Article Text

Abstract
Objective To assess the prevalence of cardiovascular risk factors in severely obese children and adolescents.
Methods A nationwide prospective surveillance study was carried out from July 2005 to July 2007 where paediatricians were asked to report all new cases of severe obesity in 2–18-year-old children to the Dutch Paediatric Surveillance Unit. Severe obesity is defined by gender and age-dependent cut-off points for body mass index based on Dutch National Growth Studies corresponding to the adult cut-off point of 35 kg/m2. Paediatricians were asked to complete a questionnaire for every severely obese child regarding socio-demographic characteristics and cardiovascular risk factors (blood pressure, fasting blood glucose and lipids).
Results In 2005, 2006 and 2007, 94%, 87% and 87%, respectively, of paediatricians in the Netherlands responded to the monthly request from the Dutch Paediatric Surveillance Unit and 500 children with newly diagnosed severe obesity were reported. 72.6% (n=363) of paediatricians responded to a subsequent questionnaire. Cardiovascular risk factor data were available in 255/307 (83%) children who were correctly classified as severely obese. 67% had at least one cardiovascular risk factor (56% hypertension, 14% high blood glucose, 0.7% type 2 diabetes and up to 54% low HDL-cholesterol). Remarkably, 62% of severely obese children aged ≤12 years already had one or more cardiovascular risk factors.
Conclusion A high number (2/3) of severely obese children have cardiovascular risk factors. Internationally accepted criteria for defining severe obesity and guidelines for early detection and treatment of severe obesity and comorbidity are urgently needed.
Statistics from Altmetric.com
Introduction
Over the last decades the prevalence of childhood overweight and obesity has rapidly increased worldwide. In addition, the degree of obesity in children and adolescents has risen. Between 1980 and 2009, the prevalence of overweight (including obesity) in the Netherlands among 2–21-year-old boys as defined by the International Obesity Task Force (IOTF) increased from 5.1% to 13.3%, and in girls from 7.2% to 14.9%.1 ,2 In the same period the prevalence of obesity increased even more, from 0.3% to 1.8% among boys and from 0.5% to 2.2% among girls.2 This is of great concern because obesity is related to type 2 diabetes and cardiovascular disease.3 These serious comorbidities are expected to occur even more frequently in
What is already known on this topic
-
The prevalence and severity of obesity in children worldwide is still rising.
-
Obesity can cause serious comorbidity including cardiovascular disease and type 2 diabetes.
-
However, studies on comorbidity in severely obese children are scarce.
What this study adds
-
Nearly two thirds of young (≤12 years of age) severely obese children already have cardiovascular risk factors.
-
Half (50%) of young (≤12 year) severely obese children already have hypertension.
-
Up to 54% of severely obese children have low HDL-cholesterol and up to 20% have high fasting glucose.
In contrast to the situation in adults, for children it is still unclear if different categories of obesity should be distinguished and how these different categories should be defined as there are no internationally accepted criteria. Based on data from the National Health and Nutrition Examination Survey of 1999–2004, Freedman et al4 have established cut-off values for severe obesity based on the 99th percentile of body mass index (BMI) for age. However, because these data are collected in the USA, where the prevalence of obesity is much higher, these cut-off points may not be applicable to other populations.
Data on the prevalence, characteristics and consequences of severe obesity in children are important for public health policy as they give an indication of the need for early detection, timely treatment and the development of interventions for this specific group. This is important for healthcare providers and the organisation of healthcare. To gather information on the socio-demographic characteristics and comorbidity of severely obese children, we used the Dutch Paediatric Surveillance Unit which is a nationwide registration system where paediatricians are asked each month to register specific diseases.6 Comparable observational surveillance systems have also been set up in other countries.7
The aim of this study was to determine cardiovascular risk factors in children and adolescents with severe obesity diagnosed by paediatricians in the Netherlands.
