Article Text

Abstract
Background: Head injuries related to bicycle use are common and can be serious. They can be prevented or reduced in severity with helmet use; however, education has resulted in modest helmet use in most developed countries. Helmet legislation has been proposed as a method to increase helmet wearing; while this social intervention is thought to be effective, no systematic review has been performed.
Objectives: This review evaluates the scientific evidence for helmet use following legislation to identify the effectiveness of legislative interventions to increase bicycle helmet use among all age groups.
Search strategy: Comprehensive searches of CENTRAL, MEDLINE, EMBASE, CINAHL, Web of Science, British Education Index, LILACS Database, TRIS (Transport Research Information Service), the grey literature, reference lists, and communication with authors was performed to identify eligible studies.
Selection criteria: Eligible studies for this review were community based investigations including cohort studies, controlled before-after studies, interrupted time series studies, non-equivalent control group studies
Data collection and analysis: Two reviewers extracted the data regarding the percentage of helmet use before and after legislation from each study. Individual and pooled odds ratios were calculated along with 95% confidence intervals.
Main results: Out of 86 prescreened articles, 25 were potentially relevant to the topic and 11 were finally included in the review. Of 11 studies, eight were published articles, two were published reports, and one was an unpublished article. One additional survey was incorporated following personal communication with the author. While the baseline rate of helmet use among these studies varied between 4% and 59%, after legislation this range changed to 37% and 91%. Helmet wearing proportions increased less than 10% in one study, 10–30% in four studies, and more than 30% in seven studies. While the effectiveness of bicycle helmet legislation varied (n = 11 studies; OR range: 1.2–22), all studies demonstrated higher proportions of helmet use following legislation, particularly when the law was targeted to a specific age group.
Conclusions: Legislation increased helmet use among cyclists, particularly younger age groups and those with low pre-intervention helmet wearing proportions. These results support legislative interventions in populations without helmet legislation.
- head protective devices
- bicycling
- legislation
- review
Statistics from Altmetric.com
Bicycling is a popular means of transportation, recreation, and exercise in many countries. However, injuries do occur and they can be severe. Head injuries are among the most severe injuries in cyclists comprising one third of emergency department visits and two thirds of bicycling deaths.1,2 Use of bicycle helmets can prevent or lessen the severity of brain injury during a bicycle crash. In a recently published Cochrane systematic review, Thompson et al provided evidence that bicycle helmets reduce the risk of head injury between 63% and 88%.3 The review also revealed that bicycle helmets provide equal protection for crashes involving motor vehicles (69%) and crashes from all other causes (68%).
Despite the enormous degree of protection afforded by a bicycle helmet, a 1994 US national telephone survey revealed that only 50% of bicyclists owned a helmet and only 25% reportedly always wear one when cycling.4 This condition did not improve until 1999, where the percentage of children who reported always using a helmet varied from 13% to 65%, depending on the state.5 In Sweden, during 14 years of follow up from 1988 to 2002, helmet use increased from 5% to 33% among school children and from 2% to 14% among adults.6 Helmet use increased from 10.7% to 31.1% among school children from 1988 to 1991 in Ottawa, Canada.7
Although educational programs, promotional campaigns, and community incentives have been used to increase bicycle helmet use,8,9,10,11,12 many jurisdictions decided to make helmet wearing mandatory for children and adolescents in the early 1990s. In the following years, many researchers tried to examine the effectiveness of bicycle helmet legislation in increasing helmet use among children and adults.13–23 While this intervention has been shown to be effective by studies in selected jurisdictions, no systematic review covering the complete published literature has been performed.
The objective of this review was to identify the effectiveness of bicycle helmet legislation to increase bicycle helmet use among all age groups.
METHODS
Inclusion criteria
Included studies were required to be community based and one of these design types: cohort studies, controlled before-after studies, interrupted time series studies, or non-equivalent control group studies. Studies involving children, adolescents, and/or adults of both genders observed while cycling for any purpose in any location within a defined community were considered. We included those studies with introduction of bicycle helmet wearing legislation at the regional, state/province-wide, or municipal level, compared with a pre-, non-legislative period in the same community or a matched control community without legislation.
