Article Text

Abstract
It is well established that permanent childhood hearing impairment (PCHI) has a detrimental impact on speech and language development. The past two decades have seen the gradual introduction of universal newborn hearing screening (UNHS) programmes coupled with early intervention programmes. We review studies that have capitalised on the advent of newborn hearing screening to assess the impact of early identification of PCHI on language outcomes in deaf children. The research supports the conclusion that, in children with PCHI, newborn hearing screening and early identification lead to beneficial effects on language development, with the most consistent evidence provided for links between early identification of PCHI and positive language outcomes. Future research needs to encompass a wider range of outcomes and to assess the impact of UNHS in adolescents and young adults.
Statistics from Altmetric.com
Introduction
Permanent childhood hearing impairment (PCHI) refers to deafness in childhood that is not a temporary result of transient factors, such as middle ear infections. PCHI can be congenital or acquired, can affect a child unilaterally or bilaterally, and can range in severity from mild (25–40 dB loss), through moderate (40–70 dB loss) and severe (70–95 dB loss), to profound (95+ dB loss). PCHI affects all aspects of oral language acquisition, as a child's ability to access and extract information from the oral language models around them is compromised. Research has consistently demonstrated the detrimental impact of PCHI (the severity corresponding to the degree of hearing impairment) on speech, language and literacy development.1,–,5 Children born with PCHI are particularly vulnerable to disordered and delayed language development, as they experience auditory deprivation during a ‘sensitive period’ for language acquisition in the first few months of life.6,–,8
The decline in language learning ability and efficiency with age that characterises the sensitive period is underpinned by changes at the neural level: the absence of appropriate language input during the early sensitive period has a direct impact on the neural pathways in the brain that support language, whereas the same absence later in life does not.9 ,10 Furthermore, the structural and functional changes to the brain that result from early language deprivation can be reversed to some extent if intervention in the form of electrical stimulation of the auditory pathway by a cochlear implant is given early enough in life. The effect is lost later indicating a greater degree of plasticity in the brain during the first part of life,9,–,12 and demonstrating the need for the earliest possible intervention for children with PCHI.13,–,23
What is already known on this topic
▶ The advent of universal newborn hearing screening (UNHS) has made possible the early identification of children with permanent childhood hearing impairment.
▶ A number of research studies have capitalised on this development to explore the effects of early identification of hearing impairment on later language outcomes.
What this study adds
▶ We provide a timely review of the evidence regarding the effects of UNHS and early identification on language outcomes in children with hearing impairment.
▶ We discuss the implications of this evidence for the concept of a ‘sensitive period’ for language development, and for future research and practice.
Current UK policy is that newborn infants are screened for hearing impairment as part of a universal newborn screening (UNS) programme. As with any screening programme, the justification of the programme depends on a precise case definition. In the instance of the UK UNS programme for PCHI, a case was precisely defined as a child with bilateral PCHI of >40 dB averaged across four sound frequencies. This cut-off point was selected because of the strength of the evidence that losses of this degree or worse were linked to clinically important impairment of language development and subsequent life chances. Specifically, the average reading age of children with this degree of PCHI at age 17 years, according to estimates in both the USA and the UK, is equivalent to that of a 9 year old with normal hearing.24 ,25 Before the introduction of UNS for PCHI across the whole of the UK in 2006, infants were screened for hearing impairment using the health visitor distraction test, which refers infants for full hearing assessment if they fail to make attempts to localise sounds produced outside of their visual field.26 As this test is feasible only from approximately 7 months, many infants have already experienced several months of degraded auditory input by the time of detection. In addition, it is insensitive: Davis et al26 reported that use of this screen in the UK resulted in almost half of infants with PCHI remaining unidentified by the time they were 18 months old, and about a quarter still unidentified by the time they were 3.5 years old.
UNS for PCHI became feasible because of the development of two screening techniques, detection of transient evoked otoacoustic emissions (TEOAEs)27 and automation of auditory brainstem response (AABR) testing.28 These tests provided alternatives to the distraction test that would identify infants with PCHI more accurately, and at a much younger age.