Methods
From July 2005 to July 2007 all paediatricians in general hospitals in the Netherlands received a monthly request by post or email from the Dutch Paediatric Surveillance Unit to report all newly diagnosed cases of severe obesity. There are no private paediatric clinics in the Netherlands. But in each of the eight university medical centres, the head of the department of paediatrics nominated a specific contact person who was responsible for reporting to the Dutch Paediatric Surveillance Unit. All paediatricians received a protocol describing how to diagnose severe obesity in children aged 2–18 years. As no internationally accepted criteria for defining severe obesity were available, gender and age-dependent cut-off points for BMI were developed for the purposes of this study (table 1) using data from the Third Dutch National Growth Study (1980, n=41 766) and the Fourth Dutch National Growth Study (1997, n=14 500).8 ,9 Centiles linked to the adult cut-off point for severe obesity of 35 kg/m2 were constructed. This method was also used to define the internationally accepted cut-off points for overweight and obesity constructed by the IOTF where data from the Third Dutch National Growth Study were also used.1
Gender and age dependent cut-off values for body mass index (BMI; kg/m2) for severely obese children and adolescents in the Netherlands
In 2005, 2006 and 2007, 94%, 87%, and 87%, respectively, of paediatricians responded to the monthly request from the Dutch Paediatric Surveillance Unit.10 Subsequently, an anonymous questionnaire was sent to every paediatrician who reported a case. The aim of this questionnaire was to collect data on socio-demographic characteristics and BMI. In addition we requested data on cardiovascular risk factors (blood pressure, fasting blood glucose, cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides). Blood pressure was measured with an oscillometric blood pressure monitor or a sphygmomanometer. The paediatrician reported the cardiovascular risk factor values and the investigators compared the values to the cut-off points, which are given in table 2. The country of origin was noted. If the child was born outside the Netherlands, his/her country of birth was used to determine ethnicity. If the child was born in the Netherlands and the mother and/or father were born outside the Netherlands, the child's ethnicity was based on their country of birth. If both mother and father were born outside the Netherlands, the country of birth of the mother prevailed.
Cut-off points for cardiovascular risk factors
Statistical analysis
To study the influence of age on cardiovascular risk factors in severe obesity, we compared young children (≤12 years) to adolescents (>12 years) as 12 years of age is often used as the start of adolescence and is also the age when children move from primary to secondary school. Differences in age groups, gender, socio-demographic characteristics and the comorbidities of children were compared with the χ2 test or Fisher's exact test and tested with logistic regression (SPSS V.15.0). Differences between outcomes were considered to be statistically significant if p<0.05.
Results
Between July 2005 and July 2007 paediatricians reported 500 children with newly diagnosed severe obesity to the Dutch Paediatric Surveillance Unit. The response rate to the questionnaire that was subsequently sent to the paediatricians was 72.6% (n=363). One case was excluded because of double reporting and in eight cases information on weight, height or age was missing. Of the 354 remaining children, 47 (13.3%) were misclassified as they did not meet criteria for severe obesity, leaving 307 children correctly diagnosed with severe obesity (table 1). The socio-demographic characteristics of the children are shown in table 3. Overall, 161 of the 307 (52%) children were boys. Younger (≤12 year) boys were more often severely obese compared to older boys (p<0.05), while the reverse was found for girls (p<0.05). Of the severely obese children, 40% were of Turkish, Moroccan or Surinamese origin. Only one child was obese because of a medical cause (hypothalamic tumour).
