients with chromosomal anomalies and mental retardation [8]. The variations in mortality rates are institutionally dependent, and reflect the differences among the populations of children treated, and the differences in specialties and procedures available at the different units. The majority of admissions from the study of Graham et al. were scheduled postsurgical admissions, whereas the majority of admissions in our study were unscheduled. The mortality of our patients with neurodevelpmental disabilities corresponds better with the survey of Dosa et al. where the mortality of patients with unscheduled admissions that were related to chronic diseases was 10.7% [5].
The evaluation of performance disclosed that the PIM2 scoring system was applicable for the whole population of our patients [13]. The PIM2-predicted mortality did not differ significantly among the three groups in this study. That lack of significance points to the consistency in application of the ICU admission criteria for all our patients. However, the observed mortality was significantly higher in patients with neurodevelopmental disabilities. The difference between the predicted and the observed mortality indicates the higher susceptibility for physiologic instability provoked by the acute insult in this group of children. The principal reason for this high susceptibility is likely the children’s inclination for overwhelming pulmonary infections. Respiratory problems reduce life expectancy and are the main cause of death in children with neurological impairment [16, 18]. They are multifactorial, numerous, and difficult to cope with [19]. Our patients with a neurodevelopmental disability were significantly more susceptible to severe respiratory illness than patients with other or no chronic disease. Moreover, bronchopneumonia was the commonest cause of death in this group. The significantly longer stay, the younger age at admission, and the greater need for mechanical ventilation compared with the other two groups, fit into the context of the observed morbidity pattern that is dependent on the neurological disability.
Our data set is relatively small, but it indicates that the course and the outcome of critical illness were associated with the existence and type of the underlying chronic condition of the studied groups of patients. Besides the broad range of health-related needs, the particularities and diversities of their needs make children with chronic diseases especially vulnerable [15, 20]. The needs of children with neurodevelopmental disabilities include additional complex services. A substantial proportion of these children are technology-dependent, and repeat admissions for this group at the PICU are more than likely [3, 5].
There were several limitations to our study. The studied population was relatively small. We did not perform a detailed diagnosis classification of our patients. The grade of the resource utilization for the three groups of patients was not evaluated. However, the demographic and mortality data of this study disclosed that patients with neurodevelopmental disabilities may be more endangered than patients with other or no chronic disease. An organized approach should be aimed at meeting the health-related needs and improving the general health of children with neurodevelopmental disabilities. That approach includes patient-oriented primary care, family support, access to specialty care, planning and monitoring home care, planning the use of emergency care services, and management of respiratory problems [1, 2, 6, 10, 11, 16]. The comprehensive application of these measures aids in reducing the development of life-threatening complications induced by an acute illness and protecting this susceptible population from unfavorable outcomes.
References
Ad Hoc Task Force on Home Care of Chronically Ill Infants and Children (1984) Guidelines for home care of infants, children and adolescents with chronic disease. Pediatrics 74:434–736
American Academy of Pediatrics, Medical Home Initiatives for Children With Special Needs Project Advisory Committee (2000) The medical home. Pediatrics 110:184–186
American Academy of Pediatrics, Johnson CP, Kastner TA, Committee/Section on Children With Disabilities (2005) Helping families raise children with special health care needs at home. Pediatrics 115:507–511
Crocker AC (1989) The causes of mental retardation. Pediatr Ann 18:623–629
Dosa NP, Boeing NM, Kanter RK (2001) Excess risk of severe acute illness in children with chronic health conditions. Pediatrics 107:499–504
Emergency Medical Services For Children, National Task Force on Children With Special Health Care Needs (1997) EMS for children: recommendations for coordinating care for children with special health care needs. Ann Emerg Med 30:274–280
Feudtner C, Christakis DA, Zimmerman FJ, Muldoon JH, Neff JM, Koepsell TD (2002) Characteristics of deaths occurring in children’s hospitals: implication for supportive care services. Pediatrics 109:887–892
Glass NL, Pollack MA, Ruttimann E (1986) Pediatric intensive care: who, why, and how much. Crit Care Med 14:222–226
Graham RJ, Dumas HM, O’Brien JE, Burns JP (2004) Congenital neurodevelopmental diagnoses and an intensive care unit: defining a population. Pediatr Crit Care Med 5:321–328
Jardine E, Wallis C (1998) Core guidelines for discharge home of the child on long term assisted ventilation in the United Kingdom. Thorax 53:762–767
Kuhlthau K, Nyman RM, Ferris TG, Beal AC, Perrin JM (2004) Correlates of use of specialty care. Pediatrics 113:E 294
McPherson M, Arango P, Fox H, Lauver C, McManus M, Newacheck P, Perrin J, Shonkoff JP, Strickland B (1989) A new definition of children with special health care needs. Pediatrics 102:137–140
Meštrovi J, Kardum G, Poli B, Omazi A, Stričevi L, Šusti A (2005) Applicability of the Australian and New Zealand Paediatric Intensive Care Registry diagnostic codes and Paediatric Index of Mortality 2 scoring system in a Croatian paediatric intensive care unit. Eur J Pediatr 164:783–784
Newacheck PW, Strickland B, Shonkoff JP, Perrin JM, McPherson M, McManus M, Lauver C, Fox H, Arango P (1998) An epidemiologic profile of children with special health care needs. Pediatrics 102:117–123
Perrin CE, Lewkowicz C, Young MH (2000) Shared vision: concordance among fathers, mothers, and pediatricians about unmet needs of children with chronic health conditions. Pediatrics 105:277–285
Plioplys AV, Kasnicka I, Lewis S, Moller D (1998) Survival rates among children with severe neurologic disabilities. South Med J 91:161–172
Randolph AG, Meert KL, O’Neil ME, Hanson JH, Luckett PM, Arnold JH, Gedeit RG, Cox PN, Roberts JS, Venkatarman ST, Forbes PW, Cheiftetz IM (2003) The feasibility of conducting clinical trials in infants and children with acute respiratory failure. Am J Respir Crit Care Med 167:1334–1340
Reddihough DS, Baikie G, Walstab JE (2001) Cerebral palsy in Victoria, Australia: mortality and causes of death. J Paediatr Child Health 37:183–186
Seddon PC, Khan Y (2003) Respiratory problems in children with neurological impairment. Arch Dis Child 88:75–78
Shatin D, Levin R, Ireys HT, Haller V (1998) Health care utilization by children with chronic illnesses: a comparison of Medicaid and employer-insured managed care. Pediatrics 102:E 44
Slater A, Shann F, McEnirey J (2003) The ANZPIC registry diagnostic codes: a system for coding reasons for admitting children to intensive care. Intensive Care Med 29:271–277
Slater A, Shann F, Pearson G (2003) PIM2: a revised version of the paediatric indeks of mortality. Intensive Care Med 29:278–285
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Meštrovi, J., Kardum, G., Poli, B. et al. The influence of chronic health conditions on susceptibility to severe acute illness of children treated in PICU. Eur J Pediatr 165, 526–529 (2006). https://doi.org/10.1007/s00431-006-0114-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-006-0114-3