Article Text

Abstract
Purpose It is often assumed that prolonged time to diagnosis (TTD) for cancer negatively influences overall survival and survivorship through advanced stage disease at diagnosis. This systematic review assesses existing early diagnosis research in childhood and young adult cancer and aims to identify whether a consensus exists within the literature in relation to the terminology and methodologies used to investigate TTD in this population.
Methods Medline, Embase, the Centre for Reviews and Dissemination database and Cochrane library were searched for papers on children and young adults (0–30 years) published from 1948 to the present.
Results Of the 1665 potentially eligible citations identified, 32 papers met the inclusion criteria. The majority of work was in European (n=15) or North American (n=8) populations. Most work focused on brain tumours (n=10), retinoblastomas (n=5) and bone and soft tissue sarcomas (n=4). The majority of studies were in hospital-based settings (n=25), with only seven papers adopting a population-based setting. Summary statistics presented were mostly median TTD, the skewed distribution of the data meant comparisons between studies based on medians were difficult and combining studies within a meta-analysis was not appropriate.
Conclusions Within the childhood and young adult population, TTD for cancer varies between diagnostic groups and with age at diagnosis in the majority of studies. In order that clear conclusions can be drawn from early diagnosis research in children and young adults, specific criteria identifying circumstances in which delay has occurred should accompany a defined time line to diagnosis or treatment in every study.
- Oncology
- Epidemiology
- Health services research
- Evidence Based Medicine
Statistics from Altmetric.com
What is already known on this topic
-
Cancer in children and young adults is rare but is a major cause of mortality and morbidity in this population.
-
In the UK, 5-year survival for children, teenagers and young adults with cancer lags behind that in our major European counterparts.
-
Improving the time to diagnosis (TTD) for cancer is key to improving cancer care within the National Health Service.
What this study adds
-
There is a lack of focus to early diagnosis research and limitations in present knowledge regarding the TTD of cancer in children and young adults.
-
TTD for childhood and young adult cancer varies by diagnostic group and the associated variable relationship with survival.
-
Early diagnosis researchers should define criteria to identify the circumstances that lead to a delayed diagnosis which should be included in a model of TTD.
Introduction
Improving time to diagnosis (TTD) for cancer patients has been repeatedly highlighted as a key area for improving cancer care within the National Health Service (NHS)1–3; however, the impact of the time taken to achieve a diagnosis of cancer on patient outcomes is unclear.4 Early diagnosis research has lacked clear direction until recently, with an international consensus group publishing guidance for early diagnosis research across all age groups in 2012.5 Many of the difficulties faced by researchers in adult early diagnosis are also encountered by those working with children and young adults. However, distinct challenges are posed by the rarity and unique patterns of cancer in children and young adults, the age group which forms the focus of this paper.
To date two reviews have focused on TTD for childhood and young adult cancer. In 2007, Dang-Tan and Franco6 published a review of 23 epidemiological papers which included study populations under the age of 30. The authors provide an analysis of the factors associated with delay to diagnosis in childhood and young adult cancer, grouping factors as patient, cancer or healthcare-related.6 This review touches on the challenges of early diagnosis research but does not explore the limitations in the methodology used in the reviewed studies.6
The second review published by Brasme et al in 2012 is more extensive and identified 98 papers relating to the ‘distribution, determinants and consequences’ of TTD of paediatric cancers.7 Papers describing adults were included if at least 70% of the study population was paediatric. This review again provides an extensive analysis of the factors associated with delay, identifying and discussing some of the medico-legal issues surrounding delayed diagnosis in childhood cancers.7 Statistical methods calculating weighted means of the median and mean TTD are of debatable efficacy. Brasme et al7 provides little insight into the intrinsic limitations of the applied methodologies in early diagnosis research in children and young adults, nor is there any proposed solution to the issue of how we interpret delay and TTD.
This review will focus on how TTD in children and young adults varies by age and diagnosis. The limitations of the methods used in previous work will be explored and we aim to provide key points of consideration for early diagnosis research in children and young adults.
