
Abstract
Epidemiological studies have shown high rates of occurrence of arterial hypertension and type 2 diabetes mellitus among adults, and early preventive actions are extremely relevant for public policy strategies. The purpose of this study was to analyze the relationship between the prevalence of arterial hypertension and type 2 diabetes in adulthood and physical activity (currently and in childhood/adolescence). A retrospective study was carried out from March to November of 2009. Data were collected through interviews, and both diseases were assessed through self-report and confirmed by previous medical diagnosis. Current physical activity and that performed in childhood (7–10 years old) and adolescence (11–17 years old) were analyzed. Of the 1436 adults analyzed in this survey, ∼61% were women (n=881). Respondents' ages ranged from 18 to 94.8 years, and 20.2% of the total participants were ⩾65 years old. Our results show that men (18%) were more physically active than women (9.4%), whereas younger respondents and those with more formal education exhibited greater physical activity levels (P<0.001). Obese subjects presented lower physical activity levels (P=0.027). Physical activity in youth was associated with lower rates of occurrence of arterial hypertension (odds ratio (OR)=0.42 (95% confidence interval (CI)=0.29–0.62)) and type 2 diabetes mellitus (OR=0.29 (95% CI=0.15–0.56)) in adulthood, but current physical activity was not related to these outcomes. Our study reveals a positive relationship between early physical activity in both childhood and adolescence and lower rates of occurrence of endocrine and cardiovascular diseases in adulthood.
Similar content being viewed by others
Introduction
Epidemiological studies have shown high rates of occurrence of obesity, arterial hypertension and type 2 diabetes mellitus among the adult population.1, 2 Thus, effective protection against risk factors for endocrine and cardiovascular diseases is an important issue for public health policies.3 Evidence indicates that physically active individuals have more longevity with less morbidity and mortality. Indeed, physical exercise may prevent or reduce the deleterious effects of pathological conditions, such as arterial hypertension, type 2 diabetes mellitus and metabolic syndrome.4 Furthermore, it has been reported that cellular abnormalities associated with the development of these unhealthy outcomes in adulthood are initiated in early life.5 Accordingly, it has been shown that a higher level of physical activity is associated with lower blood pressure at rest in children.6 However, the relative influences of the levels of physical activity practiced currently and during youth on unhealthy outcomes in adulthood are unclear.
Thus, the purpose of our retrospective study was to analyze the relationship between the prevalence of arterial hypertension and type 2 diabetes mellitus in adulthood and physical activity currently and during youth.
Methods
Participants
This study was approved by the Review Board of the Institute of Bioscience of the Sao Paulo State University, and all participants provided written informed consent.
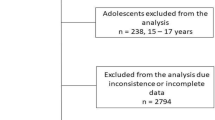
Our survey was carried out from March to November of 2009 in four cities: Rio Claro (191 886 inhabitants and a human development index of 0.825), Presidente Prudente (207 725 inhabitants and a human development index of 0.846), Bauru (359 429 inhabitants and a human development index of 0.825) and São Paulo (11 037 593 inhabitants and a human development index of 0.841) in the state of Sao Paulo (the most industrialized Brazilian state). Before beginning the study, two necessary sample sizes were estimated in consideration of the mean outcomes, and the higher one was adopted (arterial hypertension (n=749) with prevalence of 36%7 and type 2 diabetes mellitus (n=687) with prevalence of 29%;1 both estimated with a standard error of 4.5% and a significance of 5%). Both sample sizes granted a type I error rate of 5% and a power of 80%. Thus, considering a sample size of 749 and 10% loss, it was planned to interview a final sample of at least 824 participants. A multistage random process was carried out in the urban areas of each city, and three inclusion criteria were adopted: (i) age ⩾18 years, (ii) no chronic orthopedic complication (that is osteoporosis or osteomyelitis) and (iii) living in the current home for at least 2 years. After fieldwork, the final sample of interviewed adults totaled 1436 participants.
Self-reported data
Data were collected by interviews, and both diseases, arterial hypertension and type 2 diabetes mellitus, were assessed by self-report and confirmed by previous medical diagnosis. Body weight (kg) and height (m) were self-reported, and body mass index (BMI) was calculated as body weight divided by height squared and expressed in kg m−2. Schooling was categorized as 1–4 years, 5–8 years, 9–11 years or ⩾12 years. Smoking status (currently smoking or have either never smoked or smoked in the past) was also assessed. During the fieldwork, 23 subjects did not indicate their body weight; therefore, the analysis of nutritional status was carried out with 1413 subjects.
