Article Text

Abstract
Background The National Health Service Plan (July 2000) aimed to empower patients with more influence upon their own treatment. Provision of additional educational health information (AEHI) serves to inform families about health conditions and to allow them to manage their own health after discharge. However, to date, it is unknown how parents or carers perceive this information.
Objectives To identify parents' and carers' views towards the current provision of AEHI following discharge of their child from an emergency care service, to assess their needs concerning AEHI and to provide recommendations for subsequent research.
Methods Between 11 April and 19 June 2007, a piloted questionnaire was handed out at random times to each family attending the children's emergency department while they were waiting to be clinically assessed. 1046 families chose to participate and answered questions about their ethnicity, language preference and ability, media access and their sources of health information. The data were analysed using descriptive methods.
Results A majority of families wish to receive hospital AEHI as leaflets. Additionally, families frequently use a variety of other resources such as extended family and friends and the Internet to address their information needs. Poor literacy is a barrier to understanding in 15.6% of the study population. 73% of carers with children aged between 10 and 16 years wish their children to receive AEHI.
Conclusions The authors identified a gap in the provision of health information with respect to appropriate educational material for children and young persons, for families with poor literacy skills and those with language barriers.
Statistics from Altmetric.com
Introduction
Parents and health professionals agree that enhancing the provision of health information would contribute to improvement in child health.1 2 More data are warranted to support the development of educational interventions targeted towards the families' requirements and to ensure further empowerment of families.
Consultation with health service users is a national priority; the National Health Service (NHS) Plan 2000 suggested that patient surveys should be conducted in order to help services become more patient-centred3; the third national emergency department (ED) survey by the Healthcare Commission supports this.4 The government expressed a clear intention to put information at the centre of health5 recommending that advice leaflets containing additional educational health information (AEHI) for carers and children should be available for a range of conditions in the paediatric ED.6 It is recognised that AEHI, rather than verbal medical advice only, should be an integral part of the patient's journey3 since the provision of both written and verbal instructions ensures better understanding of how to manage care issues following hospital discharge.7 8 It had been acknowledged that there was inadequate provision.5 8
What is already known on this topic
▶ There is a need for increased provision of additional health information for patients.
▶ Provision of both written and verbal instructions lead to better parental understanding of the care needed rather than verbal instructions alone.
▶ Parents and health professionals believe that overall child health could be further improved by enhancing health education in child care.
What this study adds
▶ Families use a variety of sources to address their health information requirements.
▶ A significant number of families with insuffi cient language and/or literacy skills indicates the need for provision of AEHI via non-written audiovisual media.
▶ Families want the provision of AEHI not only for extended carers, but also for children and young people.
In many hospitals, including the University Hospitals of Leicester (UHL) where this study was conducted, AEHI is provided mainly as educational leaflets, written in plain English, targeted at the adult population—including leaflets concerning child health. Clinical Knowledge Summaries9 and NHS Choices10 have already made advances in addressing issues surrounding and improving the content of AEHI as well as attempts to provide a common platform, since it is known that patients also turn to independent sources, such as family, friends and the Internet among others, rather than their local healthcare provider for relevant AEHI.7 11 12
Furthermore, a failure to consider a patient's cultural and linguistic issues can result in a variety of adverse consequences. These include miscommunication and poor continuity of care.13,–,16 Language preference and ability are directly linked to understanding, and poor literacy within segments of the population has resulted in suggestions to deliver information using modes other than the written format.8
At UHL, there is a commitment to uphold those recommendations given for the provision of AEHI. Part of the discharge protocol is to supply families with health information regarding the condition that necessitated the emergency consultation following their discharge. As it is unknown how this provision is perceived, whether it is delivered appropriately or meets the needs of the service user, we sought to explore the families' views on our current provision of AEHI. To achieve this we undertook a pragmatic participatory survey and gathered information on the families' cultural, linguistic and literacy background, media access, preferred source of information and views on the provision of AEHI to the extended family or to children directly.