The Wessex Trial29 aimed to determine whether a two-stage universal newborn screen comprising TEOAE detection and, in children in whom these were not detected, AABR testing was an effective way of picking up infants with PCHI at an earlier age than had previously been possible with the health visitor distraction test. This controlled trial involved teams of screeners moving between two pairs of hospitals every 4–6 months for 3 years between 1993 and 1996. This created two birth cohorts of infants, one born in a period when universal newborn hearing screening (UNHS) was available, and the other born in a period when it was not; as a result of the controlled design of the trial, the birth cohorts should have differed only in terms of their exposure to newborn screening. Screening using the health visitor distraction test continued throughout the study, but the researchers reported that, during periods when newborn screening was also available, the equivalent of an extra 62 babies with PCHI per 100 000 target population, equivalent to about 50% of the expected population prevalence of infants with PCHI of this degree, were referred before the age of 6 months compared with periods without newborn screening (number needed to treat (NNT) = 7.65). After statistical adjustment for the effect of the severity of hearing impairment, it was found that the odds of referral before 6 months were 19 (95% CI 3.2 to 111.0) times higher among babies born in a period when UNHS was available.
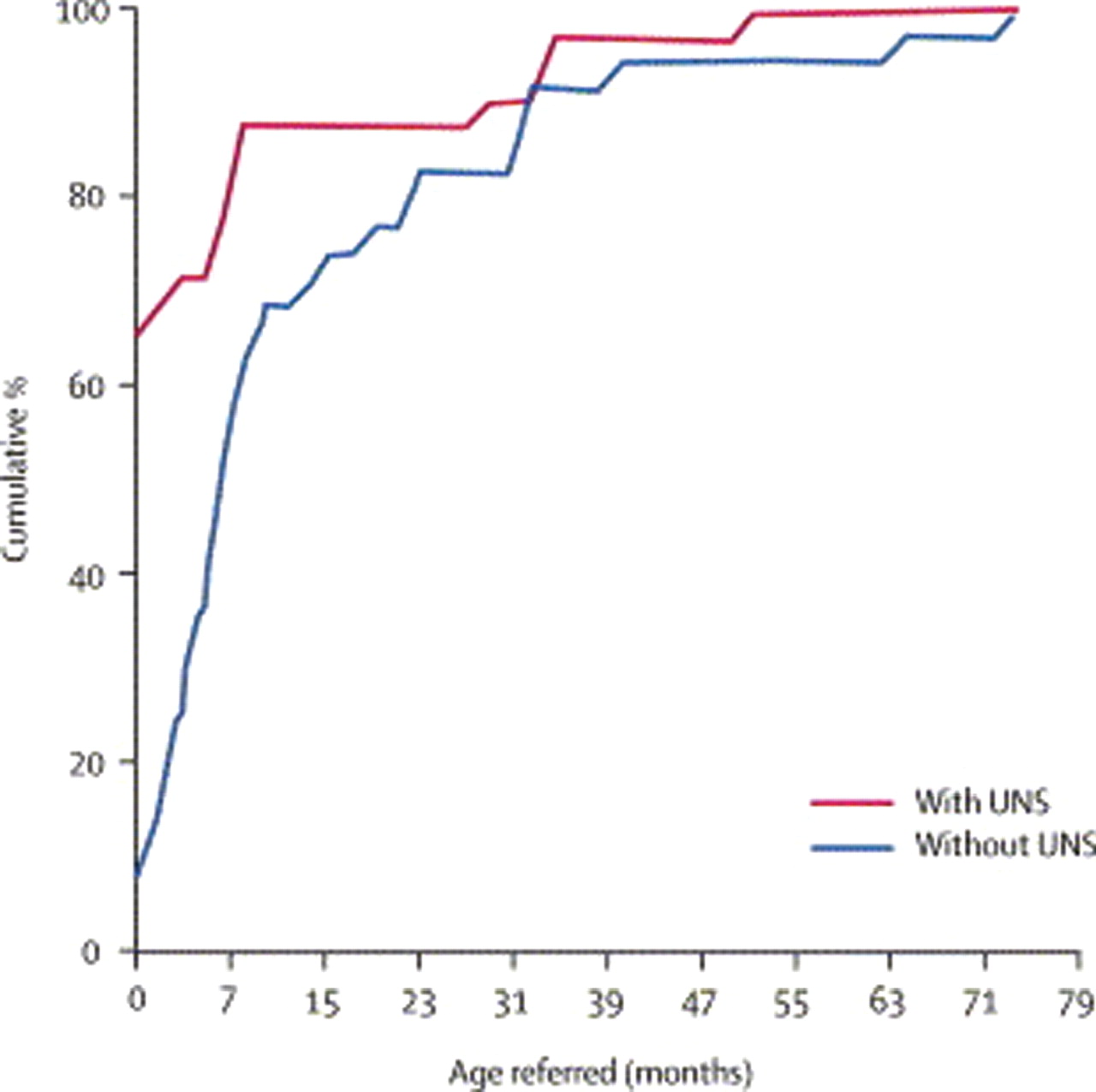
Eight years later, the researchers carried out a follow-up study of the birth cohort enrolled in the Wessex Trial. This length of follow-up period allowed the identification of all true cases of PCHI, including instances of PCHI that were missed by screening (false negatives) as well as cases of progressive PCHI.30 They found that being born in a period when newborn screening was available more than doubled the proportion of all true cases of PCHI that were referred before 6 months, with 74% of cases born in periods with UNHS referred at less than 6 months of age, compared with only 31% of cases born in periods without UNHS (figure 1).

Cumulative percentage of all known cases of bilateral permanent childhood hearing impairment >40 dB hearing level, excluding acquired cases, in the population at age 7–9 years by birth in periods with and without universal newborn screening (UNS). Reproduced with permission from Lancet, vol 366, pages 660–662, copyright 1995 by Elsevier.