Current physical activity and physical activity during youth
Current physical activity levels were assessed by the Baecke questionnaire (section 2: sport activities in leisure time),8 on the basis of which each participant was defined as (i) inactive (no physical activity in leisure time); (ii) insufficiently physically active (subjects perform less than 180 min per week of physical activities of moderate to vigorous intensity or had performed 180 min per week of physical activities of moderate to vigorous intensity for less than 9 months); or (iii) physically active (subjects perform any physical activity of moderate to vigorous intensity for ⩾180 min per week and had done so for more than 9 months preceding the interview). In this assessment, we included both physical activities performed in leisure time (for example, walking and running) and fitness club activities (for example, running on a treadmill, aerobics or resistance training).
For assessment of physical activity in youth, childhood was defined as the period from 7 to 10 years of age and adolescence as the period from 11 to 17 years of age. Physical activity levels in both periods were assessed by two questions: ‘Outside the school, did you engage in any organized/supervised sporting activities for at least 1 year during the time you were 7–10 years old?’ and ‘Outside of school, did you engage in any organized/supervised sport activities for at least 1 year during the time you were 11–17 years old?’ Other physical activities, such as dance training, were also included. Thus, for all statistical analyses, a variable was created with three possible values: (i) None: if the participant responded ‘no’ to both questions; (ii) Either childhood or adolescence: if the participant responded ‘yes’ to just one question; and (iii) Both: if the participant responded ‘yes’ to both questions.
Validity and reproducibility of the self-reported data
Validity and reproducibility of the main outcomes were assessed previously. For reproducibility, 2 weeks after the first home interview, participants were reinterviewed by a different interviewer. The relationship between the BMI values reported in the two measurements was high (intraclass correlation=0.99; P=0.001). In addition, the kappa statistic (κ) was high for all categorical variables: arterial hypertension (κ=1.00; P=0.001), type 2 diabetes mellitus (κ=1.00; P=0.001), nutritional status (obesity presence: κ=0.86; P=0.001), physical activity in childhood (κ=1.00; P=0.001), physical activity in adolescence (κ=1.00; P=0.001) and current physical activity (⩾180 min per week: κ=1.00; P=0.001).
For assessment of the validity of reported values, during the second home interview, a subsample of participants were invited to participate in a direct measurement of fasting glucose, resting blood pressure and anthropometry. Of a total of 30 invitees, only 18 agreed to participate (15 men and 3 women; because of the low number of females, female participants were excluded from this analysis). The correlation between reported and measured BMI values was high (intraclass correlation=0.89 (0.72; 0.96); P=0.001). No subjects in this subgroup reported having type 2 diabetes mellitus; mean fasting glucose was 91.4 mg dl−1 (ranging from 81 to 130 mg dl−1), and only one subject presented fasting glucose ⩾100 mg dl−1. Approximately 93.4 % of the respondents reported correct health status.
Arterial hypertension was defined according to the guidelines of the Inter-American Society of Hypertension (starting at stage 1 with systolic blood pressure values ⩾140 mm Hg and/or diastolic blood pressure values ⩾90 mm Hg at rest). In this subsample, only one subject had previously self-reported arterial hypertension and, in the indirect measurement in the laboratory, presented systolic and diastolic blood pressure of 130 and 90 mm Hg, respectively, confirming the previous diagnosis. Excluding this hypertensive subject, mean diastolic blood pressure of the sample was 72.8 mm Hg (ranging from 50 to 82 mm Hg), and mean systolic blood pressure was 124.1 mm Hg (ranging from 107 to 142 mm Hg). Two subjects who had not previously self-reported arterial hypertension presented systolic blood pressure ⩾140 mm Hg in indirect measurement. Approximately 86.7% correctly self-reported their health status.
Statistical analysis
Numerical data were compared using the Student's t-test for independent samples. Categorical data were expressed as rates and compared by χ2-tests with Yates' correction in 2 × 2 tables and for linear trends. Binary logistic regressions were applied when χ2-test results were statistically significant. For assessment of the relationship between unhealthy outcomes in adulthood and physical activity (currently and during youth), a multivariate model for logistic regression was structured, in which potential confounders captured by the interviews (age, nutritional status, schooling, gender and smoking history) were inserted. Kappa statistics and intraclass correlations were used as indicators of agreement (categorical variables) and linear relationship (numerical), respectively. Significance (P) was indicated when P<0.05, and the statistical software SPSS (version 13.0) was used in all analyses.