Search strategies
The following electronic databases were searched using standardized terms: Cochrane Injuries Group Trials Register, Cochrane Central Register of Controlled Trials, DARE (Database of Abstracts of Reviews of Effectiveness), MEDLINE, EMBASE, CINAHL, Web of Science, British Education Index, LILACS Database, and the TRIS (Transport Research Information Service) database. Search terms and outputs are available from the authors upon request. In addition, the grey literature was searched (Google Scholar, University Microfilms (UMI) for dissertations) as were conference proceedings. Finally, reference lists of included studies and communication with authors were also performed to identify unpublished studies.
Study selection
A two-step selection process for study inclusion was used. First, the initial search results were screened by two reviewers and relevant articles were retrieved. Two reviewers then read the full reports to ensure that each met the predetermined inclusion criteria. Disagreements were resolved through consensus or, if necessary, a third person adjudication.
Inclusion criteria
In order to be included in this review, studies needed to be one of the following types:
Cohort studies
These studies were required to involve measurement of helmet use in two groups of individuals in two separate, yet similar communities. These communities were required to be comparable on the basis of environmental conditions, population size, cultural issues, socioeconomic status, and bicyclist population. One community was also required to be exposed to legislation while the control community was not and minimum follow up of six months after legislation implementation was required.
Controlled before-after study
These studies involved direct observations of cyclists. With this approach, exposure to helmet legislation would be introduced at the group level (that is, geographic area); however, the outcome of helmet use would be measured at the individual level. Two or more communities without legislation would be observed. One or more of these communities would subsequently implement legislation.
Interrupted time series studies
These studies involved measurement of helmet use at multiple times before and after the implementation of helmet legislation.
Non-equivalent control group study
These studies were required to involve measurement of helmet use in a community exposed to helmet legislation compared with one or more non-intervention communities in order to determine bicycle helmet wearing prevalence.
Exclusion criteria
Excluded were hospital based studies, telephone or mailing surveys, and self-reported questionnaire based studies.
Quality assessment
There is no specifically designed quality assessment tool in use to evaluate the methodological quality of such observational studies. Some researchers have used the Downs and Black checklist for evaluating cohort studies;24 however, this checklist was designed to assess the methodological quality of both randomized and non-randomized studies of healthcare interventions. A modified version of this form, including 15 applicable questions for these study designs, was independently used by two reviewers (MK, JC) to rate each article.
Statistical analyses
We examined changes in the helmet use proportions among cyclists before and after legislation. We also reported the odds ratios (OR) comparing helmet use before and after the implementation of legislation. For calculating individual and pooled ORs with 95% confidence intervals (CI), we used available population data from intervention and control groups or pre and post-legislation studies.
When available, we used data on helmet prevalence from one year pre-legislation and the last year of the study post-legislation. This approach attempted to negate the temporary effects of legislation immediately after implementation. To explore any variability of the legislation effectiveness on helmet use, age groups, gender, and pre-intervention helmet wearing prevalence were examined in our analyses.
Promotion and enforcement
We reviewed the original manuscripts seeking further information on enforcement/promotion surrounding the implementation of legislation. When no manuscript information was available, efforts to communicate with the lead author of each article were repeatedly made. A three-question electronic mail correspondence was sent on two occasions and the tabulated results were sent for confirmation to each lead author. Authors were requested to provide the promotional activities and enforcement approaches employed during the implementation of legislation.
RESULTS
Description of search
From 86 citations, 25 were assessed as potentially relevant. Overall, 14 studies were excluded based on a priori criteria resulting in 11 studies selected for review. Eight reports were journal publications15,16,21,25–29 and two were formal reports.30,31 One relevant survey was unpublished32 and another incorporated following personal communication with the author.33 Detailed information on each study is provided in the following summaries (see http://www.injuryprevention.com/supplemental).