Methods and materials
Data search
A literature search from 1948 to May 2012 using a predefined search protocol was undertaken in Medline, EMBASE, EMBASE Classic, CRD databases, Cochrane Library, and Medline In-Process & Other Non-Indexed Citations. Citation searches, reference lists and colleague recommendations were also reviewed. One reviewer (CDL) screened each title and abstract for inclusion, and a second reviewer (MvL) checked a random sample of potential citations (20%). Concordance between reviewers was high, and differences of opinion were resolved by discussion.
Inclusion criteria
Primary research studies published in English were considered if they:
-
Focused on children and young adults (0–30years) (the upper age limit was extended to 30 to include US studies involving young adults)
-
Quantified the time between the onset of symptoms and a definitive diagnosis of cancer for at least 15 cases
-
Used diagnostic groups similar to the those listed in the International Classification of Childhood Cancer.8
Papers were excluded if they focused only on melanoma, due to inconsistency in the classification and registration of skin cancers in this study population.
Quality assessment
The methodological quality of the papers was assessed using the scoring systems outlined in Macdonald et al9 ,10 and against the Aarhus checklist.5
Data extraction
Data extracted included study type and period, published year, country, cancer type, explanatory factors, sample size and numbers excluded. Descriptive statistics extracted included range, inter-quartile range, median, mean and SD of TTD along with summary data for patient and professional intervals. We also recorded the authors’ defined study time period.
Results
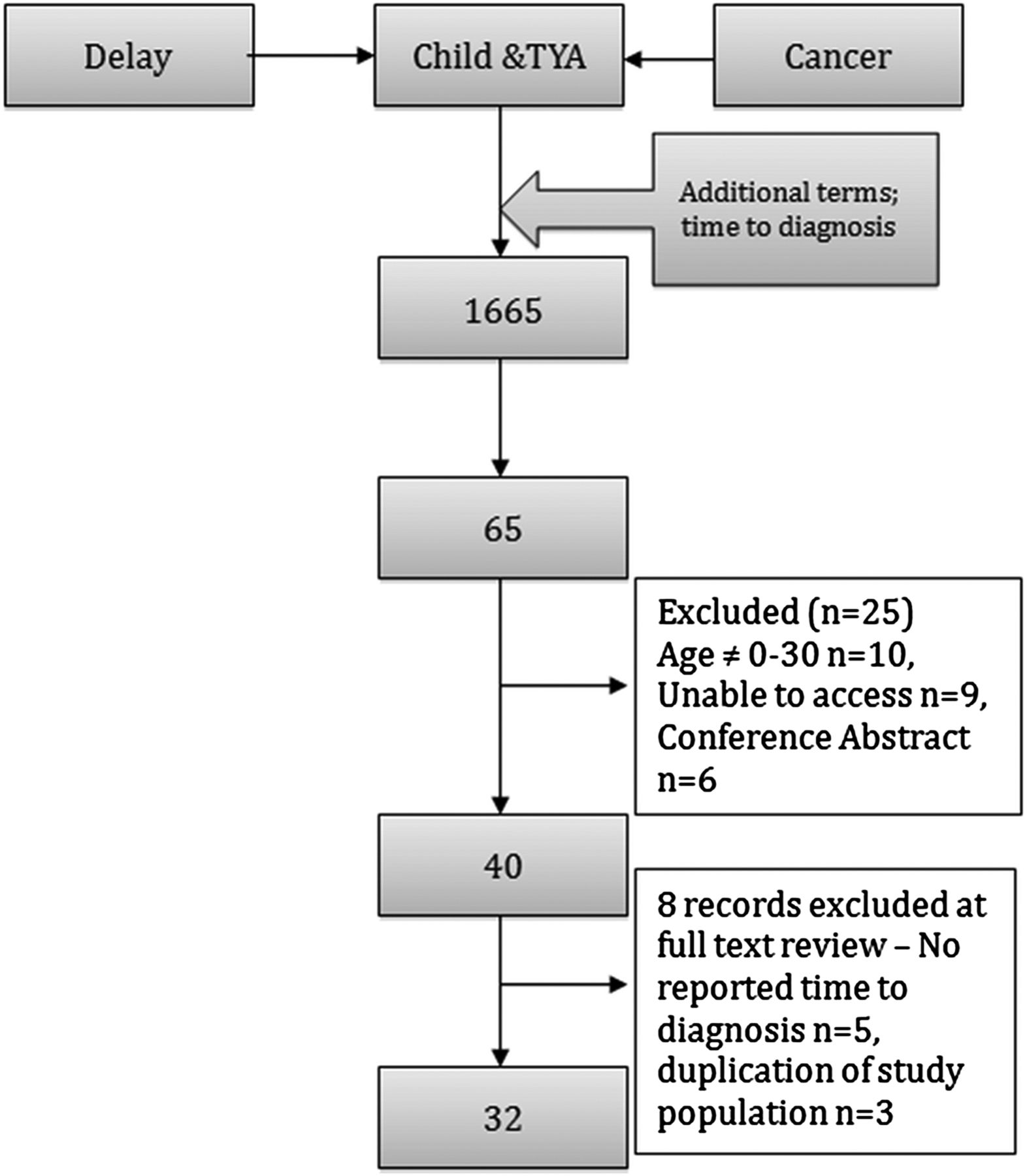
Of the initial 1665 abstracts, 65 full text articles were assessed, and 32 papers included in this review (figure 1). The country of publication varied, with papers predominantly published in Europe and North America (table 1). Eleven studies included multiple diagnostic groups,11–21 but most focused on individual groups including those with brain tumours (n=10),22–31 retinoblastoma (n=5),32–36 bone tumours or soft tissue sarcomas (n=4),37–40 central nervous system germ-cell tumours (n=1)41 and adenocarcinoma of the colon and rectum (n=1).42
Summary data presented in the papers reviewed

Flow chart for inclusion of studies in the review of the time to diagnosis in children and young adult patients. TYA, teenagers and young adults.
Quality of studies