Results
Of the 1436 adults analyzed in this survey, 61% were women (n=881) and 39% were men (n=555). In the overall sample, respondents' ages ranged from 18 to 94.8 years, with 20.2% of the total participants being ⩾65 years old (n=290). The mean age for women was 48.3±18.5 years and that for men was 45.8±191 years (P=0.012). Formal education of the sample studied was categorized as 1–4 years (24%), 5–8 years (15.5%), 9–11 years (38.6%) or ⩾12 years (21.9%). For participants with ⩾12 years of formal education, the percentage of men was significantly greater than that of women (25 vs. 20% of the overall sample, P=0.001).
Our results show that men were more physically active than women and younger participants with more formal education engaged in more physical activity. Obese and overweight subjects reported lower physical activity levels. The data are summarized in Table 1.
Arterial hypertension was self-reported by approximately 25.7% (95% CI=22.6–27.8%) of the studied population (n=369), and the percentages of men and women reporting arterial hypertension were statistically different (χ2-test; Figure 1d). Regarding type 2 diabetes mellitus, 8.9% (95% CI=7.1–10.4%) of the sample reported this endocrine metabolic disorder (n=128) and the percentages were similar between men and women. On the basis of the calculated BMI, approximately 33.9% (n=479) of individuals in the sample were overweight and 17.3% (n=244) were obese. To evaluate the influence of aging, BMI and schooling on the prevalence of arterial hypertension and type 2 diabetes mellitus, we analyzed the occurrence of both pathological conditions according to each parameter. Our data show that the prevalence of arterial hypertension and type 2 diabetes mellitus increases with advancing age (Figure 1a) and increasing BMI (Figure 1b). In contrast, the prevalence of both disorders decreases in subjects with the most formal education (Figure 1c).

Prevalence (%) of arterial hypertension and type 2 diabetes mellitus stratified by age (a), BMI (b), schooling (c) and gender (d).
Analyzing the physical activity practiced in youth, our data show that elderly subjects were less regularly engaged in sporting activities during childhood and adolescence compared with younger people in our studied population (Figure 2a). As expected, men were markedly more engaged in physical activity as youths compared with women (Figure 2b), and the highest level of formal education was positively associated with physical activity in both childhood and adolescence (Figure 2c). Obese and overweight participants had been less regularly engaged in sporting activities during childhood and adolescence compared with subjects with BMI <25 kg m−2 (Figure 2d).

Prevalence (%) of physical activity in youth according to age (a), gender (b), schooling (c) and BMI (d).
More engagement in physical activity during early life was associated with lower rates of both analyzed outcomes in adulthood (Figure 3a). Similarly, current physical activity meeting the guidelines for a health-promoting effect (>180 min per week of moderate to vigorous physical activity) was significantly associated with lower occurrence of arterial hypertension but was not associated with type 2 diabetes mellitus (Figure 3b).

Prevalence (%) of arterial hypertension and type 2 diabetes mellitus stratified by early physical activity (a) and current physical activity level (b). PAL=physical activity level.
Subjects who were physically active at the time of the study were more engaged in physical activities during childhood or adolescence (OR=1.64; 95% CI=1.03–2.60; P=0.035) or both (OR=2.35; 95% CI=1.67–3.32; P=0.001).
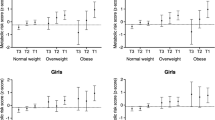
We also assessed the relationship between physical activity (currently and during youth) and occurrence of arterial hypertension and type 2 diabetes mellitus in adulthood. After adjustment for confounders (age, body weight status, schooling, gender and smoking), current physical activity was not significantly associated with both outcomes (Figure 4a for type 2 diabetes mellitus and panel b for arterial hypertension). However, physical activity during youth was associated with a lower occurrence of both arterial hypertension (panel d) and type 2 diabetes mellitus (panel c). These associations were more robust (smaller range in 95% CI) for arterial hypertension (OR=0.42; 95% CI=0.29–0.62) and type 2 diabetes mellitus (OR=0.29; 95% CI=0.15–0.56) when the adult was regularly engaged in physical activity in both childhood and adolescence.

Adjusted ORs and 95% CIs for relationships between current and early physical activity levels and occurrence of arterial hypertension (b, d, respectively) and type 2 diabetes mellitus (a, c, respectively). *=OR adjusted by gender, age, BMI, smoking history and schooling.
Discussion
This retrospective survey investigated the occurrence of endocrine and cardiovascular diseases in adults stratified according to physical activity during childhood and adolescence in a middle-income country. We found that physical activity during youth is a stronger predictor of these diseases in adulthood than is current physical activity.
