Article Text

Abstract
Objective To assess clinical management of disorders of sex development (DSD) subsequent to recommendations issued in the 2006 Consensus Statement.
Design Online questionnaire and audit of DSD literature.
Setting Invitation to complete a 28-item online questionnaire and a 12-item follow-up questionnaire, both assessing current clinic statistics and clinical management of DSD.
Participants Paediatric endocrinologists from 60 medical centres representing 23 European countries.
Main outcome measures Clinic activity, multidisciplinary team composition, provision of psychological support services, incidence of feminising clitoroplasty and use of diagnostic algorithms and newly proposed nomenclature.
Analyses Data are reported in terms of percentages with respect to implementation of recommendations outlined in the Consensus Statement. χ2 was used to analyse changes in nomenclature reported in the literature.
Results 60 centres reported on management of an average of 97.3 (range 8–374) patients per year, totalling approximately 6000. The mean number of new referrals in the previous year was 23.27 (range 8–100). 57% of centres regularly included the services of recommended paediatric subspecialists: paediatric endocrinologist, paediatric surgeon/urologist, plastic surgeon, paediatric psychiatrist/psychologist, gynaecologist, clinical geneticist, histopathologist and neonatologist; 35% reported providing these and additional services of endocrine and surgical nurses, a social worker and a medical ethicist. Additionally, 95% of centres reported offering primary psychological support services (either child psychiatrist or psychologist). 65% of centres reported using a diagnostic algorithm, and 83.3% supported the development of a standardised algorithm. 52% and 44.8% of centres reported having performed fewer or similar numbers, respectively, of clitoroplasties than in previous years and only 3.4% reported an increase. Finally, 100% of respondents reported using the newly proposed terminology. Likewise, an audit of the literature reflected a recent reduction in usage of the non-preferred historical terminology.
Conclusions There is evidence that the majority of European DSD centres have implemented policies and procedures in accordance with the recommendations issued by the 2006 Consensus Group. These findings represent a change in practice with the collaborative goal of improved patient care.
Statistics from Altmetric.com
In 2006, a consensus statement1 2 reviewing multidisciplinary management and long-term outcome of disorders of sex development (DSD, formerly intersex) was published by 50 international experts and endorsed by the Lawson Wilkins Paediatric Endocrine Society and the European Society for Paediatric Endocrinology (ESPE). The result was to make recommendations across the field, from sex assignment and management at birth to long-term patient follow-up. In summary, the Consensus made the following recommendations:
▶. Nomenclature should be revised to reflect careful consideration of the concerns of patients.
▶. Management must be carried out by an experienced multidisciplinary team, including mental health staff with expertise in DSD.
▶. All individuals should receive a sex assignment, but only after expert evaluation.
▶. Only surgeons with specific training/expertise should undertake surgical procedures.
▶. Feminising surgery should only be considered in cases of severe virilisation.
▶. Emphasis of surgical intervention in all cases should be on functional outcome rather than strictly on cosmetic appearance.
▶. Open communication with patients/families is essential and participation in decision, making is encouraged.
What is already known on this topic
The need for a multidisciplinary team approach to management of DSD, as put forward in the Consensus Statement, has been widely agreed upon; however, this is the first report to demonstrate the implementation of such recommendations across the UK and Europe.
What this study adds
This study takes the movement for improved DSD patient management forward in that it formally establishes that progress is being made. The next step in this process is to assess long-term outcomes as a function of the reported changes in patient care.
Two years on, it seemed appropriate to assess the impact of the statement. First, however, the usefulness of a consensus statement bears consideration. In recent years, a growing number of consensus statements have been devised for various disorders.3,–,5 Critics suggest that such reviews sideline original research and have the potential to stifle innovation6 and that one must be mindful that not all constituents agree entirely with the completed statement. Nevertheless, such documents aim to proffer above and beyond the most recent book chapter, offering clearly defined guidelines representing “best fit” ideas from leaders in the field. Even so, without changes in practice, a consensus statement is superfluous. In the case of the consensus on management of DSD, the drive was to provide current and comprehensive structure for the treatment of disorders which have historically been controversial and to overhaul an outdated and insensitive nomenclature. Here, we assess practice following on from the consensus.
For the current report, we collected statistics and surveyed practices of 60 DSD centres in 23 European countries. We report on patient numbers, surgical procedures, multidisciplinary collaboration, psychosexual evaluation and the formal implementation of the newly proposed nomenclature. In addition, we sampled peer-reviewed reports on DSD before and subsequent to the proposal of the new lexicon to see which terms clinicians and academics used in scholarly publications.