To the best of our knowledge, such a project had not thus far been performed in a paediatric ED. This study will pilot data for future studies aimed at improving the delivery and content of health information and thus support empowerment of families to manage and understand their child's health within the context of the equality and diversity agenda (ethnicity, language, access).
Objectives
The objectives of our study were: (1) to identify parents' and carers' views towards the current provision of educational health information following discharge of their children from an emergency care service, (2) to investigate families' particular needs concerning AEHI such as language and media needs and (3) to concurrently provide future recommendations for subsequent research.
Methods
This participatory study prospectively surveyed parents/carers over a 3-month period between 11 April and 19 June 2007 in the Children's ED at the Leicester Royal Infirmary using a questionnaire designed by the research team, which included consultants in emergency medicine and paediatrics, both of whom had experience of participatory research. The questionnaire contained four sections: (1) ethnicity, language preference and ability; (2) frequency, amount and perceived usefulness of the current provision; (3) the family's media accessibility and use and (4) the respondents' desire to have AEHI provided for their children or extended family, friends or other carers.
The UHL ‘Reader Panel’ was consulted to ensure the literacy level of the questionnaire conformed to the Trust policies on plain English usage. The questionnaire was piloted over a 2-week period and revised following input from parents and carers.
In the ED, the parent/carer was approached by an attending team member upon the families' arrival and asked for their participation and then provided with the questionnaire and a brief explanation of how to complete it. Further assistance was offered if requested or if language barriers were identified. If participation was declined, no further effort was made. Every family was approached irrespective of their presenting complaint except acute emergencies.
No identifiable information was collected from the questionnaire. The attending team member was a senior medical student bound by the NHS Code of Practice on Confidentiality.
Two team members manually collated the questionnaire data using Microsoft Access, with inter-rater reliability checked via a sample of 100 questionnaires; analysis was performed using Microsoft Excel.
This local questionnaire study fulfilled the requirements of a service evaluation scheme as confirmed by written advice from COREC (Central Office for Research Ethics Committees).
Limitations of the study
This study was conducted over a 3-month period and captured only a snapshot of activity in the ED. Responses may not be representative of the whole population attending the ED or of Leicestershire. Further, no method of statistical sampling was applied, limiting the ability to test any hypotheses.
One of the most obvious biases in this study was the use of a written English-language questionnaire. Those who would have difficulty completing the form would include non-English speakers, people with low literacy levels and those with poor eyesight. We tried to overcome this limitation by having a team member present within the ED to provide help to people completing the forms, but uncertainty still remains as to whether any person was systematically excluded from this work.
This pilot survey highlights areas that need to be pursued, and we would suggest a further study focused on hard-to-reach families (illiteracy, language barrier) to gain a clear view of their information needs.
Results
A total of 1046 families responded to the questionnaire. About 99.7% of the children were 16 years of age or younger (median age 7 years 0 months). Over 90% of respondents stated that they were the main carers, and the majority of respondents were parents. Trauma was the main reason for attendance (53.6%) and medical reasons in 24.4% (others: 13.6%; no responses: 8.4%). Our sample was racially and ethnically diverse as shown in table 1.
Ethnicity within the study population
Language
In our study population 26 separate first languages were reported, English being the one most commonly spoken (76.7%). The majority stated that they are fluent in spoken and written English. However, a significant minority indicated that they could only speak English but could not read or write English very well (14.2%) or could not converse (speaking, reading or writing) in English at all (1.4%) (figure 1).

Self-reported English language ability.
More than three-quarters of carers (77.2%) would prefer AEHI to be provided in English; however, a considerable percentage (13.1%) would prefer AEHI in another language with Gujarati and Polish being the most common. Most of the children (91%) in the 10–16-year age group were fluent in English (including written), and English was preferred as the first language in 81.7% of all age groups of children.
Media and families' sources of health information
The families' access to various media platforms was high (figure 2).
