Article Text

Abstract
Background Children receiving chemotherapy for acute lymphoblastic leukaemia (ALL) may be susceptible to skeletal morbidity.
Aim To determine the incidence and risk factors for skeletal morbidity in ALL children.
Patients and methods The medical records of all (n=186, boys=110) children presenting to a single centre with ALL between 1997 and 2007 and treated on UKALL97, UKALL97/01 or UKALL2003 were studied. Skeletal morbidity included musculoskeletal pain, fractures and osteonecrosis (ON). Musculoskeletal pain was classified as any event of limb pain, muscle pain, joint symptoms or back pain that required radiological examination. Fractures and ON were confirmed by x-rays and MRI, respectively.
Results Skeletal morbidity, presenting as musculoskeletal pain, fractures or ON were reported in 88 (47%) children of whom 56 (63%) were boys. Of 88 children, 49 (55%), 27 (30%) and 18 (20%) had musculoskeletal pain, fracture(s) or ON, respectively. 6 (7%) had fractures and ON. The median (10th, 90th centiles) age at diagnosis of ALL in those children without skeletal morbidity was 3.9 (1.4–12) years which was lower than in those with skeletal morbidity at 8.2 (2.2–14.3) years (p<0.00001, 95% CI 1.7 to 4.4). Children with ALL diagnosed over 8 years of age were at increased risk of developing fracture(s) (p=0.01, OR=2.9, 95% CI 1.3 to 6.5) whereas the risk of ON was higher in those who were diagnosed after 9 years of age (p<0.0001, OR=15, 95% CI 4.1 to 54.4). There was no sex difference in the incidence of skeletal complications. Children who received Dexamethasone had a higher incidence of skeletal morbidity than those who were treated with Prednisolone (p=0.027, OR=2.6, 95% CI 1.1 to 5.9).
Conclusion The occurrence of skeletal morbidity in ALL children may be influenced by age and the type of glucocorticoids. These findings may facilitate the development of effective bone protective intervention.
Statistics from Altmetric.com
Acute lymphoblastic leukaemia (ALL) is the commonest childhood cancer with a 5-year survival rate of over 80%.1 With the sustained improvement in survival rates, attention has been directed towards recognition and prevention of disease and treatment-related morbidity. Over the last two decades, skeletal morbidity is increasingly being recognised as a major problem in these children and may occur at diagnosis as well as during or following treatment.2 It may present as fractures, osteonecrosis (ON), pain or loss of mobility and deformity, with resultant adverse consequences on quality of life. A clear understanding of this group of complications may enable the institution of rational strategies that can improve bone health. While the aetiology of skeletal morbidity in this group of children may be multi-factorial and include the disease itself, chemotherapy, poor nutrition, mineral abnormalities, physical inactivity, low lean mass and ongoing inflammation,3 glucocorticoid therapy is well known to be associated with poor skeletal development in many clinical conditions in childhood and may play a vital contributory role in the skeletal morbidity in children receiving chemotherapy for ALL.4 In ALL, glucocorticoid therapy, as well as other intensive therapy, is associated with abnormalities of markers of bone turnover that favour bone resorption,5 and these abnormalities may be more pronounced in those children who receive Dexamethasone rather than Prednisolone.6 An increased predisposition towards skeletal morbidity in children receiving Dexamethasone has been observed by Strauss et al7 but not by other investigators.8 9 Over the last decade, the chemotherapy protocols for the treatment of ALL in the UK have evolved from a clinical trial where children received either Dexamethasone or Prednisolone (UKALL97/01) to solely Dexamethasone (UKALL2003). The aim of the current study was to perform a retrospective survey of the extent of skeletal morbidity encountered in children treated on these protocols and to investigate the relationship of this morbidity to therapy and patient-related factors.
What is already known on this topic
▶. Skeletal morbidity is a known short-term complication of chemotherapy for acute lymphoblastic leukaemia.
▶. Risk factors for skeletal morbidity may include glucocorticoid therapy and adolescence
What this study adds
▶. Children who suffer from osteonecrosis are significantly older than those who suffer from fractures
▶. Children treated with Dexamethasone had a higher incidence of skeletal morbidity than those treated with Prednisolone.