Methods
Participants
Paediatric endocrinologists from 77 medical centres were invited to take part in the survey. Sixty (78%) centres completed the survey, representing 21 EU countries and two countries outside the EU (Turkey and Switzerland). Additionally, we sent a secondary survey to all those who completed the initial survey for clarification on four items. Thirty (50%) of original respondents completed the follow-up survey.
Survey
The initial survey contained 28 items/questions assessing DSD patient numbers, using the classification system proposed by the Consensus, provision of specific DSD clinics, surgical procedures, multidisciplinary collaboration, psychosexual management, sex assignment in cases of ambiguous genitalia or sex dissatisfaction, usage of/preference for diagnostic algorithm(s), institutional education and research, support group affiliation(s) and use of the proposed nomenclature. In the follow-up survey, we asked for more detailed information on frequency of DSD clinics, exact patient numbers (rather than ranges), clarification on incidence of clitoroplasty and more specific usage of nomenclature. Regarding clitoroplasty, we originally asked if this operation was performed in similar, greater or lesser numbers compared to previous years; on follow-up, we asked whether this estimation was independent of increases/decreases in case load. With respect to nomenclature, we asked about the specific context of usage, that is, as descriptive, diagnostic or not at all. In both survey designs, we sought feedback from paediatric endocrinologists and patient-advocacy groups.
Literature sampling
We recorded the use of the following search terms: intersex, hermaphrodite, pseudohermaphrodite and disorder of sex development by sampling 200 titles/abstracts from articles published in the 2 years before the Consensus Statement and 160 titles/abstracts from articles published in the 2 years following the Consensus Statement.
Statistical analyses
Reports are presented in terms of percentages. As there were no previous data of this kind, we were unable to make comparisons across time. Also, we have not made comparisons across centres or countries due to inter-centre variation. With respect to the literature sampling, χ2 was used to assess differences in terminology use before and after the proposal of a new lexicon.
Results
Centre statistics
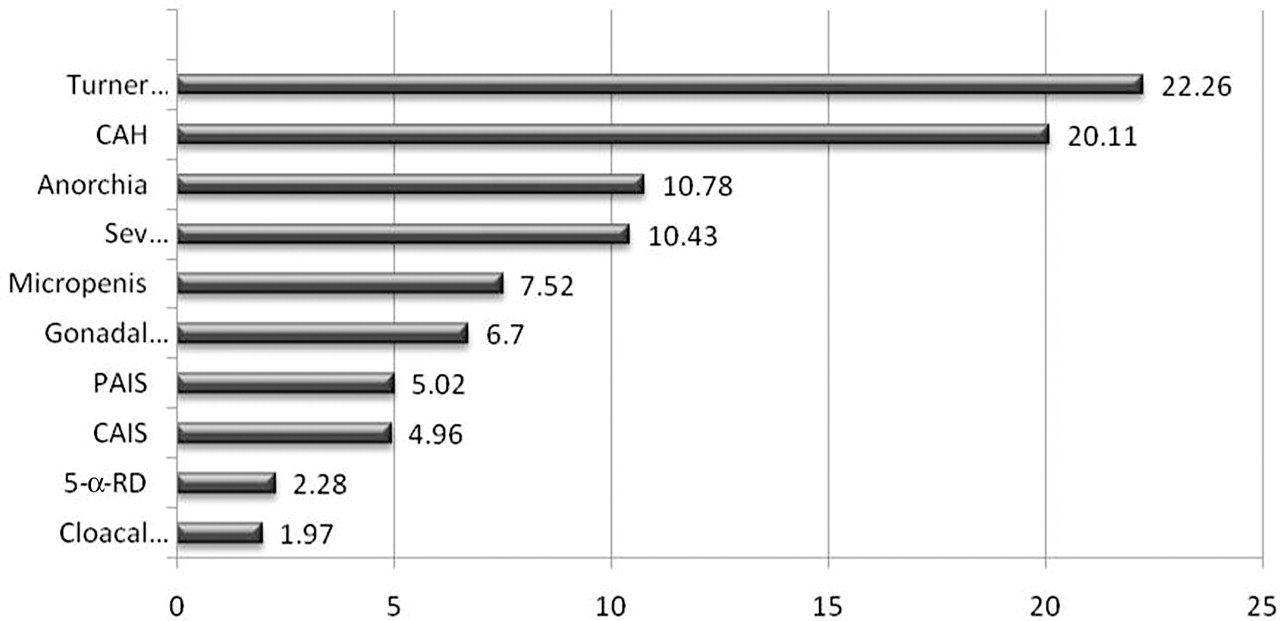
Figure 1 shows mean patient numbers by diagnostic category and centre. The total number of cases seen in the previous year across the 60 centres was approximately 6000. The number of new referrals during this period across all centres was approximately 1400.