Description of studies
All of the studies included in this review were published after 1992 (table 1). Studies were based in the United States, Canada, Australia, and New Zealand. Two studies used non-equivalent control groups,15,27 and 10 were interrupted time series or pre-post observational studies.16,21,25,26,28–33 While four included studies involved children of school age exclusively,26–29 eight included all riding ages.15,16,21,25,30–33
The 12 included studies: study methods and population sizes
Among the 12 studies, various cyclist factors were recorded including: age (11), gender (10), location (8), time of day (7), racial characteristics (3), bicycle type (2), backpack use (2), accompaniment (2), and type of road (1) (table 2). Length of follow up after helmet legislation varied between six months30 and 11 years.33 Three studies had <1 year follow up,15,16,30 six studies had 2–3 years follow up,21,25,27,29,28,32 and three studies had four or more years of follow up.26,31,33
General descriptions of the 12 included studies
Two surveys26,27 obtained information only from observational sites in elementary and middle schools, but others collected data from sites everywhere in the communities.15,16,21,25,28–33 Almost all studies used trained observers to collect data in pre-defined sites except one27 which used questionnaires completed by school personnel.
Changes in helmet use proportions
The primary result in most of the studies was the proportion of cyclists using helmets before and after helmet legislation. The baseline rate of helmet use varied between 4% and 59% and this range after legislation changed to be between 37% and 91%. One study demonstrated an increase of helmet wearing proportions after introduction of the law of less than 10%; four studies reported a 10%–30% increase, while seven studies reported an increase of more than 30% (table 3).
Change from baseline helmet use in studies evaluating the effectiveness of legislation on helmet use in cyclists
Long term effect of legislation (two, four, and 11 years) were compared with the short term effects (less than or about one year follow up). The long term effect of helmet legislation was examined by some authors;21,25–29,31–33 five demonstrated an increase of 40% or more,21,25–28 three demonstrated an increase of 21–32%,29,31,33 and one reported an increase of 10%.32 In the longest study identified, helmet wearing remained unchanged 10 years after the introduction of the original legislation.33
Effect measures
The results (OR = 4.60; 95% CI 2.87 to 7.36) indicate that helmet use was more than four times higher following helmet legislation. This result is heterogeneous (I2 = 99%) and four a priori subgroups (type of control group, <16 years old v all-age cyclists, length of follow up, males v females) were examined in an effort to understand this heterogeneity (fig 1). Some of the heterogeneity was explained on the basis of control methodology. The before-after method resulted in a smaller effect size (OR = 4.13; 95% CI 2.45 to 6.97) than the non-equivalent control groups design (OR = 7.8; 95% CI 6.45 to 9.44).

Relationship between the effect of helmet legislation and long term effect of legislation.
The results suggest no clear differences between communities with legislation focusing on children <16 (OR = 4.22; 95% CI 2.03 to 8.76) compared with communities with legislation for all cyclists (OR = 5.35; 95% CI 2.74 to 10.47). In one study, helmet legislation was only in effect for children <18 years old; however, age subgroup information was reported. The subgroup analysis for children generated a larger effect estimate (OR = 12.46; 95% CI 5.16 to 30.10) than the overall effect estimate (OR = 1.51).32
For evaluating the long term effect of legislation on bicycle helmet use, a subgroup analysis using the time period after legislation (<1 year, 1 year, 2 years, 4 years, and 11 years) in each community was performed. The point estimates appear quite dissimilar among these studies based on long term effect (fig 1).