The Wessex findings have been replicated in a number of programmes worldwide.31,–,38 For example, Sininger et al31 capitalised on the staggered introduction of newborn screening programmes in California to compare the average ages of screened and non-screened children with bilateral PCHI at diagnosis, fitting of amplification, and enrolment in intervention. They found that screened children were significantly younger at diagnosis (median age 25 months lower), at fitting of hearing aids (24 months lower), and at enrolment in early intervention (20 months lower). In a pre- and post-UNHS comparison, Weichbold et al35 showed that, at age 6 months, 69% of the screened group (n=164) had been diagnosed and 61% had begun intervention, while only 6% of the unscreened group (n=154) had been diagnosed and only 4% had started to receive intervention.
These studies indicate that UNHS programmes offer a more effective way of picking up children with hearing impairment early than previously used techniques such as health visitor distraction screening. In the following sections of this paper we will review evidence on the impact of UNHS and early identification of PCHI on later speech, language and literacy outcomes.
Search strategy and selection criteria
References for this review were identified through searches of PubMed using combinations of the MESH search terms ‘hearing disorders’, ‘newborn screening’ and ‘language’, with no restriction on dates of publication. Studies were selected for inclusion in the review if they provided evidence on the impact of UNHS, or of early identification of PCHI, on speech and language outcomes. The included studies were rated for quality using predefined USPSTF quality rating criteria, and quality ratings are reported. Where possible, based on the information provided in the papers, effect sizes (Cohen's d for mean comparisons) were calculated and reported to further facilitate comparison of reviewed studies.
Outcomes after UNHS
A body of work undertaken by Yoshinaga-Itano and colleagues in Colorado made an important early contribution to the evidence base regarding the impact of exposure to newborn screening for PCHI on later language outcomes.39 ,40 Superior speech and language outcomes were reported for children aged 9–61 months who had been born in hospitals that screened for PCHI (table 1).
Summary of studies that have explored the impact of UNHS on speech and language outcomes
The researchers found a mean total LQ (the quotient of each child's language age on the receptive and expressive language measures used and their chronological age, multiplied by 100) of 82 for the screened group and 64 for the unscreened group (figure 2); this placed the screened group mean within the normal range of language ability (>80).