Arterial hypertension is a highly prevalent chronic disease and the most common reversible risk factor for cardiovascular disease. Approximately 50% of coronary heart disease and 75% of stroke are due to higher than ideal blood pressure levels.9 The number of hypertensive persons worldwide in 2000 was estimated at 972 million, and by the year 2025, it is estimated that 1.56 billion persons will have hypertension.10 However, safe, effective and inexpensive options are available for the management of hypertension, such as changes in lifestyle.11 In fact, physical exercise of adequate intensity, duration and frequency improves cardiorespiratory fitness in healthy subjects, in addition to managing chronic diseases.12, 13
The prevalence of arterial hypertension and type 2 diabetes mellitus is estimated to be 29 and 9.3%, respectively, in the American adult population.1, 2 In our study, approximately 25.7 and 8.9% of adults reported arterial hypertension and type 2 diabetes mellitus, respectively, confirming the presence of elevated rates of both disorders in a Brazilian population obtained by self-report (that is, with a likelihood of underestimation). In agreement with our data, a recent survey indicated that the prevalence of arterial hypertension in a rural Chinese population increased from 20.4% in 1991 to 30.6% in 2007.14 These data reinforce the importance of preventive actions to control prevalence, as well as the risk factors associated with both pathological conditions, such as advancing age, dyslipidemia and rapid growth in the rates of overweight and obesity.
Regarding body weight status, our findings clearly show that current physical activity levels were lower in obese adults compared with those of normal body weight. In addition, a cross-sectional relationship was found between current physical activity level and the prevalence of arterial hypertension. One previous study has encouraged health-care professionals to recommend physical activity to ill subjects, and therefore our results could be affected by this reverse causality.15 It should be emphasized that in the assessment of current physical activity in our analysis, a previous period of engagement of at least 9 months in the reported activities was required to avoid bias. On the other hand, BMI was the most powerful confounder in the multivariate model, and when it was inserted into the analysis of current physical activity, the analyses did not yield a significant association of current physical activity with both outcomes.
Obesity has a relevant role in the genesis of arterial hypertension and type 2 diabetes mellitus, although the exact nature of this relation remains unclear. Several potential mechanisms have been linked to obesity, including greater sympathetic activity, endothelial dysfunction and increased plasma levels of angiotensin II, leptin, cortisol and insulin.16 In our study, obesity was associated with arterial hypertension and type 2 diabetes mellitus, supporting the findings of previous studies.7, 16 It is well documented that physical activity promotes improvement of vascular function, as well as increased insulin sensibility, showing the beneficial effects of physical activity on the prevention of cardiovascular and endocrine metabolic diseases.4, 17, 18 Recently, a study reported that a decline in fitness from childhood to adulthood was associated with insulin resistance in adulthood, suggesting that this outcome should be derived from a decline in physical activity, but this association was not analyzed directly as childhood physical activity was not assessed.19 In our study, we clearly show that physical activity performed during youth is positively associated with lower prevalence of arterial hypertension and type 2 diabetes mellitus in adulthood, indicating the importance of physical activity in the young population. The positive effect of early physical activity on these outcomes is likely due to the well-documented continuous endocrine metabolic stimulation, as well as because of hemodynamic changes in the organism in response to physical activity, which present characteristics of tracking.
One previous study failed to show a relationship between arterial hypertension in adulthood and early physical activity.20 Methodological differences may explain the discrepancy between that study and the present study. In our study, childhood and adolescence are considered both separately and in combination (with the variable combining both periods presenting the more restricted 95% CI for its OR), whereas in the other study, early physical activity was considered only during adolescence. Thus, our findings show that considering both childhood and adolescence makes the association more consistent than those made in an isolated manner. Moreover, our definition of childhood and adolescent physical activity required at least 12 months of practice, whereas the Reichert et al.20 study used a 6-month period.
Our study has strengths, such as the multistage random process used and the high level of reproducibility/validity, which grant internal validity. On the other hand, its limitations are related to the self-report of diseases, which can lead to underestimation of the analyzed outcomes. It is noteworthy that our data were similar to those obtained by previous studies, indicating that this underestimation, if it happened, was similar in all subgroups and did not affect the overall findings. The lack of control for BMI during childhood, which is an important potential confounder, should also be considered.
In conclusion, our study revealed a negative association between early physical activity—in both childhood and adolescence—and the occurrence of endocrine and cardiovascular diseases in adulthood. Our data reinforce the importance of preventing obesity and physical inactivity in childhood and adolescence as a primary focus of public policies.