Methods
Patients
The medical records of 186 consecutive patients (boys, 110) who were diagnosed between January 1997 and December 2007 to the Royal Hospital for Sick Children in Glasgow with a diagnosis of ALL were examined for information regarding skeletal morbidity including musculoskeletal pain, fractures and ON until 6 months after the last diagnosis. The median follow-up for boys and girls was 5.7 (1.9–10) and 5.9 (2.3–10) years, respectively (NS). The median (10th, 90th centiles) age at presentation for the whole cohort was 5.3 (1.7–13.7) years, and there was no significant difference between the median age at diagnosis of boys at 5.6 (1.7–12.6) years and girls at 5.3 (1.7–13.7) years. Skeletal morbidity included musculoskeletal pain, fractures and ON. Musculoskeletal pain was defined as any event of limb pain, joint and muscle symptoms or back pain that required diagnostic imaging. Fractures were confirmed by x-ray whereas ON was confirmed by XR and MRI imaging. Location of skeletal morbidity, sex distribution, age and details of chemotherapy at presentation of skeletal morbidity were also recorded. Of the 186 children, 12 did not survive and 10 children proceeded to bone marrow transplantation.
Between 1997 and 2001, children were randomised to receive Prednisolone or Dexamethasone according to UKALL97. However, Dexamethasone was the steroid administered to all patients during intensification blocks of therapy on this protocol irrespective of steroid randomisation. From 2001 to 2003, all children received Dexamethasone as glucocorticoid therapy according to UKALL97/01, and from 2003 onwards, children were treated with Dexamethasone as part of UKALL2003. Of the 186 children, 31 were randomised to receive Prednisolone; 6 were treated by high-risk ALL (HRL); 2 were treated by infant leukaemia regimen; 82 received Dexamethasone as part of UKALL97 or 97/01 and 65 (26, 10, 28 regimen A, B and C, respectively, and 1 treated by infant leukaemia regimen) children received Dexamethasone as part of UKALL2003. Therefore, the total number of children who were treated with Dexamethasone was 146. Dexamethasone was converted into Prednisolone equivalence by multiplying its dose by a conversion factor of 6.67 based on the relative anti-inflammatory responses. The total dose of glucocorticoids for both protocols was calculated as Prednisolone and Prednisolone equivalence (table 1). The total amount of glucocorticoids was lower in the Prednisolone treated children than the Prednisolone-equivalence dose (Dexamethasone treated children) in the UKALL97/01 (table 1). Comparing steroid doses between the UKALL97/01 and UKALL2003 protocols shows that the calculated doses of Prednisolone in the UKALL97/01 was slightly lower than the doses of Prednisolone-Equivalent (Dexamethasone) in the UKALL2003. Boys had a longer duration of glucocorticoids and, therefore, a higher cumulative dose of glucocorticoids.
The cumulative dose of Pred and/or Dex in the UKALL97, UKALL97/01 and the UKALL 2003 protocol.
Statistical analysis
Results are presented as medians and 10th and 90th centiles. Statistical analysis was performed with XL STAT V.7.0 (Addinsoft, Paris, France), Minitab15 (Minitab, Coventry, UK) and MS Excel 2003 (Microsoft, Redmond, Washington, USA). Difference between groups was assessed using the Mann–Whitney U test and the Pearson Correlation, logistic regression and the χ2 test were employed to assess any association between groups of variables. The study was approved by the local Ethics Committee as an audit of a standard treatment protocol.
Results
Skeletal morbidity
Skeletal morbidity, as musculoskeletal pain alone, fracture(s) or ON were reported in 88 (47%) of the 186 children, and 56 (63%) were boys (fig 1). Of the 88 children, musculoskeletal pain alone, that is, without any evidence of fracture(s) or ON was present in 49 (55%) of whom 29 (59%) were boys. Fractures alone occurred in 21 (23.8%) of whom 16 (76%) were boys and ON alone in 12 (13%) of whom 7 (58%) were boys. A further six (6.8%) children had fractures and ON. Therefore, the total incidence of musculoskeletal pain, fractures and ON was 49/186 (26%) 27/186 (14.5%) and 18/186 (9.7%), respectively.

The distribution of skeletal morbidity by protocol and distribution of children who suffered from musculoskeletal pain only, fractures, osteonecrosis (ON) or a combination of ON and fractures. (A) Each skeletal morbidity in the whole cohort who received five different protocols (UKALL97 and UKALL97/01 (n=113), UKALL2003 (n=64), high-risk acute lymphoblastic leukaemia (n=6) and infant leukaemia regimen (n=3)). (B) The distribution of each skeletal morbidity in those children who were treated by Prednisolone (UKALL97). (C) The distribution of each skeletal morbidity in those children who were treated with Dexamethasone (UKALL97/01). (D) The distribution of each skeletal morbidity in those children who were treated by Dexamethasone (UKALL 2003).