Mean number of patients per disorders of sex development (DSD) centre by diagnosis. 5-α-RD, 5-alpha reductase deficiency; CAH, congenital adrenal hyperplasia; CAIS, complete androgen insensitivity syndrome; PAIS, partial androgen insensitivity syndrome.
With respect to specific DSD clinics, 58.3% of centres reported that they held a clinic designated solely for DSD patients: 38% for CAH and 41.7% for Turner syndrome. In the follow-up survey, 50% of centres reported that they held a DSD clinic at least monthly.
Investigations and management of DSD
Multidisciplinary team
A key point of the Consensus Statement was the recommendation of a multidisciplinary approach, specifically the involvement of a number of paediatric subspecialists. These included paediatric endocrinologist, paediatric surgeon/urologist, plastic surgeon, paediatric psychiatrist/psychologist, gynaecologist, clinical geneticist, histopathologist and neonatologist. Ideally, there should also be a social worker, specialist nursing staff and a medical ethicist. Figure 2 shows an analysis of the subspecialties. Remarkably, 57.6% of centres provided for nearly all recommended subspecialties (excluding social worker, specialised nursing staff and/or medical ethicist), and 35.6% of centres reported providing all recommended services. Only 6.8% of centres were missing a key service, that is, paediatric endocrinologist, urologist/surgeon and/or psychological services.

Multidisciplinary team composition. Shows the percentage of centres (N=60) whose team composition is ideal, intermediate or missing key services. Ideal team: paediatric endocrinologist, paediatric surgeon/urologist, plastic surgeon, paediatric psychiatrist/psychologist, gynaecologist, clinical geneticist, histopathologist and neonatologist; Intermediate team: all subspecialties except specialist nursing, social work or medical ethicist; Missing key services: missing paediatric endocrinologist, psychological services or urologist/surgeon.
Diagnostic and clinical evaluation
Sixty-five per cent of centres reported using a diagnostic algorithm and 83.3% expressed favour for a standardised protocol. Overall, 95% of centres reported using published norms for evaluation of ambiguous genitalia, with 75.4% using the Prader scale7 and 8.8% the external masculinisation score8; 10.5% reported using both systems. Additionally, all centres had access to biochemical and genetic investigations, of which 76.7% were available from within their own institution.
Psychosexual management
Sex assignment, reassignment and dissatisfaction
The call en masse for regular psychological support services for patients and families appears to have been answered. Only 5% of 60 reported that neither of these services was currently available. Figure 3 shows an analysis of psychological services.

Proportion of disorders of sex development (DSD) centres (total=60) providing primary psychological services (child psychiatrist/paediatric psychologist) according to level of care.
We also enquired about the inclusion of psychological services in cases of sex assignment/reassignment. Of the initial 60 centres surveyed, 63% involved a psychologist specialising in DSD in the decision-making process from the outset. Conversely, 24% reported rarely or never employing such a subspecialist. In the follow-up survey, we asked respondents to estimate what percentage of sex reassignment cases involve specialised psychological services. While 80% of all cases involved a psychiatrist/psychologist, most centres reported that 100% of patients and families were offered the service. Finally, few cases of sex dissatisfaction were reported (n=37 across 30 centres), and approximately 57% of these cases took advantage of psychological support.
Surgical management
Clitoroplasty
There has been a trend away from clitoroplasty: 52% of respondents to the follow-up survey reported a reduction in the number of clitoroplasties, and 45% reported no change in practice. Only one centre reported an increase.
Nomenclature and definitions
Figure 4 reflects usage of historical and newly proposed nomenclature as reported by 30 centres in the follow-up survey. Figure 5 shows the change in nomenclature usage in peer reviewed publications. χ2 analysis indicated that use of non-preferred historical terms has significantly decreased (p=0.000, p=0.067 and p=0.000 for the terms intersex, hermaphrodite and pseudohermaphrodite, respectively) in the 2 years following the publication of the Consensus Statement.