{kind=link}
{kind=link}
Discrepancy between cognitive quotient (CQ) and language quotient (LQ) by age of identification of hearing loss for children with normal cognition. Reproduced with permission from Pediatrics, vol 102, pages 1161–1171, copyright 1998 by the American Academy of Pediatrics.
In England, Kennedy and colleagues capitalised on the experimental design of the Wessex Trial to carry out a population-based follow-up study, with the aim of establishing whether being born in a period when UNHS was available was associated with improved speech and language outcomes.41 The children from the Wessex Trial birth cohort were aged 7–9 years at the time of this follow-up study, and were combined with an additional cohort aged 6–10 years from four districts in Greater London, two of which were the only districts in this region to offer UNHS when these children were born, and two neighbouring districts which had not had UNHS programmes in place. Children who underwent UNHS showed significantly better receptive language and reading ability41 ,42 than those who were not exposed to UNHS, but differences between the two groups in terms of their expressive language and speech ability were not significant (table 1).
In the Netherlands, Korver et al43 compared developmental outcomes of children with congenital PCHI in regions that had introduced UNHS with those of children in regions that were still distraction screening. The UNHS group showed non-significant advantages relative to the distraction screened group on parent-completed measures of receptive and expressive language and number of spoken words (table 1). Conversely, the mean number of words signed was significantly higher in the distraction screened group. As with the studies of Kennedy and colleagues,41 ,42 these analyses controlled for factors that may have influenced group differences—in this case, maternal education level and age at assessment.
A Canadian study44 examined the speech and language abilities of 65 children with PCHI aged 5 years and under (26 screened as newborns, 39 not screened as newborns) and found no significant differences in performance between the screened and unscreened groups on any of the speech and language measures used (table 1), leading them to conclude that improved language skills after exposure to a newborn screening programme were ‘not demonstrable in the context of this study’. It is possible that the small number of participants recruited to the study may have rendered it statistically underpowered to detect any differences between the two groups, or that assessing the children in the first few years after they were diagnosed may not have provided sufficient scope for the long-term benefits of newborn screening on language development to manifest themselves. However, even in the studies discussed previously that had much larger sample sizes43 and that worked with older children,41 ,42 the association between birth during periods of UNHS and superior speech and language outcomes was by no means unequivocal (table 1).
The picture is further complicated by the fact that some of the studies discussed above had serious methodological limitations (as highlighted in USPSTF systematic reviews), including observational rather than experimental study design and the use in some studies of convenience rather than population-based samples, and of non-blinded assessments.38 ,45 In the more recent of the USPSTF systematic reviews, Nelson et al45 rated the study of Kennedy and colleagues41 as being ‘good quality’, but even in that study, the superiority of language ability in children born in periods with UNHS reached statistical significance only for receptive, and not for expressive language or speech, skills.
One reason for these modest effect sizes may be that being born in a period when newborn screening is available is, in practice, a somewhat indirect proxy for the variables that are actually likely to impact on speech and language ability, namely early diagnosis and subsequent early intervention. Although newborn screening undoubtedly enhances the likelihood of early diagnosis, figures provided by the authors of the studies discussed above confirm that the relationship between newborn screening and early confirmation of PCHI is not absolute. Kennedy et al41 found that 67% of their screened group of children with PCHI had their hearing impairment confirmed before 9 months of age, compared with 27% of their unscreened group, suggesting that not all screened children have their deafness diagnosed early and that not all unscreened children have it diagnosed later. Furthermore, Korver et al43 reported that being born in a period when UNHS is available is no guarantee that an infant will be screened at birth, and vice versa. This lack of a one-to-one link between newborn screening and early diagnosis may have contributed to the lack of clear findings in those studies that have explored the relationship between newborn screening and later language outcomes. Thus we will now go on to discuss studies that have looked directly at the impact of early confirmation of PCHI on language development.
Outcomes after early identification
To supplement the investigations reported above on the impact of newborn screening on language development, both Kennedy et al in England and Yoshinaga-Itano et al in the USA also examined the impact of age of confirmation of PCHI on the language outcomes of their samples41 ,42 ,46,–,48 (table 2).