Timing and age
While the median age at diagnosis of ALL was 5.3 (1.7–13.6) years for the whole cohort (fig 2), the median age at diagnosis of those children without skeletal morbidity was 3.9 (1.5–12) years and lower than in those with skeletal morbidity (8 (2.2–14.3) years; p<0.00001, 95% CI 1.7 to 4.4). The median age at diagnosis of ALL in those children with musculoskeletal pain was 6.4 (2–14) years. The median age at diagnosis of ALL in those children with a fracture was 8.3 (2.1–13.8) years and lower than that for children with ON at 12.2 (6.8–14.9) years (p=0.0077, 95% CI 1.1 to 6.3). Furthermore, the median age of children at diagnosis of fracture(s) was 10 (4.8–16) years and at diagnosis of ON was 13.8 (9.6–18) years (p=0.002, 95% CI 1.6 to 6.6). The first fracture occurred after a median duration of chemotherapy of 18.7 (4.3–35) months whereas the first event of ON occurred at a median of 29 (8.8–48) months after the start of chemotherapy (NS). Six (33%) out of the 18 children with ON had total body irradiation (TBI) and the remaining 12 (67%) were just treated with standard anti-leukaemia chemotherapy (SAC). The median time from diagnosis of ALL to first diagnosis of ON was 17 (3–49) and 46 (29–73) months in the SAC and TBI, respectively (p=0.02, 95% CI 8.0 to 39.0). Children >8 years at diagnosis had a significant (p=0.01, OR=2.9, 95% CI 1.3 to 6.5) risk of developing fractures whereas the risk of ON was seen in children >9 years at diagnosis (p<0.0001, OR=15.9, 95% CI 4.14 to 54.37).

Median, 25th, 75th centiles, minimum and maximum values for age at (A) diagnosis of acute lymphoblastic leukaemia (ALL) for the whole group (B) diagnosis of ALL for those who had no skeletal morbidity, (C) diagnosis of ALL for those who had skeletal morbidity, (D) diagnosis of ALL who had musculoskeletal pain, (E) diagnosis of ALL who had fractures and (F) diagnosis of ALL who had osteonecrosis (ON) (G) diagnosis of fractures (H) diagnosis of ON. *p=0.01, **p<0.0001.
Sex distribution
No sex differences were observed in any form of skeletal morbidity. The incidence of musculoskeletal pain in boys and girls was almost equal 29/110 (26%) and 20/76 (26%), respectively, whereas the incidence of fractures in boys at 21/110 (19%) was over twice compared to girls at 6/76 (8%). In addition, there was no difference in the incidence of ON between boys at 11/110 (10%) and girls at 7/76 (9%). The median age at time of fracture(s) in girls was 10.2 (3.7–12.4) years which was almost similar to boys at 9.9 (5.2–16.2) years. The median age at diagnosis of ON in boys occurred at 14.6 (10.6–18.5) years and in girls at 13.1 years of age (9.6–15.8) (NS).
Glucocorticoids
Children treated with Prednisolone had a lower incidence of skeletal morbidity than those treated with Dexamethasone by about 2.6 times (p=0.027, 95% CI 1.1 to 5.9). Musculoskeletal pain alone as a feature of skeletal morbidity occurred in 49 children in total. This group consisted of 6/31 (19%) children who were treated with Prednisolone and 40/146 children (27%) treated with Dexamethasone; 3/6 children (50%) were treated with HRL, and no skeletal morbidity was observed in children who received the infant protocols (2). The incidence of fractures in those children who were treated with Prednisolone and Dexamethasone was 3/31 (9.6%) and 24/146 (16%), respectively. The incidence of ON in those children who were treated with Dexamethasone was higher at 16/146 (11%) than in those children who were treated with Prednisolone and HRL regimen at 1/29 (3.5%).
