
Abstract
Background
Fecal microbiota transplantation (FMT) has been demonstrated to be highly effective for the treatment of recurrent Clostridium difficile infection (CDI). However, the best route of administration has not been established. We present a pooled analysis of the reported cases of CDI treated with FMT via colonoscopy or nasogastric tube (NGT) to evaluate treatment efficacy.
Methods
PubMed was searched for English-written articles published up to December 2011. Studies that reported cases of FMT for recurrent CDI using either colonoscopy or NGT-guided fecal infusion were reviewed.
Results
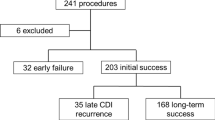
A total of 182 patients from 12 published studies were identified; 148 patients received FMT via colonoscopy (colonoscopy group) and 34 patients received FMT via NGT (NGT group). The median age in the colonoscopy group as compared with the NGT group was 72 and 82 years, respectively. There were differences regarding pre-FMT treatment for CDI; 134 patients (90.5 %, 134/148) received lavage with/without antibiotic in the colonoscopy group and 34 patients (100.0 %, 34/34) received antibiotic without lavage in the NGT group, P < 0.001. A higher stool volume was used for FMT in the colonoscopy group (121 patients, 81.8 %, used 100–400 ml) than in the NGT group (33 patients, 97.0 %, used <100 ml), P < 0.001. The treatment efficacy did not differ significantly; 93.2 % (138/148) success for the colonoscopy group as compared to 85.3 % success (29/34) for the NGT group, P = 0.162. Recurrence of CDI after FMT was also similar in both the colonoscopy group (8/148 5.4 %) versus the NGT group (2/34, 5.9 %), P = 1.000.
Conclusions
Despite procedural differences, FMT via colonoscopy or NGT appears to be highly effective and safe for the management of recurrent CDI.
Similar content being viewed by others

References
McMaster-Baxter NL, Musher DM. Clostridium difficile: recent epidemiologic findings and advances in therapy. Pharmacotherapy. 2007;27:1029–39.
Zilberberg MD, Shorr AF, Kollef MH. Increase in adult Clostridium difficile-related hospitalizations and case-fatality rate, United States, 2000–2005. Emerg Infect Dis. 2008;14:929–31.
Freeman J, Bauer MP, Baines SD, Corver J, Fawley WN, Goorhuis B, Kuijper EJ, Wilcox MH. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529–49.
Rupnik M, Wilcox MH, Gerding DN. Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat Rev Microbiol. 2009;7:526–36.
Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect. 1998;40:1–15.
Wenisch JM, Schmid D, Tucek G, Kuo HW, Allerberger F, Michl V, Tesik P, Laferl H, Wenisch C. A prospective cohort study on hospital mortality due to Clostridium difficile infection. Infection. 2012 Apr 17. [Epub ahead of print].
Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, Kelly C, Khoruts A, Louie T, Martinelli LP, Moore TA, Russell G, Surawicz C; Fecal Microbiota Transplantation Workgroup. Treating Clostridium difficile infection with fecal microbiota transplantation. Clin Gastroenterol Hepatol. 2011;9:1044–9.
McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol. 2002;97:1769–75.
Famularo G, Trinchieri V, De Simone C. Fecal bacteriotherapy or probiotics for the treatment of intestinal diseases? Am J Gastroenterol. 2001;96:2262–4.
Gough E, Shaikh H, Manges AR. Systematic review of intestinal microbiota transplantation (fecal bacteriotherapy) for recurrent Clostridium difficile infection. Clin Infect Dis. 2011;53:994–1002.
Liacouras CA, Piccoli DA. Whole-bowel irrigation as an adjunct to the treatment of chronic, relapsing Clostridium difficile colitis. J Clin Gastroenterol. 1996;22:186–9.
Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431–55.
Persky SE, Brandt LJ. Treatment of recurrent Clostridium difficile-associated diarrhea by administration of donated stool directly through a colonoscope. Am J Gastroenterol. 2000;95:3283–5.
Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficile colitis: case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clin Infect Dis. 2003;36:580–5.
Wettstein A, Borody TJ, Leis S, Chongnan J, Torres M, Hills LA. Fecal bacteriotherapy: an effective treatment for relapsing symptomatic Clostridium difficile infection. Gut. 2007;56:A303.