All included papers were observational studies and data collection was predominantly retrospective by patient interview or case note/cancer registry review. The majority of studies were cross-sectional focusing on an institution or clinic, with the remainder being population-based cohort studies.
Very few studies offered a clear hypothesis and most cross-sectional studies lacked clearly defined inclusion criteria and did not deal with bias in the study design.24 ,26 ,38 ,39 All papers had moderate to low scores when the descriptive study assessment tool was applied, and a similar outcome was seen when the Aarhus checklist was applied.5 Only one study set out a clear framework of time intervals.12 The circumstances in which a delay to diagnosis became unacceptable were clearly defined by Shay et al29: if the patient encountered any of six defined circumstances prior to diagnosis the delay was considered unacceptable (figure 2).

Given the complexity of accurately identifying the date of diagnosis, a hierarchical rationale for defining the date of diagnosis of a primary cancer was not implemented or discussed. Studies of databases and case notes infrequently reported a reproducible method for data extraction.
TTD, patient interval and diagnostic interval
The time between symptom recognition and a definitive diagnosis were described as: TTD,11 ,29 delay to diagnosis,16 ,20 ,23 ,32 pre-diagnostic interval,22 ,25 ,26 ,31 lag-time14 ,15 ,17–19 ,21 ,33 and duration of symptoms.13 ,24 ,34 ,37 ,40 ,41 The term ‘symptom-interval’ was used to describe the time between symptom onset and overall TTD.30 ,38 ,39
‘Patient-interval’ (PI)5 ,11 was used to describe the time between symptom onset and first clinical presentation. Other terms used were patient delay,6 ,14 ,15 ,20 ,21 ,37 ,39 and onset of symptoms to presentation.40 Diagnostic-interval (DI) referred to the period from primary engagement with a healthcare professional to a definitive diagnosis (also referred to as doctor, physician or healthcare delay).6 ,14 ,15 ,20 ,21 ,37 ,39
Wide variation exists between diagnostic groups regarding the frequency of reported median values for TTD. Brain tumours had the most frequently reported median TTD (n=12) and hepatic tumours the least (n=1) (figure 3). A wide range of median values for TTD were reported within each diagnostic group (figure 3). TTD varied by diagnostic group, for example, there was no overlap between the reported median TTD for leukaemia and lymphoma, while renal tumours appeared to have the shortest TTD. Ten papers reported the median values for TTD, PI and DI (table 1).
