Article Text

Abstract
Background Unintentional injuries are a leading reason for seeking emergency care. Refugees face vulnerabilities that may contribute to injury risk. We aimed to compare the rates of unintentional injuries in immigrant children and youth by visa class and region of origin.
Methods Population-based, cross-sectional study of children and youth (0–24 years) from immigrant families residing in Ontario, Canada, from 2011 to 2012. Multiple linked health and administrative databases were used to describe unintentional injuries by immigration visa class and region of origin. Poisson regression models estimated rate ratios for injuries.
Results There were 6596.0 and 8122.3 emergency department visits per 100 000 non-refugee and refugee immigrants, respectively. Hospitalisation rates were 144.9 and 185.2 per 100 000 in each of these groups. The unintentional injury rate among refugees was 20% higher than among non-refugees (adjusted rate ratio (ARR) 1.20, 95% CI 1.16, 1.24). In both groups, rates were lowest among East and South Asians. Young age, male sex, and high income were associated with injury risk. Compared with non-refugees, refugees had higher rates of injury across most causes, including for motor vehicle injuries (ARR 1.51, 95% CI 1.40, 1.62), poisoning (ARR 1.40, 95% CI 1.26, 1.56) and suffocation (ARR 1.39, 95% CI 1.04, 1.84).
Interpretation The observed 20% higher rate of unintentional injuries among refugees compared with non-refugees highlights an important opportunity for targeting population-based public health and safety interventions. Engaging refugee families shortly after arrival in active efforts for injury prevention may reduce social vulnerabilities and cultural risk factors for injury in this population.
- immigration
- injury
- Ontario
- paediatric
- refugee
- migration
Statistics from Altmetric.com
Background
Unintentional injuries are largely preventable yet continue to be a leading reason for children and youth to seek emergent medical care.1 Socioeconomic disadvantage, more specifically, low income and parental education, has been recognised as a risk factor for childhood injury.2–5 However, other social vulnerabilities, including immigrant and refugee status, have been less well studied and their influence on injury risk is poorly understood. Population-based public health strategies aimed at preventing injuries have reduced some socioeconomic inequities that contribute to injury.6–8 With rising levels of global migration, the role immigration factors play in contributing to injury is becoming increasingly important. Such factors may represent opportunities for targeted injury prevention in children and youth.
Immigrants now represent 20% of the Canadian population.9 Depending on the context of their experiences prior to migration including their home country safety standards, culture, settlement experiences and environment after arrival, risk of injury may vary. Immigrant children and youth have recently been identified as having lower rates of unintentional injury compared with their non-immigrant counterparts in both Canada and Denmark.10 11 Moreover, neighbourhood level income, which typically has a strong inverse association with injury risk in non-immigrants, has not been observed among immigrants.10 This suggests different causal pathways for injury among immigrants. In particular, refugee immigrants may face social stress, substandard housing and play spaces, and lack of access to safety equipment, which may increase their risk of injury.
Immigrants may come to Canada and become permanent residents (granted the right to live and work in Canada without limitations on their stay) through one of several immigration visa classes. One major class includes refugees, who are admitted to Canada because they are in need of protection. These immigrants typically have fewer supports, and often have had traumatic experiences prior to migration. Health outcomes for several conditions are worse in refugee compared with non-refugee immigrant populations across the globe.12 This contrasts with the majority (approximately 88%) of immigrants who come to Canada annually as economic or family class immigrants. These latter classes are selected through stringent criteria and must demonstrate reasonable health and potential to contribute to Canada’s economy. While these individuals are often highly skilled, educated and motivated, they too may face socioeconomic disadvantage upon arrival, cultural and language differences, and challenges adapting to and functioning in a new environment.
In this study, we aimed to describe and compare the rates of unintentional injuries in immigrant children and youth in Ontario, Canada, by immigration visa class and region of origin. Given refugees face different exposures prior to and after arrival, have lower socioeconomic status, and potentially different risk-taking behaviours, we hypothesised that refugee children and youth would have higher rates of injury compared with non-refugee immigrants.
Methods
Study design
This was a population-based, cross-sectional study using linked health, administrative, and immigration data in Ontario, Canada. Access to study data was available through research agreements between the Institute for Clinical Evaluative Sciences (ICES) and Immigration, Refugees and Citizenship Canada, as well as ICES and the Ontario Ministry of Health and Long-Term Care. Research ethics board approval was obtained from The Hospital for Sick Children and Sunnybrook Health Sciences Centre in Toronto, Ontario.