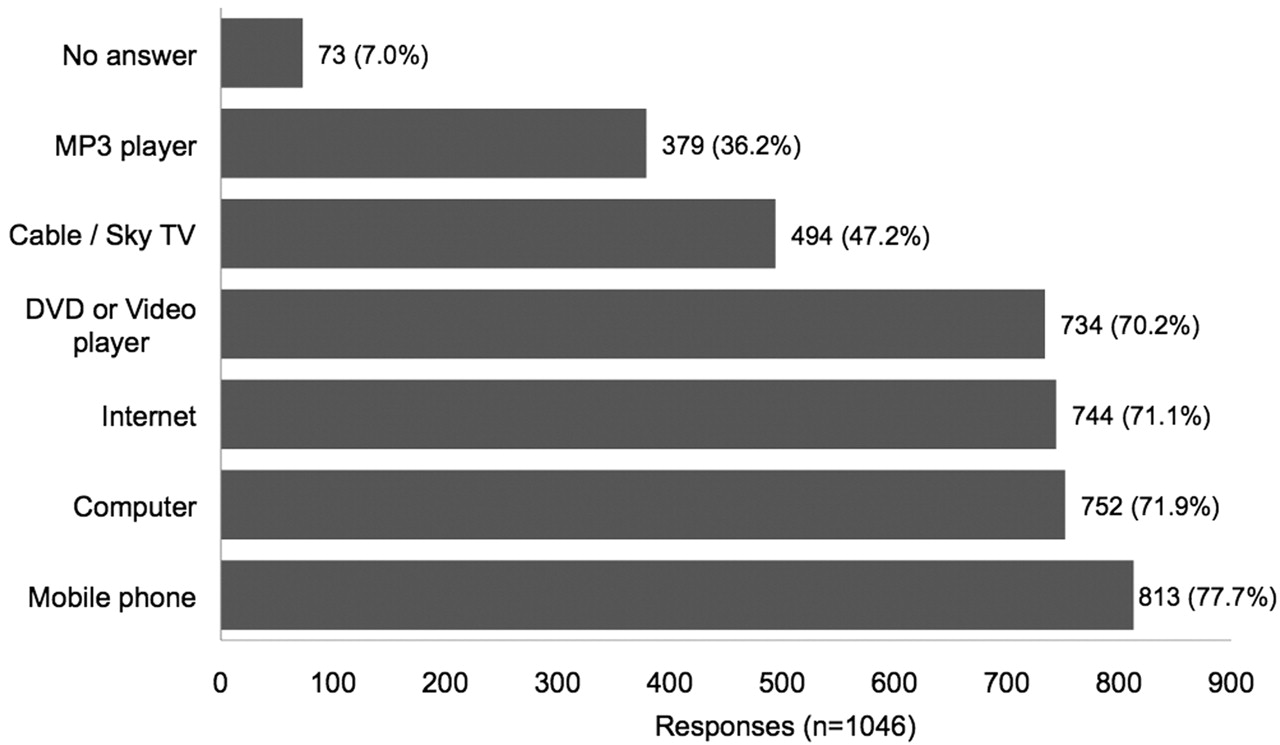
Families' media access.
We asked in what ways our respondents would like to receive AEHI and allowed multiple answers. A majority would like to continue to receive AEHI as leaflets (80.5%), nevertheless a significant number of respondents (47.9%) also named alternatives such as video/DVD (30.9%), CD or MP3 (5.8%), cable television (5.8%) and SMS text (5.4%). These numbers were comparable for the extended carers.
Most families and caregivers have sought information in addition to that provided by the doctor and their local healthcare provider. Commonly cited sources include family and friends (59.5%), the Internet (57.5%) and books (43.7%) (table 2).
Sources of additional health information*
However, over a third of the respondents (36%) indicated that they would always like to have additional information from their healthcare provider—whereby only a fifth (19%) claimed to consistently receive it. Most are happy with the amount of information they receive (56%), but still 29% would like to receive more information and 2% would like to receive less.
Families think that the provided information is useful (82%), with a majority perceiving it as very helpful (53%) and 29% perceiving it as slightly helpful. Only 3% do not think that the information is helpful at all. About 15% of respondents declined to give a response to this question.