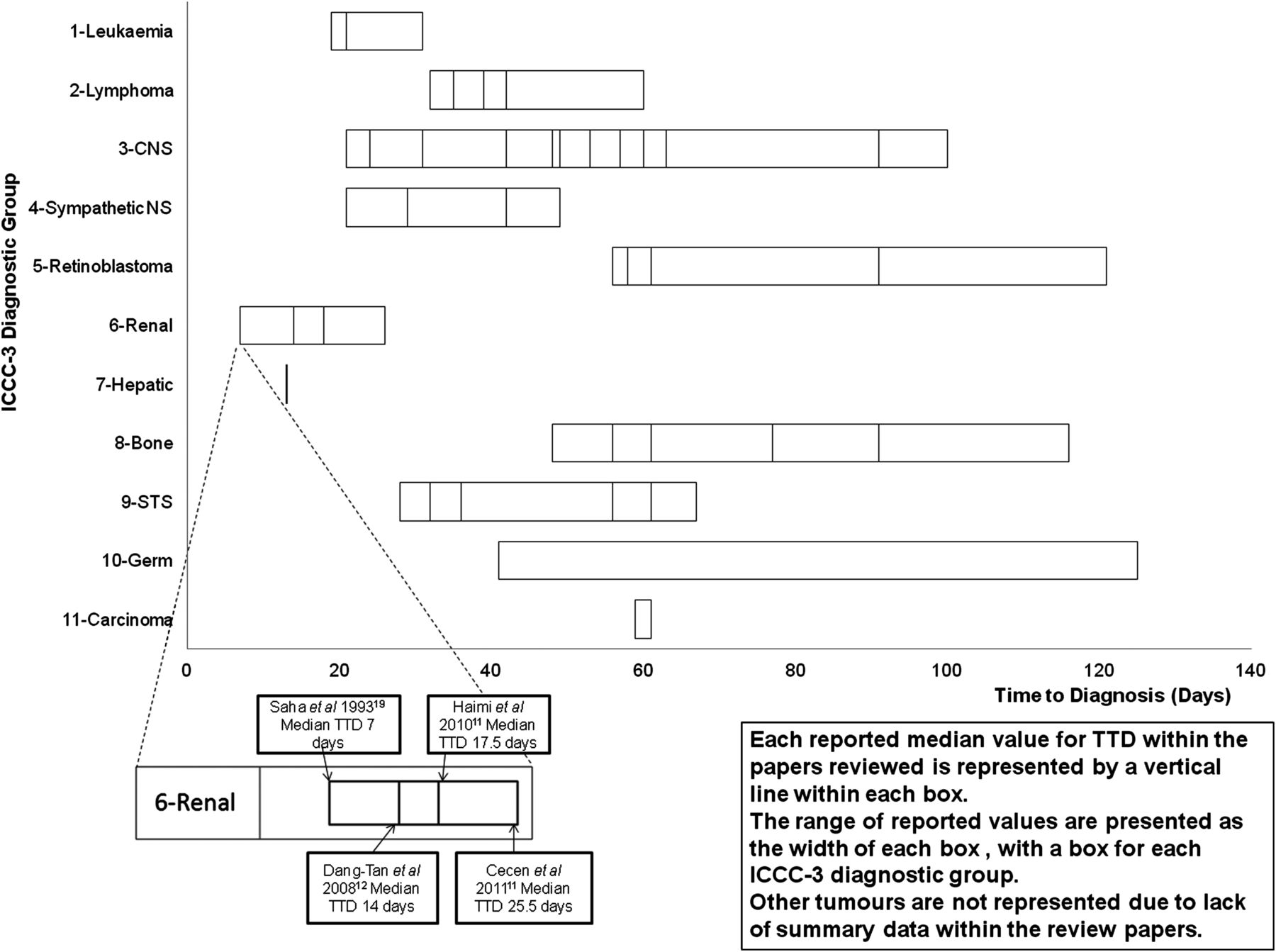
Graph of the reported medians for time to diagnosis by diagnostic group. CNS , central nervous system; ICCC-3, International Classification of Childhood Cancer, Third Edition; NS, nervous system; STS, soft tissue sarcoma; TTD, time to diagnosis.