Data sources
Several databases were linked using unique, encoded health identification numbers and analysed at ICES. In Ontario, residents are insured for medically necessary care from physicians and hospitals under the province’s single-payer universal Ontario Health Insurance Plan (OHIP). Immigrants admitted to Canada as permanent residents are typically eligible for OHIP after 3 months of residing in Ontario. Alternative health insurance, either privately or through the Interim Federal Health Program, often insures immigrants and refugees during this brief waiting period but these data are not available for linkage. Ontario’s healthcare registry, the Registered Persons Database, contains sociodemographic information for all residents eligible for OHIP and includes their age, sex and postal code. Immigrants were identified using the Ontario portion of the Permanent Resident Data System (PRDS), a federal database maintained by Immigration, Refugees and Citizenship Canada. The PRDS contains individual-level demographic information, including visa class and country of birth, for permanent residents with landing dates from 1985 to 2012. Information is collected at the time of landing in Canada from official immigration documents. Detailed linkage information to ICES holdings has been previously published and has demonstrated that over 86% of individual immigrants in the PRDS can be probabilistically and deterministically linked to ICES holdings.13 Data on temporary or undocumented immigrants are not included in this database.
The MOMBABY database, derived at ICES, pairs all mothers with their newborns delivered in Ontario hospitals through the Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD) hospital records of delivering mothers and their newborns. Linkage rates are approximately 96%. This database was used to identify newborns born in Canada to immigrant mothers. The CIHI-DAD and National Ambulatory Care Reporting System contain information, including diagnoses, on admissions and emergency department (ED) visits to Ontario hospitals, respectively. Neighbourhood income quintile was obtained using Statistics Canada’s Postal Code Conversion File to link a patient’s postal code to dissemination areas based on 2006 Canadian Census data.
Study population
Children and youth from immigrant families who were 0–24 years of age during the study period (1 January 2011 to 31 December 2012) were included if they had a PRDS record, or were born to an immigrant mother with a PRDS record, linked through the MOMBABY database. Maternal immigrant status was used to identify children included in the study to reflect the influence of family immigrant status, rather than that of only the child. Maternal immigrant status has been previously associated with risk of injury.14 Records with a missing or invalid health card number, age or sex were excluded.
Independent variables
The main independent variable was immigration visa class. Immigrants were grouped according to admission visa class as either refugees or non-refugees. Refugees included government-assisted refugees, privately sponsored refugees, refugees landed in Canada, refugee dependents and blended visa office-referred refugees, as defined by Immigration, Refugees and Citizenship Canada.9 All other permanent resident immigrants were considered non-refugees.
We included as covariates age (on 31 December 2011), sex and neighbourhood income quintile as these have been shown to be associated with injury.8 15 16 Region of origin, based on modified regions from Immigration, Refugees and Citizenship Canada,9 was also used as a covariate (online supplementary file 1).
Supplementary file 1
Outcome measures
The main outcome measure was the rate of unintentional injury-related hospitalisations and visits to EDs, and the rate of unintentional injury-related deaths (in and out of hospital). The cause of injury was grouped according to previously published and internationally recognised standards for injury reporting, which include injury intent and cause of injury.1 17 Injury codes used for this study are available in online supplementary file 2. Multiple visits by the same patient were included; however, only one event per patient per day was included. Where an emergency room visit led to a hospitalisation or death, only the more serious event was counted.
Supplementary file 2
Statistical analysis
Descriptive statistics were performed for the independent variables, outcome variables and covariates. To compare outcomes of immigrants by visa class, multiple variable Poisson regression models adjusting for overdispersion were used to compute rate ratios with 95% CIs. For each model, variables were selected a priori and included in the regression analysis. The main model included both refugees and non-refugees and models were also then stratified by visa class. Multiple variable Poisson regression models were then used to model cause-specific injuries by visa class, adjusting for age, sex, neighbourhood income quintile and region of origin. All statistical modelling was carried out using SAS Enterprise Guide, V.6.1 (SAS Institute).