Hellemans R, Naegels S, Holvoet J. Fecal transplantation for recurrent Clostridium difficile colitis, an underused treatment modality. Acta Gastroenterol Belg. 2009;72:269–70.
MacConnachie AA, Fox R, Kennedy DR, Seaton RA. Faecal transplant for recurrent Clostridium difficile-associated diarrhoea: a UK case series. QJM. 2009;102:781–4.
Khoruts A, Dicksved J, Jansson JK, Sadowsky MJ. Changes in the composition of the human fecal microbiome after bacteriotherapy for recurrent Clostridium difficile-associated diarrhea. J Clin Gastroenterol. 2010;44:354–60.
Garborg K, Waagsbø B, Stallemo A, Matre J, Sundøy A. Results of faecal donor instillation therapy for recurrent Clostridium difficile-associated diarrhoea. Scand J Infect Dis. 2010;42:857–61.
Rohlke F, Surawicz CM, Stollman N. Fecal flora reconstitution for recurrent Clostridium difficile infection: results and methodology. J Clin Gastroenterol. 2010;44:567–70.
Yoon SS, Brandt LJ. Treatment of refractory/recurrent C. difficile-associated disease by donated stool transplanted via colonoscopy: a case series of 12 patients. J Clin Gastroenterol. 2010;44:562–6.
Duplessis CA, You D, Johnson M, Speziale A. Efficacious outcome employing fecal bacteriotherapy in severe Crohn’s colitis complicated by refractory Clostridium difficile infection. Infection. 2011 Dec 8. [Epub ahead of print].
Kelly CR, de Leon L, Jasutkar N. Fecal microbiota transplantation for relapsing Clostridium difficile infection in 26 patients: methodology and results. J Clin Gastroenterol. 2012;46:145–9.
Mattila E, Uusitalo-Seppälä R, Wuorela M, Lehtola L, Nurmi H, Ristikankare M, Moilanen V, Salminen K, Seppälä M, Mattila PS, Anttila VJ, Arkkila P. Fecal transplantation, through colonoscopy, is effective therapy for recurrent Clostridium difficile infection. Gastroenterology. 2012;142:490–6.
Rolfe RD, Helebian S, Finegold SM. Bacterial interference between Clostridium difficile and normal fecal flora. J Infect Dis. 1981;143:470–5.
Voth DE, Ballard JD. Clostridium difficile toxins: mechanism of action and role in disease. Clin Microbiol Rev. 2005;18:247–63.
Rao SS, Edwards CA, Austen CJ, Bruce C, Read NW. Impaired colonic fermentation of carbohydrate after ampicillin. Gastroenterology. 1988;94:928–32.
Grehan MJ, Borody TJ, Leis SM, Campbell J, Mitchell H, Wettstein A. Durable alteration of the colonic microbiota by the administration of donor fecal flora. J Clin Gastroenterol. 2010;44:551–61.
Brandt LJ, Reddy SS. Fecal microbiota transplantation for recurrent Clostridium difficile infection. J Clin Gastroenterol. 2011;45:S159–67.
McCarthy DM. Proton pump inhibitor use and Clostridium difficile colitis: cause or coincidence? J Clin Gastroenterol. 2012;46:350–3.
Hafner CD, Wylie JH Jr, Brush BE. Complications of gastrointestinal intubation. Arch Surg. 1961;83:147–60.
Kannan S, Morrow B, Furness G. Tension pneumothorax and pneumomediastinum after nasogastric tube insertion. Anaesthesia. 1999;54:1012–3.
Brandt LJ, Borody TJ, Campbell J. Endoscopic fecal microbiota transplantation: “first-line” treatment for severe Clostridium difficile infection? J Clin Gastroenterol. 2011;45:655–7.
Ko CW, Riffle S, Michaels L, Morris C, Holub J, Shapiro JA, Ciol MA, Kimmey MB, Seeff LC, Lieberman D. Serious complications within 30 days of screening and surveillance colonoscopy are uncommon. Clin Gastroenterol Hepatol. 2010;8:166–73.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Postigo, R., Kim, J.H. Colonoscopic versus nasogastric fecal transplantation for the treatment of Clostridium difficile infection: a review and pooled analysis. Infection 40, 643–648 (2012). https://doi.org/10.1007/s15010-012-0307-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-012-0307-9