Provision to the families' extended carers and children
Opinion was split on the provision of AEHI to the wider family and extended carers. Just short of half of the respondents (45%) felt that it would be appropriate to provide information on their child's health to them, whereas 39% felt it would not be appropriate.
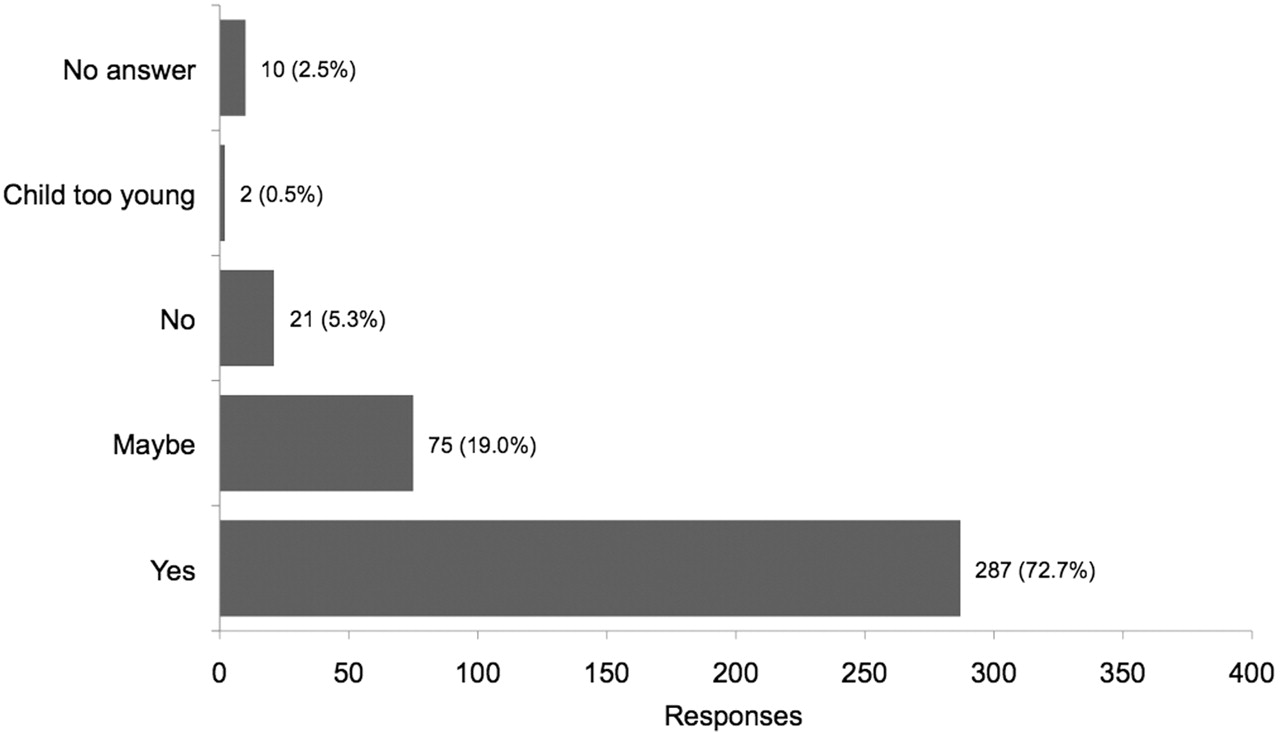
With respect to the provision for children, families indicate that they would like their children to be supplied with AEHI. In the age group between 10 and 16 years, 72% of the families or carers thought it would be useful for their children to receive additional information about their illness. A further 19% believed it might be useful to their children, making it an overall positive response in 92% (figure 3). There was no ethnic preference.

{kind=link}
{kind=link}
{kind=link}
Additional health information for children—carers' perceptions of children >10 years (n=395).