Results
There were 999 951 immigrants included in the cohort. Up to 15.4% of immigrants were refugees. Most immigrants were from South Asia (26.9%) and East Asia and the Pacific (22.6%). The largest proportion (24.6%) of refugees were from South Asia, followed by Africa (22.6%). Compared with non-refugee immigrants, refugees were older and had a larger proportion of individuals living in the lowest neighbourhood income quintile (table 1).
Cohort of immigrant children and youth in Ontario, Canada, overall and by visa class, 2011–2012
There were 53 074 and 11 861 injury-related ED visits annually in non-refugee and refugee children and youth, respectively. This corresponded to rates of 6596.0 and 8122.3 ED visits per 100 000 non-refugees and refugees (table 2). Injury-related hospitalisation rates were higher among refugees (185.2 hospitalisations per 100 000 refugees) compared with non-refugees (144.9 hospitalisations per 100 000 non-refugees) (p<0.0001), as were injury-related deaths (5.8 deaths per 100 000 refugees vs 4.0 deaths per 100 000 non-refugees) (p=0.028) (table 2). ED visits for injuries in both groups and deaths from injuries among refugees increased with increasing neighbourhood income quintile whereas hospitalisations and deaths from injuries among non-refugees did not show this income gradient (table 2).
Unintentional injury-related ED visits, hospitalisations and deaths by visa class, 2011–2012
Table 3 shows the Poisson regression model of the association of unintentional injury and visa class adjusted for age, sex, neighbourhood income quintile and region of origin. Overall, the rate of unintentional injuries among refugees was 20% higher than among non-refugees (adjusted rate ratio 1.20, 95% CI 1.16, 1.24). Young age, male sex and living in a high-income neighbourhood were associated with injury risk. There was considerable variability in risk of injury by region of origin with lowest rates among East Asian and South Asian immigrants. In the stratified models, the association between young age and injury risk in non-refugees was stronger compared with refugees. The effect of neighbourhood income quintile on injury risk was similar between refugees and non-refugees. Compared with non-refugees from the USA, UK and Western Europe (reference group), rates of injury were lower among non-refugees from all other regions. Within the refugee group, injury rates (compared with the reference group) were only lower in refugees from East and South Asia and Africa.
Rate ratios for unintentional injuries by visa class and sociodemographic variables, 2011–2012
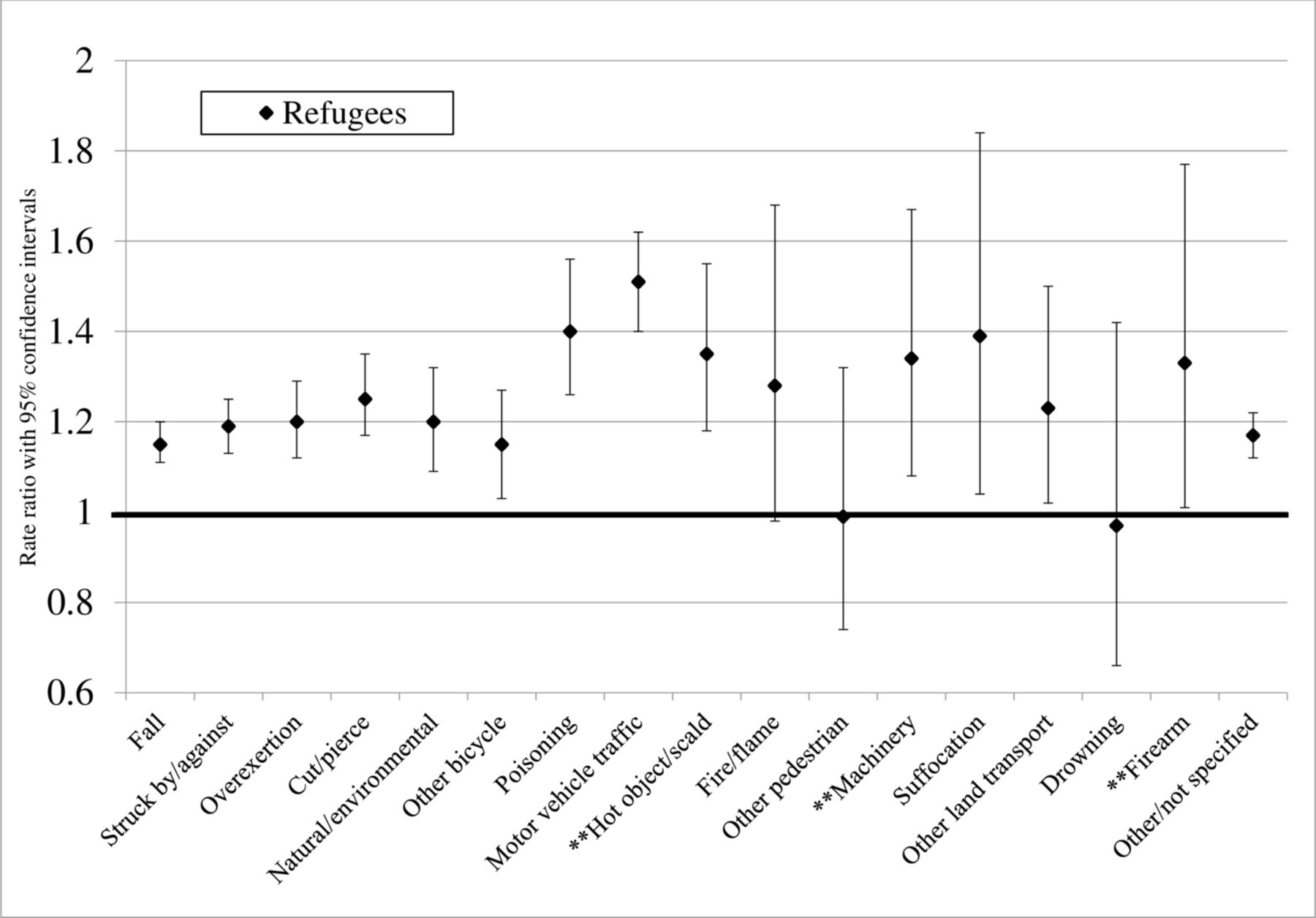
The cause-specific rate ratios for unintentional injury comparing refugees to non-refugees are shown in figure 1. Refugees had higher rates of injury for most causes, except fire/flame injuries, pedestrian injuries and drowning. Compared with non-refugees, the rates of unintentional injury in refugees were higher from motor vehicle injuries (by 51%), poisoning (by 40%), suffocation (by 39%) and scald burns (by 33%).
{kind=link}