Site of skeletal morbidity
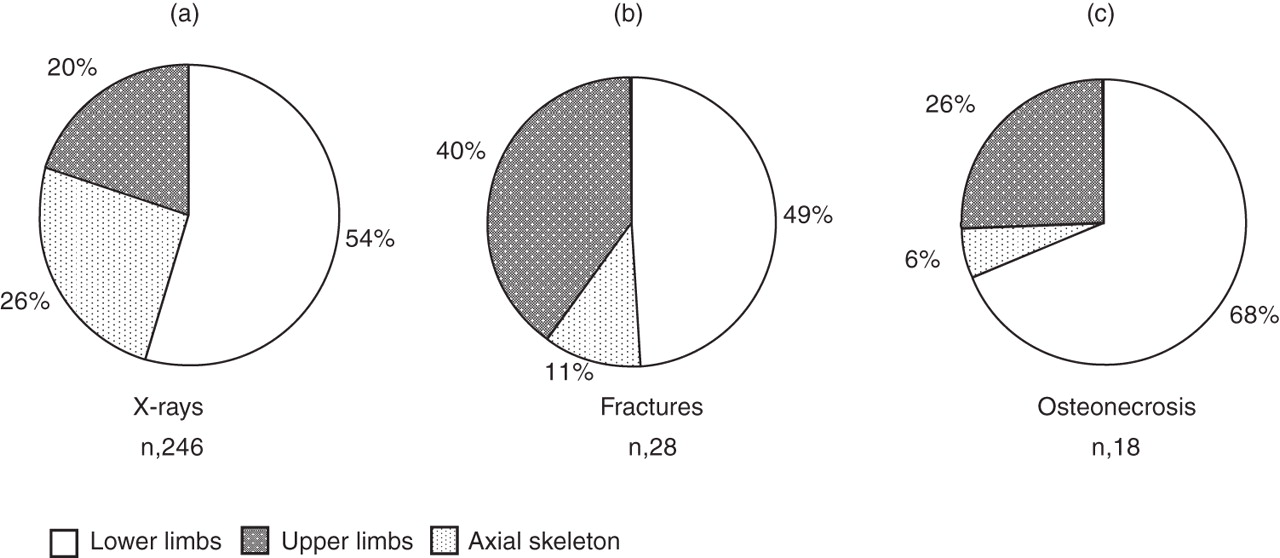
The 90 children with complaints of skeletal morbidity had 246 x-ray examinations. In order of frequency, 134 (54%) examinations were performed in lower limbs (foot, tibiae, fibulae, knees and femora), 63 (26%) in axial bone (spine and pelvis) and the remaining 49 (11%) in the upper limbs (hands, radii, ulnae, humeri; fig 3). In the 28 cases who had fractures, 16 (57%) children had a single fracture, 7 (25%) children had two fractures and the remaining 5 (18%) had more than two fractures. Of a total of 43 fractures, 22 (51%) occurred in the lower limbs of which 10 occurred in the feet. Fractures in the upper limbs occurred in 17 (40%) cases of which 14 occurred in the hands (n=3) and forearms (n=11). In the remaining four (9%) cases, fractures occurred in the spine. Among the 35 cases of ON, 13, 9 and 7 cases occurred in the knees, hips and shoulders, respectively. ON was multifocal in 10/18 (55%) children who were affected.
{kind=link}
{kind=link}
{kind=link}
The proportion of sites (lower limbs, upper limbs and axial skeleton) affected by skeletal morbidity as judged by (A) x-rays performed for musculoskeletal pain, (B) the distribution of fractures and (C) the distribution of osteonecrosis.
Discussion
This current review represents the largest systematic single centre study of skeletal morbidity in children who received chemotherapy for ALL in the UK. By defining skeletal morbidity as those events of musculoskeletal pain that required radiological imaging our study may have underestimated the incidence of skeletal morbidity. However, despite this limitation, the study showed that musculoskeletal pain was sufficiently severe to require imaging in about half of children with ALL. In about half of this group of children with musculoskeletal pain, there were no abnormal findings on imaging, and in the other half, there was clear evidence of a fracture or ON. Thus, a quarter of children had skeletal morbidity which was confirmed on imaging. These results show a markedly higher incidence of skeletal morbidity than those reported by Mitchell et al10 who reported the incidence of osteopenia and ON in over 1600 children with leukaemia who received Dexamethasone or Prednisolone in ALL97 and ALL99. However, our results are generally similar to those reported for fractures and ON by previous investigators.7 8 11,–,14 Trabecular bone, as found in the axial skeleton, is more sensitive to glucocorticoid induced osteoporosis.15 However, the current study, as well as previous studies, tend to suggest that fractures are more likely to be identified in the appendicular skeleton in children receiving ALL chemotherapy. This observation may represent a selection bias as diagnostic imaging may only have been undertaken in those children where there was clinical concern. Given that vertebral fractures can be difficult to diagnose in children and that symptoms may overlap with general muscular and postural pain,16 it is possible that fractures in the axial skeleton may not be identified without systematic radiological screening of the spine. Detailed vertebral morphometry studies performed recently in 186 children with ALL suggested that 16% may have a vertebral deformity consistent with a compression fracture.17 However, these vertebral compressions were assessed within 30 days of diagnosis and could be viewed as presenting features rather than complications of therapy.