Discussion
Language: the need for a different provision for families with language barriers
A significant number of carers (14%) in our survey stated that they only speak but cannot read or write English. It is known that the comprehension of discharge information is dependent upon literacy and that understanding instructions sufficiently is key to participating in one's own care.13 14 17 18 Patients with poor language skills and low literacy scores are less likely to comprehend discharge instructions13 18 and poor comprehension is a major factor in compliance.17 Language barrier significantly influences both the provision of all care in the ED19 and patient satisfaction.13
The number of carers in our study who can only understand spoken English fits within the estimated entry-level literacy for Leicester (17%)20 and Leicestershire (7%).21 Nationally, around 24%22 of adults are estimated to be ‘functionally illiterate’, meaning they are unable to understand or employ printed information in daily life, at home, at work and/or in the community.23
Although language and culture are considered to be inseparable,14 our data indicate that one cannot correlate first-language use to ethnicity on a general basis: 58.6% of respondents indicated their ethnicity as white-British or white-Irish; however, there was a 73% response stating their first language as English. Therefore, we believe that our data support the notion that English is accepted as the common verbal platform for communication, irrespective of ethnicity.
Nevertheless, independent of ethnicity, a significant number of families with language difficulties would benefit from a different, not written, provision of AEHI. It is further recognised that recent migration of different ethnic groups may increase communication problems and therefore pose a greater need for further or different provision of AEHI.18 We believe that more studies are needed to establish how best to provide AEHI as non-written audiovisual media to families with particular language needs, while also considering their access to various forms of media.
Media and families' sources of health information
The majority of respondents, however, are fluent in English and would like to continue to receive information in the form of leaflets. Nevertheless, 47.9% are also interested in other modes of delivery. It is known from other surveys that in order to address their health information needs patients and families use sophisticated strategies to search for relevant and reliable health information using various sources.7 11 12 24 In particular, the Internet is frequently named not only in this study but also in other studies.12 25,–,27 It is known that the majority of families have Internet access and most want to receive medical information electronically.7 Further research is needed to establish how other media can be used most effectively to target these families in order to provide up-to-date, consistent and reliable health information.
Provision to the families' extended carers and children
Extended families and friends feature strongly as a source of health-related information in this survey, which supports the findings of other studies that families cross-reference information with their immediate social network as well as their general practitioner before making a health-related decision.12 24 This hints at the complexity of the decision-making process of families. Further, a significant number (44.7%) state that they would want other carers to receive child health information.
In our view, this justifies the notion that more emphasis needs to be put on the provision of consistent and reliable health information from trusted platforms for families and their wider support network in order to ensure up-to-date information and education of the whole social network.
A large number of families would like to have provision of AEHI for their children, in particular for children aged 10–16 years. Previous studies have shown that adolescents, in particular, are known to use the Internet in order to find AEHI on a variety of conditions;28,–,30 however, the quality of the online experience is often limited by their health and online literacy skills.11 CD-ROMs are also known to be a viable mean to disseminate adolescent health education programmes.31 Therefore, further studies are needed to establish the best way of delivering reliable and understandable AEHI to young people while taking their literacy, cultural and ethnic influence into account as well as their computer skills and knowledge.
Conclusions
Effort is required to provide parents with the information they need to take good care of their children.32
Our study noted that provision of AEHI with educational leaflets in English is the preferred adjunct to verbal medical advice irrespective of ethnic background. However, literate families have access to various media and use those as well as extended families and friends as advisers when dealing with health matters. There is a significant number of families with language barriers, and these families are in need of an alternative provision as are children or young attenders, particularly in the age group of 12–16 years.
Illiterate families and those with insufficient language skills as well as visually impaired attendees would benefit from the provision of non-written audiovisual media. Future studies should look into establishing the best way to ensure this provision.
Providing age-appropriate information to children and young people, educating families with reliable and consistent information from a trusted platform and further exploring the use of audiovisual media should be considered when providing future healthcare information and implementation policies.
The need to provide AEHI for children themselves should be considered seriously, and further studies should establish their health information needs, linguistic and cultural influences, preferred mode of delivery, and health and online literacy skills.
Acknowledgments
The authors would like to thank the staff in the children's ED and all the parents who participated as well as the Leicester Library for help and support.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.