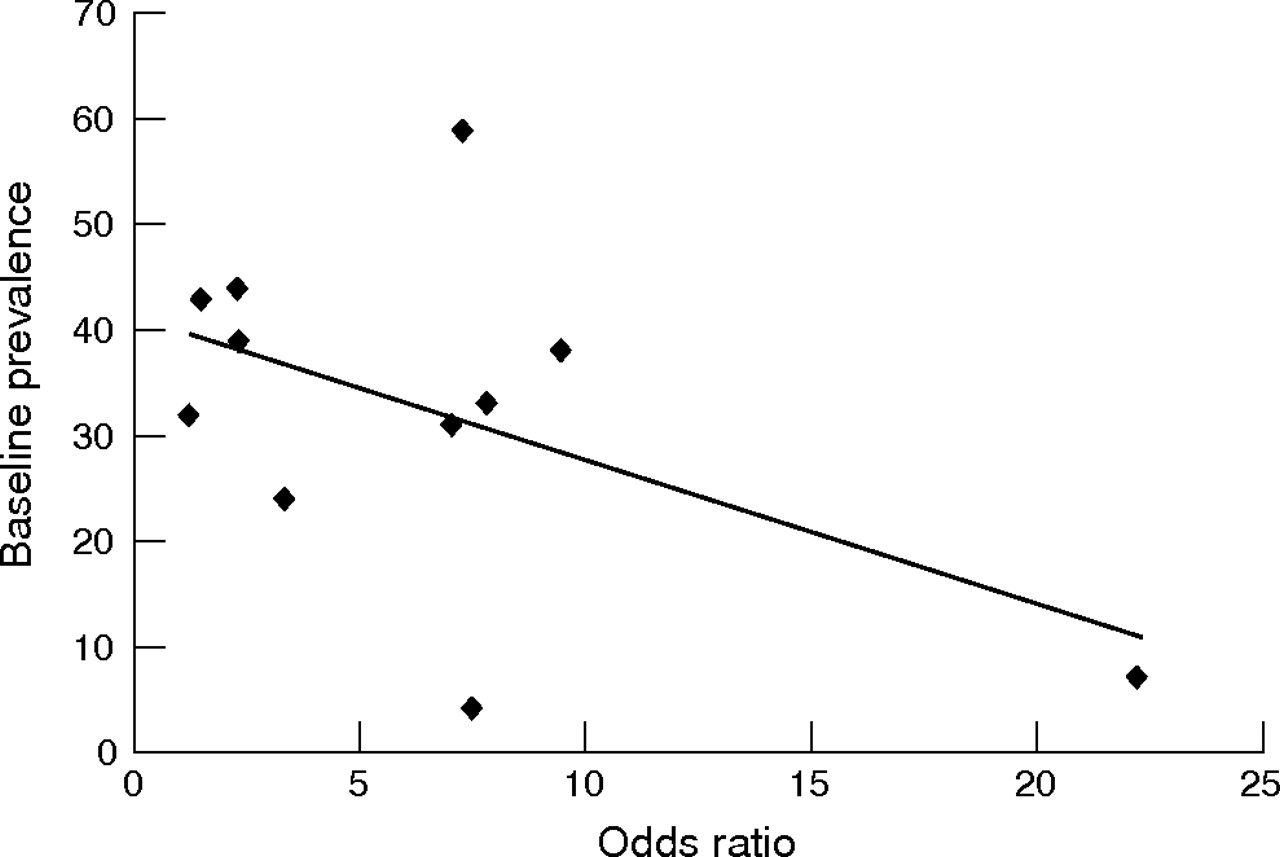
Four studies which provided gender subgroup data failed to identify an influence of gender on the relationship between helmet use and legislation (OR = 5.27; 95% CI 4.20 to 6.62 for men v OR = 5.61; 95% CI 4.90 to 6.42 for women). The possible relationship between the OR of individual studies and the corresponding baseline proportion of helmet use was explored (fig 2); a negative, although not statistically significant, relationship between baseline rate of helmet use and the effect of helmet use after legislation (r = −0.51; p = 0.11) was identified. This subgroup analysis implies that higher baseline proportions of helmet use may be associated with smaller subsequent intervention effectiveness.

{kind=link}
{kind=link}
Relationship between baseline helmet prevalence and odds ratios.