TTD and diagnostic group
The diagnosis of bone tumours,12 ,18 brain tumours,13 ,14 ,19 germ cell tumours11 and retinoblastoma11 ,12 was associated with longer TTD compared to leukaemia12 ,13 ,17 and renal tumours (figure 3).11–13 ,19 There were significant variations by subtype, for example, medulloblastoma had a significantly shorter TTD than other brain tumours,27 Ewing's sarcoma had a longer TTD than osteosarcoma,39 and non-rhabdomyosarcoma soft tissue sarcomas had a longer TTD compared to Ewing's family soft tissue sarcomas (STS).38
TTD and age
The majority of reviewed articles included childhood and teenage populations, with seven papers including patients aged 20 years or over.14 ,17 ,18 ,38–40 ,42 The study by Martin et al17 was the only one to focus solely on teenagers and young adults (aged 15–29 years). Authors often subdivided the study population into age groups for comparison; however, there was marked variation in age divisions, which were dictated by the overall age range, by the peak incidence of a tumour or by age thresholds for certain treatments.
A longer TTD was significantly associated with older age at diagnosis in a number of studies that involved childhood and young adult bone tumours, leukaemia, lymphoma, brain tumours, retinoblastoma and soft tissue sarcoma.14 ,16 ,18 ,26 ,38 Nevertheless, no correlation between age and TTD was shown in some brain tumour studies28 ,30 or in the study focusing solely on teenagers and young adults.17
TTD and outcome
Two distinct patterns of survival emerged from the review:
-
An almost linear decrease in survival probability with increasing TTD. This was observed in the Ewing's family of soft tissue sarcomas.38
-
A non-linear relationship showing an initial fall in survival probability to a nadir at a relatively short TTD, followed by an increasing survival probability with increasing TTD. This was observed in children and young adults with brain26 and non-rhabdomyosarcoma38 tumours, a contrast to adult colorectal cancer populations.43
-
No significant difference in survival with increasing TTD was observed in the bone sarcoma population.39
Summary statistics
The summary statistics presented varied between studies (table 1). The median and range were often presented for TTD, PI and DI due to extreme outliers and positively skewed distributions. However, the inter-quartile ranges were rarely cited. Furthermore, only four of 32 papers presented the mean, median, range and SD in combination.14 ,15 ,32 ,34
Discussion
The overwhelming opinion among patients, clinicians and public health professionals is that improving TTD for childhood and young adult cancers will impact positively upon survival and survivorship. However, the conclusions drawn from early diagnosis research in children and young adults to date are far from clear. This review highlights some limitations in this research area. The vast majority of publications lack a theoretical framework and consequently the definitions used for key time intervals and milestones are neither robust nor reproducible.
The term ‘delay’ is used in the majority of articles, most frequently to describe an unqualified period of time between symptom onset and definitive diagnosis.12 ,14 ,16 ,20 ,21 ,26 ,32–34 ,36 When authors attempted to qualify the point from which a delay becomes unacceptable or excessive, they often used an arbitrary time point defined by their observations41 or the median delay value for the study population.16 ,40 Given the negative connotations of the term ‘delay’, a set of defined criteria should be outlined at the start of the study to identify unacceptable circumstances during which a delay is experienced. Shay et al29 and the National Patient Safety Agency defined criteria for delay in a thematic review of the delayed diagnosis of cancer (figure 2).44 Such criteria should be accompanied by a clear model of time intervals to be studied and hierarchies for the identification of major time points (similar to the hierarchy for defining the date of diagnosis issued by the European Network of Cancer Registries).45
An outline of milestones to aid TTD research has been developed based on this review (figure 4). The terms PI, DI and TTD are purely descriptive and infer nothing about the significance or modifiability in duration of time lapse within each period. ‘Delay’ describes a variable time within the PI, DI or TTD that occurs if the outlined criteria for delay are met. More extensive models of pathways to treatment and milestones in early diagnosis research are outlined by Weller et al.5 These should be used as the theoretical models from which early diagnosis research can develop.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time line for the diagnosis of cancer.