Rate ratios of unintentional injury by cause of injury in refugee versus non-refugee immigrants (Reference=non-refugees). Adjusted for age, sex, neighbourhood income quintile and region of origin. **Region of origin not included in the model.
Discussion
This population-based, cross-sectional study examined unintentional injuries among refugee and non-refugee immigrant children and youth in Canada’s largest province (population over 13 million). We report refugee immigrants having a 20% higher rate of unintentional injuries compared with non-refugee immigrants and injury rates higher among refugees across almost all causes of injury. There was wide variability in injury rates by region of origin and refugee status, with lower rates of injuries among South Asian, Middle Eastern and South American non-refugees compared with their refugee counterparts.
To our knowledge, this is the first study in children and youth to explore unintentional injuries and cause-specific injury risk among immigrants by immigration class. One adult study has identified an association between refugee status and unintentional injuries in immigrants to Denmark but only explored injury fatalities.11 Our group has previously demonstrated lower rates of unintentional injuries among children and youth who are non-immigrants compared with immigrants (both refugee and non-refugee)10; however, the within-immigrant comparisons of the current study allow for a deeper understanding of how refugee status influences injury risk by accounting for migration factors (both measured and unmeasured) that may be common to both refugee and non-refugee immigrants.
The observed findings in our study may be explained by potential differences in environmental as well as intra and interpersonal factors between study groups. Neighbourhood level income has previously been shown to be inversely associated with injury risk,7 8 18 though not among immigrants10 or in the current study. This finding may be related to different healthcare-seeking behaviours among immigrants, especially for minor injuries or to lower rates of physical activity including high-risk sporting activities among immigrants living in low-income neighbourhoods. However, other measures of individual-level social vulnerability such as housing safety (overcrowding, functioning smoke alarms, safe storage of toxic substances, installation of safety devices, or housing repairs, and so on), limited English or French language proficiency and parental education were not accounted for and may, in part, explain our results. Low parental education, more common among refugees, has been associated with higher rates of injury in children.2 Similarly, limited multilanguage injury prevention messaging particularly for road safety, instructions for machinery and burn prevention strategies may be a factor in injury risk, especially among refugees. Environmental exposures such as access to safe playground spaces,8 19 properly fitted child restraints for cars6 or helmets for bicycles20 21 can reduce injury risk and may also play a role in contributing to injury among refugee children and youth.