Promotion and enforcement
Overall, email responses were obtained from nine of 12 authors (responses rate: 75%). The results suggest that a variety of promotional activities were associated with implementation of the helmet legislation; however, enforcement was uniformly weak in these regions. These data are presented in table 4.
Promotional activities and enforcement employed in addition to helmet legislation for locations of included studies
DISCUSSION
From 10 observational before/after studies involving 47 417 observations and two non-equivalent control group studies involving 22 193 observations, the results of this review provide insight regarding the effectiveness of bicycle helmet legislation. First, based on the available data it appears that any legislation will increase the use of helmets. Second, this effect reported is not equal in different jurisdictions, and multiple factors are likely responsible.
The effect of helmet legislation on helmet use ranges from modest (OR = 1.24),30 to massive (OR = 22.25).26 The largest effect sizes are observed in studies with lower baseline helmet use,15,26,28 and in those where helmet laws apply to all ages in the community.21,25,31,33 In this review, we were unable to identify any negative relationship between legislation and bicycle helmet use; however, one must wonder if this is a true effect or a consequence of publication bias. Given the paucity of research and our comprehensive attempts to secure published and unpublished data, we feel that this is a valid reflection of the effect of legislation rather than an example of publication bias. Moreover, while the influence of helmet laws appears positive, the magnitude of that change from baseline is difficult to estimate due to the interactions of many factors (for example, time, socioeconomics, incentives, and enforcement) and the estimate of these influences with available information was difficult. Conversely, the requirements of legislation in each jurisdiction might differ and could influence which mechanism of injury prevention would be selected by the policy makers to cope with a public issue.
Results of long term effects suggest that the legislation takes time to produce the desired effect following implementation. Although only two non-equivalent control group studies were available in this subanalysis, the larger effect estimate was generated with a smaller sample size. Overall, this finding is promising; however, further longitudinal studies are needed to determine the role of time in legislative periods.
The effect of socioeconomic status of the community on any increase of helmet use due to legislation is an important consideration. Communities with higher socioeconomic status tend to have a higher proportion of helmet use than mid and low income populations.34–36 When helmet laws come into effect, high income communities demonstrate lower effect estimates.34 Regarding community incentives, the literature indicates a positive effect on helmet wearing.9,25,26 Despite this previous research, however, we were not able to determine the effects of socioeconomic status and incentives, as the included studies failed to provide the level of detail required for analysis.
Confounding effects of some promotional activities such as extensive media campaigns, community incentives, education/instruction in schools, and enforcement following legislation has been widely acknowledged by the researchers. In the New Zealand survey, the rate of helmet use following promotional and educational activities, increased from 11% to 59% (↑45%) over five years.33 In addition, Seattle saw helmet use climb from 3% to 16% (↑13%) in a three year period.9 However, a 10 year study in Australia25 demonstrated that helmet promotion programs accounted for a 30% (6% to 36%) increase in helmet use during an eight year period before legislation (∼4% increase/year); when legislation was subsequently introduced in the ninth year, helmet use increased from 36% to 73% (37%) in one year.
Opponents of mandatory helmet legislation have suggested that legislation has a negative effect on cycling activity.37 Once again, the included studies in this review failed to provide a level of detail on a consistent basis to examine the effect of legislation on cycling participation. This issue was, however, examined by Macpherson et al, in East York, Ontario, Canada, from 1993 to 1999. They studied trends in bicycling among elementary and middle school children during eight years, and found no significant change in the number of cyclists observed per hour from pre- to post-legislation.20 Other researchers from Australia, however, noted decreased adolescent but not child or adult participation two years after introduction of bicycle helmet legislation.25,38
There are several limitations of the review. For calculating initial and pooled odds ratios, we used population data of 11 included studies. The population of one study was not available so it was excluded from analysis.28 Influence of some factors such as media campaigns, educational programs, financial incentives, and police enforcement may have been mixed with the effect of helmet legislation. We did attempt to contact the authors regarding this issue; however, many lacked the knowledge to catalogue all of the associated programs and enforcement activities associated with the legislation. Therefore, we were uncomfortable about formally analyzing the extent of enforcement and educational interventions as they related to helmet prevalence beyond what is presented in table 4. However, the results in table 4 indicate that enforcement activities were not aggressive in any jurisdictions that implemented legislation. Clearly, more work is needed on this issue.