Summary of studies that have explored the impact of early identification of permanent childhood hearing impairment on speech and language outcomes
In the English sample, compared with the relationship between newborn screening and later language benefit, stronger links between early confirmation and improved language outcomes were found,41 as evidenced by the larger effect sizes reported in table 2. The early confirmed group (PCHI confirmed before 9 months) showed significantly superior receptive and expressive language skills to the late confirmed group (PCHI confirmed after 9 months). A subsequent more detailed exploration of the expressive language abilities of the early and late confirmed groups through analysis of their spoken narratives revealed a more nuanced picture: early confirmation brought benefits to some aspects of expressive language, but not to other aspects46 (table 2). In terms of literacy outcomes, the benefit to word reading and reading comprehension ability that was associated with early confirmation was significant, and substantially more robust than that associated with exposure to newborn screening42 (table 2).
Yoshinaga-Itano et al47 compared the receptive and expressive language of two groups of children from the Colorado cohort described above with the groups in this study formed on the basis of whether each child's PCHI was diagnosed before or after 6 months of age rather than whether or not they were screened at birth. They found that, in those children with cognitive ability in the normal range, the early identified group were rated by their parents as having significantly better receptive and expressive language abilities than the late identified group (table 2), with this effect holding regardless of age, degree of hearing loss, socioeconomic status and primary communication mode.
Taken together, the above evidence from group comparison paradigms provides strong overall support for a beneficial effect of early identification of PCHI on later language outcomes. A study by Wake and colleagues in Australia,49 however, reported that performance on language and reading measures in 7–8-year-old children with PCHI was strongly related to the severity of their hearing impairment but not to the age at which it was diagnosed. This study used a different approach from those described previously; their analysis focused not on comparing groups but on exploring relationships between key variables using regression models. The fact that degree of hearing impairment was a much better predictor of later language outcomes than age of diagnosis in this study stands in contrast with the findings of the other studies discussed above that indicated that, at a group level, children identified earlier have superior language, even when their level of hearing impairment is taken into account. This does sound a note of caution against drawing any decisive conclusions about links between early identification and language outcomes. However, various aspects of the study of Wake et al have been identified as potential contributors to this negative effect,42 namely the inclusion of children with only mild PCHI, a relatively low ascertainment rate from the cohort of eligible participants, and very small numbers (11 cases) of children whose PCHI was identified before 6 months.
Conclusions
Our review has shown that exposure to UNHS and early identification of PCHI are associated with benefits to language development in deaf children, with more consistent evidence provided for links between early identification and positive language outcomes. The relationship between early identification and superior language outcomes is likely to be mediated by intervention: early identification must be coupled with comprehensive early intervention programmes to improve the quality of the language input for children with PCHI (eg, advice for parents on how best to support their child's communication in either the oral or manual modality, amplification using hearing aids, fitting of cochlear implants) during the first few months of life—a sensitive period for language development.50 The two studies reviewed in this paper that found benefits of ‘early’ identification on language outcomes used cut-off points for early identification of 6 months47 and 9 months41, suggesting a time window for the ability to maximally benefit from intervention following early identification that ends before the age of 1 year.
To date, all the available evidence on the impact of UNHS and early identification of PCHI on language outcomes has come from studies carried out in developed countries. In this issue, Olusanya51 provides an overview of the unique challenges and opportunities surrounding newborn hearing screening in the developing world.
Looking to the future, it is less than 20 years since truly population-based UNHS was first piloted, and, partly for this reason and partly because of the challenges of undertaking any longitudinal study over periods in excess of a decade, studies of UNHS to date have used samples of preschoolers and young children, and more rarely, children in middle childhood. Consequently, the impact of UNHS, early identification and early intervention on outcomes in deaf teenagers is not yet known. There is also a need to go beyond looking solely at speech and language skills as the benchmarks of success, and consider outcomes in deaf young people that are more directly relevant to their day-to-day lives, such as educational achievement, employment, quality of life, and—of particular importance in adolescents—social and emotional functioning.
Acknowledgments
We thank Jim Stevenson for his comments on earlier versions of this paper.
References
Footnotes
-
Funding This work was supported by the Wellcome Trust (089251).
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.