References
Cowie CC, Rust KF, Byrd-Holt DD, Eberhardt MS, Flegal KM, Engelgau MM, Saydah SH, Williams DE, Geiss LS, Gregg EW . Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: national health and nutrition examination survey 1999–2002. Diabetes Care 2006; 29: 1263–1268.
Ong KL, Cheung BM, Man YB, Lau CP, Lam KS . Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension 2007; 49: 69–75.
Sichieri R, do Nascimento S, Coutinho W . The burden of hospitalization due to overweight and obesity in Brazil. Cad Saude Publica 2007; 23: 1721–1727.
Zanesco A, Antunes E . Effects of exercise training on the cardiovascular system: pharmacological approaches. Pharmacol Ther 2007; 114: 307–317.
Sinaiko A . Obesity, insulin resistance and the metabolic syndrome. J Pediatr (Rio J) 2007; 83: 3–4.
Leary SD, Ness AR, Smith GD, Mattocks C, Deere K, Blair SN, Riddoch C . Physical activity and blood pressure in childhood: findings from a population-based study. Hypertension 2008; 51: 92–98.
Jardim PC, Gondim Mdo R, Monego ET, Moreira HG, Vitorino PV, Souza WK, Scala LC . High blood pressure and some risk factors in a Brazilian capital. Arq Bras Cardiol 2007; 88: 452–457.
Baecke JA, Burema J, Frijters JE . A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 1982; 36: 936–942.
Kearney PM, Welton M, Reynolds K, Muntner P, Whelton PK, He J . Global burden of hypertension: analysis of worldwide data. Lancet. 2005; 365: 217–223.
World Health Organization. The World Health Report 2002. Reducing Risks, Promoting Healthy Life. World Health Organization: Geneva, Switzerland, 2002.
Hall JE . The kidney, hypertension, and obesity. Hypertension 2003; 41: 625–633.
Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK, American College of Sports Medicine. American college of sports medicine position stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 2009; 41: 459–471.
Blair SN, Cheng Y, Holder JS . Is physical activity or physical fitness more important in defining health benefits? Med Sci Sports Exerc 2001; 33: S379–S399.
Yang J, Lu F, Zhang C, Liu Z, Zhao Y, Gao F, Sun S, Zhao Y, Zhang Y . Prevalence of prehypertension and hypertension in a Chinese rural area from 1991 to 2007. Hypertens Res 2010; 33: 331–337.
Hallal PC, Azevedo MR, Reichert FF, Siqueira FV, Araújo CL, Victora CG . Who, when, and how much? Epidemiology of walking in a middle-income country. Am J Prev Med 2005; 28: 156–161.
Davy KP, Hall JE . Obesity and hypertension: two epidemics or one? Am J Physiol Regul Integr Comp Physiol 2004; 286: R803–R813.
Huang PL . eNOS, metabolic syndrome and cardiovascular disease. Trends Endocrinol Metab 2009; 20: 295–302.
Tousoulis D, Tsarpalis K, Cokkinos D, Stefanadis C . Effects of insulin resistance on endothelial function: possible mechanisms and clinical implications. Diabetes Obes Metab 2008; 10: 834–842.
Dwyer T, Magnussen CG, Schmidt MD, Ukoumunne OC, Ponsonby AL, Raitakari OT, Zimmet PZ, Blair SN, Thomson R, Cleland VJ, Venn A . Decline in physical fitness from childhood to adulthood associated with increased obesity and insulin resistance in adults. Diabetes Care 2009; 32: 683–687.
Reichert FF, Azevedo MR, Breier A, Gerage AM . Physical activity and prevalence of hypertension in a population-based sample of Brazilian adults and elderly. Prev Med 2009; 49: 200–204.
Acknowledgements
The authors are grateful to Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP) for financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Fernandes, R., Zanesco, A. Early physical activity promotes lower prevalence of chronic diseases in adulthood. Hypertens Res 33, 926–931 (2010). https://doi.org/10.1038/hr.2010.106
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2010.106
Keywords
This article is cited by
-
Physical activity and sedentary behaviour of adolescents and their parents: a specific analysis by sex and socioeconomic status
Archives of Public Health (2023)
-
Relationship between vigorous physical activity and health care costs among adolescents: ABCD Growth Study
BMC Pediatrics (2022)
-
Multimorbidity and leisure-time physical activity over the life course: a population-based birth cohort study
BMC Public Health (2021)
-
Sports Participation from Childhood to Adolescence is Associated with Lower Body Dissatisfaction in Boys—A Sex-Specific Analysis
Maternal and Child Health Journal (2021)
-
Young-onset type 2 diabetes mellitus — implications for morbidity and mortality
Nature Reviews Endocrinology (2020)