Alternatively, the published evidence does provide some insight into the level of enforcement and helmet legislation effectiveness. Data from Coté et al15 and Ni et al16 support the contention that even with minimal enforcement, there is a significant increase in helmet wearing rates accompanying legislation. Finch found that fear of police and the possibility of receiving a fine for not wearing a helmet was a relatively unimportant reason (∼15%) for wearing even in the face of enforcement.39 Safety was the major reason cited for helmet wearing (54%).39 Cameron et al, reported a 6% to 36% increase in helmet use over an eight year period of promotion; however, a 37% increase in the year following legislation.25 Finally, a major review concluded that “Minimal enforcement of helmet laws does not seem to undermine the positive effects of legislation”.40 The published evidence and our results suggest that perhaps the main effect of the legislation is to educate the community/parents that bike helmets are protective, subsequently changing social norms about helmet use and increasing prevalence. This appears to occur even in the absence of rigorous enforcement.
Key points
-
Overall, helmet legislation increased bicycle helmet use.
-
Legislation was consistently associated with an increase in helmet prevalence; however, variability is present.
-
The effect of legislation appears smaller in areas with a higher baseline proportion of helmet use and areas with high socioeconomic status.
-
Limited evidence exists on the role of helmet legislation for children on adult helmet wearing proportions; one study suggested no effect.
Lack of control group for the surveys was a common problem. This issue is more important for non-equivalent control group studies, but may still be an issue for pre-post intervention studies due to the effect of time bias. Many researchers have been reluctant to attribute causal associations to ecological studies due to the threat of the ecological fallacy. However, consistency in the literature of the positive effect of helmet legislation indicates that we cannot ignore the relationship between helmet legislation and subsequent helmet use.
The pooling of study results in the face of variability of results is controversial. In some cases, reviewers elect to simply present the individual results without a summary statistic. In this case, despite the variability of results, we elected to pool results in an effort to provide an average estimate of the effect of legislation. We recognize this variability, and caution readers regarding the interpretation of the effect estimate.
IMPLICATIONS
Communities
While universal use of helmets is desirable, legislation appears to substantially increase helmet wearing. Subgroup analysis suggests the effect of the intervention may be less impressive where baseline rates are high; however, this does not imply that the intervention should be abandoned in such settings.
Research
Although helmet legislation is effective in increasing helmet use by cyclists, the effect of helmet laws on outcomes (for example, injuries) is also important. These results do not provide detailed evidence of the effectiveness of the components of the legislation, and additional research comparing similar communities with and without helmet legislation is required. Further efforts to explore the transition effect of helmet law expansion from younger to all ages is also required.
Acknowledgments
The authors wish to thank Ms Lynley Povey (Senior Scientist, Research and Statistics, Ministry of Transport; Wellington, New Zealand) for her assistance with this project. Lisa Tjosvold and Carol Friesen are acknowledged for their assistance with constructing the literature searches. In addition, the authors would like to thank an anonymous reviewer for his/her recommendations. Dr Rowe is supported by the Canadian Institute of Health Research (CIHR; Ottawa, ON) as a Canada Research Chair. Dr Hagel is supported through a Professorship in Child Health and Wellness, funded by an Anonymous Donor to the Alberta Children’s Hospital Foundation, Calgary, Alberta, Canada. Part of this work was completed while Dr Hagel was with the Alberta Centre for Injury Control & Research, Dept of Public Health Sciences, Faculty of Medicine and Dentistry, University of Alberta.
REFERENCES
Supplementary materials
Files in this Data Supplement:
- view PDF - Appendix: Characteristics of excluded studies.