Our finding of a clear association of fractures with Dexamethasone administration has only been described by one other group of investigators.7 Glucocorticoids are an essential component of treatment for ALL. Compared to Prednisolone, Dexamethasone has enhanced lymphoblast cytotoxicity and penetration of the central nervous system, even at a dosage that is equipotent for glucocorticoid effect. This finding has led to the substitution of Dexamethasone for Prednisolone in the treatment of ALL and to improved event-free and overall survival.10 However, Dexamethasone is associated with increased toxicity10 with more marked adverse effects on growth, bone turnover and surrogate biochemical markers of fat mass and insulin sensitivity in children with ALL.6 18 The extent of glucocorticoid effect may be variable, and the concept of “one equipotent dose for glucocorticoid effect” needs to be reconsidered as it may be an end-organ-specific phenomenon. Our observation that ON was almost exclusively associated with the use of Dexamethasone is also notable and may reflect on the aetiology of this condition. Despite relatively minor differences in Prednisolone equivalent doses in the Dexamethasone group versus the Prednisone group (less than 10%), we observed a threefold greater incidence of musculoskeletal morbidity in the Dexamethasone-treated group.
Our observation that ON was more commonly associated with the use of Dexamethasone is also notable and may reflect on the aetiology of this condition but needs to be confirmed in larger studies. The incidence and distribution of symptomatic ON in the current study was similar to that reported in previous studies.7 19 The lack of sexual dimorphism, earlier timing, association with large joints, particularly in the weight bearing appendicular skeleton and almost exclusive association of ON with Dexamethasone emphasises the fact that the aetiology of ON is different to that of fractures. Studies on animals with steroid-induced ON in the femoral head show hypertrophy and hyperplasia of marrow fat cells and lipid deposition in osteocytes.20 In addition, hyperlipidaemia secondary to glucocorticoid administration has also been linked to the occurrence of ON.21
There are other drugs in the chemotherapy protocol that have been reported to adversely affect bone health. Most notably, these include methotrexate (5) but vincristine may indirectly affect bone health through reduced physical activity. L-asparaginase-induced coagulopathy has previously been reported to be associated with ON,22 and in larger cohorts of patients, it would be useful to explore the combined effect of dexamethasone and the more effective forms of asparaginase that have been introduced over the last decade.
There were a number of other important findings in this study that may shed further light on the different aetiology of fractures and ON. ON was more likely to occur in older children and musculoskeletal pain, as the sole finding without any radiological findings of skeletal morbidity, and fractures were more likely to occur in younger children. ON in SAC group was more likely to occur earlier, whereas fractures were more likely to occur at a later stage of treatment. These findings point to a difference in the aetiology of these glucocorticoid-related adverse effects, and they also help in developing a rationale for the timing and nature of bone-protective interventional strategies. According to these findings, therapy duration and onset of puberty might be an influential risk for fractures and ON, respectively. The early onset of ON in girls and late onset in boys in our study may also support the correlations between ON and puberty.
The observation that fractures tend to occur later in maintenance therapy may be explained by the multi-factorial aetiology of low bone mass in these children, the accumulation of the different effects of glucocorticoids and an imbalance between low bone strength and increasing activity. However, the timing was later than that described by others7 8 and may reflect differences in the chemotherapy protocols. The predisposition of the older child to skeletal morbidity is recognised; children may be more sensitive to interference with skeletal development during the peripubertal and adolescent growth phases, when bone mass increases due to a disproportionately greater increase in bone formation than resorption. This process of bone mass accretion is linked to the direct and indirect effects of sex steroids on bone through the growth hormone axis and muscle development. It is, therefore, possible that children are more likely to fracture around the peripubertal period if the normal process of bone acquisition is disrupted. It is also possible that older children are more likely to localise musculoskeletal pain to specific parts of the skeleton.
A sex difference in fracture incidence with a higher incidence in boys has been described before.7 While our study also shows this difference, the results were not statistically significant. Interestingly, a recent study in children with asthma reported that boys receiving oral glucocorticoids were more likely to suffer osteopenia than girls.23
In summary, this report represents the first detailed study of the skeletal morbidity associated with contemporary protocols of chemotherapy for the treatment of childhood ALL in the UK. At least a quarter of children develop confirmed ON or fractures, typically at around the end of the first year and the second year of chemotherapy, respectively. These data may facilitate the institution of appropriately timed regimens that reduce skeletal morbidity.
Acknowledgments
ME is supported by the Gaddafi International Charity and Developmental Foundation of Libya.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.