Age, body mass index (BMI), country of origin and family characteristics of severely obese children
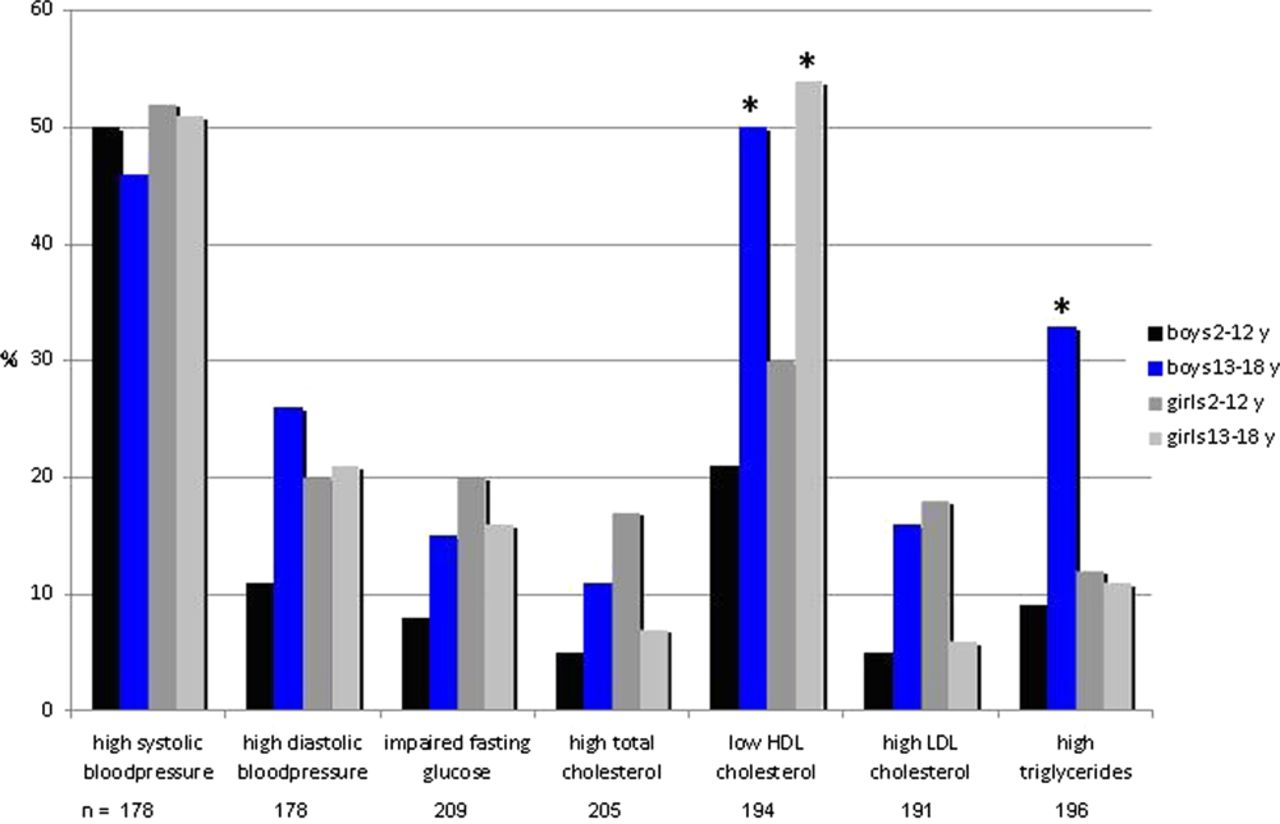
Cardiovascular risk factor data were available in 255/307 (83%) children who were correctly classified as severely obese (figure 1). At least one cardiovascular risk factor was observed in 67% and two, three and more than three risk factors were found in 17%, 8% and 2.5%, respectively. Hypertension was reported in 56% of children and at least 53% of those ≤12 years of age had high blood pressure. Cardiovascular risk factors were more frequently reported in boys aged >12 years than those ≤12 years; this was significant for high triglycerides (OR 5.12, 95% CI 1.70 to 15.48) and low HDL-cholesterol (OR 3.68, 95% CI 1.53 to 8.75). For girls low HDL-cholesterol was significantly more often observed in those aged >12 years as compared to younger girls (OR 2.71, 95% CI 1.14 to 6.41). In the older age group, elevated levels of triglycerides were more often observed in boys compared to girls (OR 3.71, 95% CI 1.30 to 10.61). Impaired fasting glucose according to the criteria of the American Diabetes Association occurred in 14% of all children and type 2 diabetes was found in two children. Both were in the older age group. There was no significant difference in cardiovascular risk factors between children of Dutch and non-Dutch origin with the exception of diastolic blood pressure which was higher in Dutch compared with non-Dutch boys (OR 3.48, 95% CI 1.08 to 11.2).
{kind=link}
Prevalence of cardiovascular risk factors in severely obese children according to gender and age group. *p<0.05, older versus younger children.