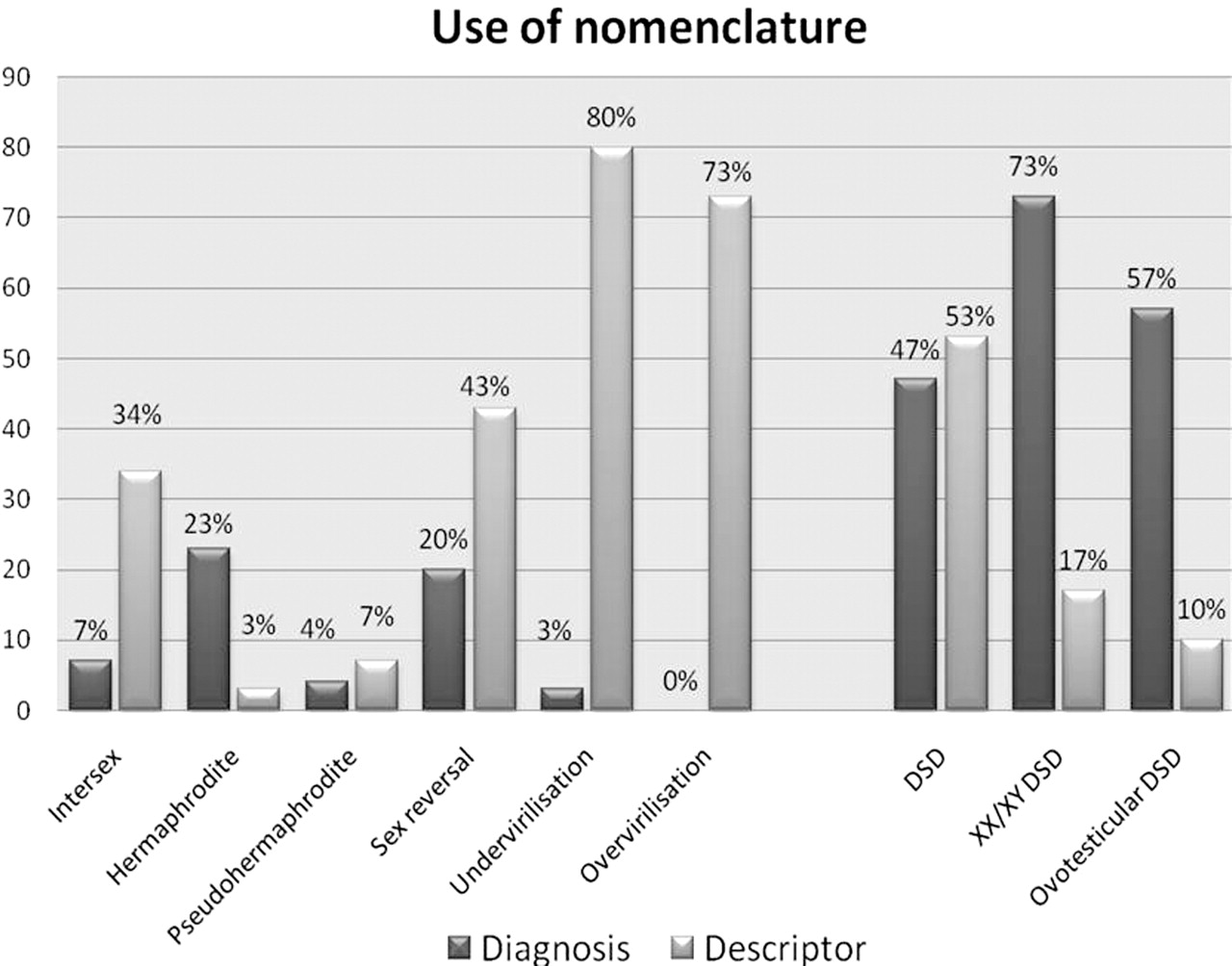
Change in clinical usage of nomenclature as descriptors or diagnoses subsequent to publication of the 2006 consensus statement. Percentages represent numbers of respondents who report using each term in respective contexts.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Numbers represent % of reports in the literature using former and newly proposed terminology. Terms were only counted when used in a diagnostic capacity rather than as a descriptor.
Discussion
The current report describes statistics/demographics and case management of DSD in 60 European centres, representing approximately 6000 patients. The findings suggest that the majority of centres were practising in accordance with recommendations made by the 2006 Consensus Statement.1 2
A fundamental recommendation of the statement was that of a multidisciplinary approach to management of DSD. Remarkably, 93% of centres reported that they included the majority of recommended subspecialists in routine patient care. Thirty-six per cent of centres provided all subspecialties, while the remainder included all except specialist nurses, social worker and/or medical ethicist. This survey is the first evidence that the multidisciplinary approach to DSD has been successfully implemented across Europe. The consensus highlighted a specific need for psychological support services, and it is gratifying that this has been achieved. Only three centres did not offer psychological support. Surprisingly, most respondents indicated that 100% of new patients were offered psychological support; yet, the average uptake of such services across centres was only 54%. It is unclear which factors contribute to rejection of additional support services, and further studies are needed to evaluate accessibility.