Regional variation in injury risk may be reflective of differing regulations in home country safety standards or cultural practices (eg, safe sleeping practices,22 cooking customs,23 time spent participating in free play,24 25 supervision of children26 27). The rates of injury among young children compared with adolescents in our study (both in refugees and non-refugees) are higher than reported rates in the general population of Canadian children and youth.28 This supports the notion that some of these cultural practices may contribute to injury risk, especially among young children. In refugees and non-refugees, prioritisation and awareness of safety may differ as competing life stressors may differ. For refugees in particular, social isolation with limited options for childcare,29 30 and mistrust of officials or concern for accusations of neglect may preclude caregivers from asking about injury prevention. These same factors may also lead to under-reporting of minor injuries and therefore may be conservative estimates of injury rates.
Strengths and limitations
This is the first study to report injury risk by refugee status and explore cause-specific injury risk. Using linked immigration and health administrative data, we objectively measured injury rates in these populations. Self-reported injuries typically underestimate the true burden of injuries,31 especially in populations where stigma or cultural barriers may influence reporting. In using administrative databases, we have almost complete provincial representation of the immigrant population in Ontario, in a setting with a large, diverse population. This study may be generalisable to other jurisdictions such as Australia, the USA and Western Europe, where both similarly large, varied immigrant populations and comparable safety standards exist.
Several limitations to our study must be noted. Immigrants were grouped based on country-level proximity, and while they likely shared several cultural and other similarities, heterogeneity within regions did not allow conclusions about country-specific injury risk. Our immigration data only contain information on permanent residents with provincial health insurance and do not include undocumented immigrants, failed refugee claimants, or temporary foreign workers, or those recently arrived (less than 3 months) in Canada and our findings may not be generalisable to these specific groups. Undocumented refugees, while a small proportion of all immigrants, are likely a high-risk group and our results may therefore be an underestimate of the true burden of injuries in this population. We only measured injuries that were serious or resulted in a visit to an emergency room. Not all injuries resulted in a healthcare interaction as minor injuries may have been treated at home and care-seeking behaviours may differ between study groups. Our study did not include contributing factors which may have helped to further contextualise our findings, including participation in sports, behavioural diagnoses that may increase risk for injury, or parental education levels as these were not available through administrative data. Linkage at ICES only allows for maternal immigration status to be ascertained. Paternal immigration factors may also be important for understanding risk of injury.
Conclusions
Refugees have unintentional injury rates that are 20% higher than non-refugee immigrants. This has been observed across most causes of injury with particularly large differences identified for motor vehicle injuries, poisoning, suffocation, scald burns and machinery-related injuries. Population-based public health and safety interventions can effectively reduce these types of injuries; however, we have identified a need for more targeted interventions for refugee families in Canada where social vulnerabilities and cultural differences may be contributing to injury risk. Engaging refugee families shortly after arrival in active efforts for culturally appropriate and language congruent injury prevention is needed.
What is already known on the subject
Unintentional injuries are largely preventable yet continue to be a leading reason for children and youth to seek emergent medical care.
Some social vulnerabilities, including low income and education, have been recognised as important contributors to injury risk and have become targets for population-based public health strategies aimed at preventing injuries.
What this study adds
Refugees have a 20% higher rate of unintentional injury compared with non-refugee immigrants, with higher rates of injury observed across most causes of injury.
There is wide variation in injury rates by region of origin.
Refugees have been identified as a population in need of more targeted interventions to reduce injury risk.
References
Footnotes
Contributors NRS conceptualised and designed the study, interpreted the results, drafted the initial manuscript, revised the manuscript and approved the final manuscript as submitted. JG analysed the data, revised the manuscript and approved the final manuscript as submitted. AM and AG conceptualised and designed the study, interpreted the results, revised the manuscript and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding AG and AM are funded through Applied Chairs in Child Health Services and Policy Research from the Canadian Institutes for Health Research. All data analyses were funded through AG’s Research Chair. This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent of the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI) and Immigration, Refugees and Citizenship Canada (IRCC). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of CIHI or IRCC.
Competing interests None declared
Ethics approval Hospital for Sick Children and Sunnybrook Health Sciences Centre Research Ethics Boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data set from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at . The full data set creation plan is available from the authors upon request.