Discussion
Overall, 67% of severely obese children and adolescents diagnosed in a nationwide prospective observational surveillance study among paediatricians in the Netherlands had at least one cardiovascular risk factor. Remarkably, 62% of severely obese children ≤12 years of age already had one or more cardiovascular risk factors. The most frequently reported cardiovascular risk factor was hypertension. This is of clinical relevance given the expanding worldwide epidemic of obesity, in particular severe obesity. Studies from the USA and other countries such as Mexico and New Zealand have emphasised that the prevalence of severe obesity is rising.4 ,11 ,12 Data from the USA show that in the period 1999–2004, 4% of 2–19-year-old children were already severely obese according to the 99th percentile of BMI-for-age.13
To the best of our knowledge, this is the first population-based study to use a nationwide paediatric registration system to assess the socio-demographic characteristics and cardiovascular risk factors of children with severe obesity, diagnosed by paediatricians in daily practice.
In our study more young boys than young girls had severe obesity. This is in contrast to the results of a large study on the prevalence of overweight and obesity in children in the Netherlands in 2009.2 However, other studies also found slightly higher percentages of severe obesity (BMI-for-age ≥99th percentile) in boys, especially those below 12 years of age.4
Children of Turkish (14%) and Moroccan origin (8%) were over-represented among children diagnosed with severe obesity compared to the distribution of these ethnic groups in the general population in the Netherlands (3.1% and 3.6%, respectively).14 This is in line with studies that show an increased risk for obesity in these ethnic groups compared to Dutch children.15 Nearly one third of severely obese children lived with one parent, which percentage is higher than in the general population (6.7%) in the Netherlands.16
In our study a high percentage of children and adolescents with severe obesity had one or more cardiovascular risk factors. The prevalence of impaired fasting glucose in this population is worrying considering the increasing prevalence worldwide of type 2 diabetes in children and adolescents. Likewise, the high prevalence of hypertension and abnormal lipids in these children may lead to cardiovascular disease in (young) adulthood. A study from the USA reported that 84% of severely obese children aged 5–17 years had at least one cardiovascular risk factor, which is higher than found in our study (67%).4 However, in the US study lower age and gender specific cut-off points were used for triglycerides and HDL-cholesterol.
A limitation of our study is that it was restricted to children and adolescents with severe obesity diagnosed by a paediatrician. Adolescents diagnosed by internists were beyond the scope of this study. Although national guidelines recommend that children with (severe) obesity be referred to a paediatrician to check for possible comorbidity, it remains to be elucidated how many severely obese children in the general population are diagnosed and treated by general practitioners or do not visit a doctor at all. It is not clear whether and how these children differ from those not referred to paediatricians by general practitioners or referred to internists.
A further limitation of our study is that there is no consensus on the definition of severe obesity, which might explain why very few studies have reported on severely obese children. Nevertheless there is a need for experienced, specialised paediatric obesity centres for the intensive treatment of severely obese children as ambulatory programmes offered to obese children and adolescents are insufficiently effective for this specific group.17 Therefore, (inter)nationally accepted criteria are required to distinguish between obese and severely obese children. Some studies have established cut-off values based on BMI-for-age at the 99th or the 99.5th percentile.4 ,18 However, these cut-off points depend on the reference population and are therefore not internationally applicable or accepted. If we had applied the criteria of Freedman et al4 (BMI-for-age >99th percentile for children from the USA) to our data, only 84% of the 5–17-year-old children would have been classified as severely obese. In 68% of these children we would have found at least one cardiovascular risk factor and in 17%, 9% and 3%, two, three and more than three risk factors. These figures are slightly higher than those found in our study. On the other hand, if we had applied the WHO criteria using the 99th percentile of BMI-for-age, we would have classified more children and adolescents as severely obese.19
In conclusion, a high number (2/3) of severely obese children, even those <12 years of age, have cardiovascular risk factors. Internationally accepted criteria for defining severe obesity and guidelines for the early detection and treatment of severe obesity and comorbidity are urgently needed.
Acknowledgments
We would like to thank all paediatricians who collaborated in this study.
References
Footnotes
-
Contributors NvE collected the data, participated in data analysis and wrote the first draft. CR participated in data analysis and in writing the manuscript. MvdV participated in data collection and analysis. SvB participated in data analysis. OvdBS participated in designing the study and data collection. JKvH participated in writing the manuscript. RH conceived the idea, designed the study and participated in writing the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.