More than 75% of centres reported using published norms for the diagnostic evaluation of ambiguous genitalia of the newborn, and 65% used a diagnostic algorithm. The Consensus Statement suggested that guidelines for a uniform protocol would not be appropriate; yet, most respondents would favour a standardised algorithm. Consideration should now be given as to how best this could be achieved.
An important recent criticism of management in female-assigned infants with DSD is that some feminising clitoroplasties are performed mostly for cosmetic reasons and when the individual is too young to consent.9 This has resulted in proposals ranging from a moratorium on surgery to establishing guidelines for when such surgical procedures are warranted.10 Our survey indicated that there has been a trend away from early clitoroplasty, with 52% of centres reporting a reduction in recent procedures. This is remarkable in the light of previous guidelines such as the “Optimal Gender Policy”11issued in the 1950s which stated that the genitals should be feminised as soon as possible in female-assigned DSD. Given the change in practice, it is anticipated that evidence of an improvement in satisfaction with sexual function will be found in future long-term outcome studies.
The most radical recommendation to emerge from the 2006 Consensus was the proposal to completely overhaul the nomenclature allied to this branch of medicine. There have been criticisms that the historical terminology proffered in the 1950s has been pejorative and confusing.11 The generic term DSD was proposed and defined as congenital conditions in which development of chromosomal, gonadal or anatomical sex is atypical.1 2 A more specific taxonomic system evolved that integrates advances in molecular genetics and lends precision when applying diagnostic labels. The survey indicated almost universal usage/satisfaction with the modern lexicon. Furthermore, the medical/scientific communities have embraced the changes in a remarkably short period of time based on surveys of the peer-reviewed literature, standard textbooks and the contents of grant applications for research in this field. Such a profound and rapid change in terminology is without parallel in recent medical practice.
There are limitations inherent in a questionnaire-based study due to the nature of the data collection and the response bias. Twenty-two per cent of centres did not respond to the primary survey, and there was an uneven distribution of response across countries. Practice and institutional characteristics vary between countries, factors which may influence results of the study. Furthermore, response rates may have been higher among centres with practices more compliant with the Consensus Statement, producing a positive bias in our report. Gathering more detailed information on each centre would have been advantageous, but a balance needed to be struck between maximising data collection and achieving a desirable response rate. Finally, the survey did not address practice before the Consensus Statement; hence, only speculative conclusions can be drawn on whether the statement alone has been a driving factor for change. The exception to this is the change in nomenclature used in scientific literature, where a comparison can be made pre- recommendations and post-recommendations.
The evaluation of clinical practice and recommending best practice has spawned a list of methodologies labelled as consensus statements, position statements, clinical guidelines or clinical practice guidelines. The 2006 Consensus Statement arose from a process that was guided by systematic reviews of evidence, meetings of the task force and subsequently several drafts of the final statement. Formulation of the recommendations was not based on the Recommendations, Assessment, Development, Evaluation12 System nor was the quality of evidence rated low–high. Consequently, according to the evidence-grading system for clinical practice recommendations proposed by the American Diabetes Association,13 expert consensus or clinical experience defines an E level of evidence and, hence, embraces the DSD consensus. What this paper highlights is evidence that a consensus statement can be “transformative” as referred to in a recent editorial.6 This applies particularly to a major change in the medical lexicon. Now that there is evidence of a change in clinical practice in Europe, it is behoved of centres providing care for families with DSD to contribute information that indicates patient satisfaction is indeed improving, and longer-term outcome measures are being collated. A start towards that goal has been made through establishment of the Euro DSD program, supported by the ESPE and the European Union FP7 programme.14
Acknowledgments
We acknowledge the helpful feedback on survey design from Faisal Ahmed, Sue Elford, Margaret Simmons and John Achermann. The time and effort expended by staff of participating centres in providing their data is much appreciated.
References
Footnotes
-
Funding This project was supported by the Cambridge NIHR Biomedical Research Centre.
-
Competing interests None.
Ethics approval Ethical approval was granted by the Cambridge Local Ethics Committee as part of studies on DSD.
Provenance and peer review Not commissioned; externally peer reviewed.