An older age at diagnosis has been consistently associated with prolonged TTD. Most authors hypothesise that as children become young adults they are subject to reduced parental surveillance, have limited knowledge of their own physical health and face hurdles when accessing healthcare.14 ,46 Childhood and young adult patients would appear to have a longer TTD than older adults for certain cancers such as bone tumours, possibly due to the rarity of such tumours in this population and a resulting lack of awareness of the diagnosis amongst general healthcare professionals.47
The relationship between TTD and outcome is also unclear. Differing patterns of survival with increasing TTD were reported across diagnostic groups, most notably in brain, bone and STS populations.24 ,38 ,39 The peaks and troughs in survival outlined earlier may signify the presence of other factors that have a stronger influence on outcome, such as tumour biology or response to treatment.26 Analysis comparing TTD in the low-grade glioma population and the medulloblastoma population concluded that tumour biology is “dominant and overwhelms any opposing effect on survival of a delay in diagnosis”.26
Overall survival is not the only measure of outcome relevant to early diagnosis; other measures include recurrence, quality of life, treatment late effects and survivorship.48 In the UK, 5-year survival for retinoblastoma between 2001 and 2005 was nearly 100%,49 yet the median TTD for this group of patients was among the longest.49 Furthermore, studies consistently showed a significant association between increasing TTD and other poor outcome measures including advanced localised or metastatic disease and increased treatment burden.32–35 Improving TTD would therefore aim to impact on survivorship by reducing the treatment burden from chemotherapy, improving visual function and long-term quality of life.
Limitations
Potential language bias was caused through a lack of scope to access and translate foreign language papers. Search strategies did not identify papers that considered prognostic factors or quantified TTD, PI or DI within the main text of the paper but not in the abstract. Publication bias has not been addressed in this study; however, we believe the effect of this is minimised due to the wide range of results obtained between and within diagnostic groups. Several other issues were observed in our study which were not included due to space restrictions, such as the impact of socio-economic status, healthcare provision and disease related factors on the TTD.
The limitations found from the literature review are summarised as follows:
-
Little consistency in the terminology of TTD and the heterogeneity of research methods made comparisons between studies difficult.
-
Summary data reported were inconsistent and incomplete, leading to difficulty interpreting comparative data. This is important as the data are skewed and contain extreme outliers.
-
There was marked variability in reporting the association between TTD and outcome.
Conclusion
TTD for cancer in children and young adults varied widely between diagnostic groups. A clearly defined theoretical framework and robust, reproducible methodology are required to describe and report TTD in the childhood and young adult population. These factors will facilitate meta-analysis of early diagnosis research in a rare group of diseases. The relationship between PI and diagnostic interval and their influence on TTD are poorly understood and require further research. Due to the negative connotations of the terms ‘delay’, early diagnosis researchers must define the circumstances in which the TTD becomes unacceptable. This review highlights examples of existing criteria for defining delays in diagnosis. A prolonged TTD may not have a detrimental effect on outcome in all cases of childhood and young adult cancer. The TTD described in relation to tumour diagnosis, grade or biology may give a more complete indication of the impact of TTD on outcomes.
Acknowledgments
We acknowledge the help received from Professor Ian Lewis in setting up this research.
References
Footnotes
-
Contibutors CDL jointly conceived the review with RGF, SP and SEK as part of a wider MD project, all of whom helped significantly with the redrafting of the article for submission. MvL reviewed a sample of the literature and helped refine the list of included articles and was also involved in redrafting the article. RP provided a significant level of guidance on the review design, including data analysis, and also helped redraft the article. CDL was responsible for the review design, the literature search, data extraction and analysis, writing the first draft and subsequent redrafting.
-
Funding This work has been made possible through the funding of a research fellowship by the Jeremy Neill Allen Fellowship awarded by the Leeds Teaching Hospitals Charitable Foundation (Ref No. 9R01/1101).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.