Article Text

Abstract
After rapid economic growth, more than 90% of the Icelandic banking system collapsed within 2 weeks in October 2008. A severe economic crisis of historic proportion ensued from which Iceland is still recovering. To protect those most vulnerable, governmental response included policy measures aimed to address the needs of children, families, the elderly, those on social benefits and the unemployed. By the maintenance of free universal healthcare for pregnant women and children, child health has been preserved. Six years later, there is little notable impact of the crisis on key child health indicators. Yet, the proportion of children born small-for-gestational age increased from 2.0% to 3.4%. One important pillar for the outcome is the good coverage and easy access to universal healthcare, educational and social services with highly qualified professionals. Iceland has shown that, by protecting the most vulnerable and maintaining universal access to healthcare, children's health and well-being can be maintained during an economic crisis.
- Public Health
- Delivery of Health Care; Integrated
- Health Policy
- Economic Recession
- Child Welfare
Statistics from Altmetric.com
Since October 2008, Iceland has experienced a deep recession. The task facing the state, its institutions and the population at large has been huge and daunting. One was to protect social, educational and healthcare services that in recent years have been ranked as one of the best in the world.1 Several studies have analysed the impact of the crisis on the health and behaviour of Icelandic adults.2–7 Yet, in economically difficult times, children and families usually experience the most difficulties.8–12
Child health and economic hardship
Socioeconomic inequalities in health are found in all societies, including welfare states like Iceland.13 Inequalities may affect children from their intrauterine development and throughout their life-course, and are socially determined.14 These may aggravate in times of economic crisis, in particular in countries with weak mechanisms for social protection.15 In a recession, vulnerable families may suddenly find themselves caught in poverty trap, for example, by unemployment and high family debts. This may have negative consequences on the health of pregnant women and young children,16 and later adult health.17 Policy measures have the potential to mitigate the negative impact economic crisis may have on families and the population at large, and include for example, fiscal stimulus, social protection and policies that address the labour market, and provide additional support to families.9 ,18 A recent systematic review10 has highlighted the adverse effect of the economic crisis on child health since 2008. The impact is varied between countries on most of the studied health outcomes, with the exception of negative impact on food consumption and nutrition of children.
The aim of this review is to address the impact of the economic crisis in Iceland on the health and well-being of children and families. The economic aftermath of the bank collapse and policy responses were studied, with particular attention given to those that might impinge on children and families. Data were retrieved from several national databases that monitor healthcare delivery and outcome, and nationwide survey data on child and adolescent health and well-being were analysed, based on commonly defined child health indicators.19–21
The socioeconomic setting
From boom to doom
The rapid rise of the Icelandic banks in 2002–2007, following their privatisation, is unprecedented in the recent history of banking.22 The total assets of the banking system went from 174% of the gross domestic product (GDP) at the end of 2003 to about 1000% at the time of the collapse in October 2008. GDP rose by approximately 5.5% each year over the period. Real estate prices increased sharply, while stock prices of Icelandic firms increased by a factor of 7, one of the most rapid increases ever in any country.23
Despite warning signs that an economic bubble based on credit boom was bound to burst,24 the financial market, commerce, economists, politicians and, not the least, the Icelandic population (about 320 000) were astounded when all three major Icelandic banks collapsed over a period of 2 weeks in October 2008. This brought down more than nine-tenths of the banking system,25 and as one entity the failed banks rank third in the US history of bankruptcies.22
Socioeconomic indicators
The steep economic downturn resulted in a fall of the GDP by more than 10% from its peak in 2008, (figure 1A).26 Unemployment rate increased (figure 1B)26 with peaks of 12%–14% in some areas, and alleviated somewhat by emigration of skilled workers, in particular to Norway.

Development of gross domestic product (GDP) and unemployment following the economic collapse. (A) GDP for the period 2007–2014. (B) Unemployment rates, corrected for season, for the period 2008–2014. Data Source: Central Bank of Iceland.26 OECD, Organisation for Economic Co-operation and Development.
The proportion of children living in homes at risk of poverty (<60% of the median income), and who experienced material deprivation was similar in the periods 2004–2007 and 2010–2013, but the levels are age-dependent (figure 2).27 Yet, the impact was disproportionate, with single parent households, young parents and those who rent their homes the worst affected. Despite the crisis, in 2012, Iceland had the second lowest proportion of children at risk of poverty, and seventh lowest experiencing material deprivation, compared with other European countries.27

The proportion of children aged 0–5 years and 12–17 years in Iceland at risk of poverty and material deprivation, during the period between 2004 and 2014. Data Source: Statistics Iceland.27
Governmental response
The overall aim of the governmental response to the economic collapse was to protect the fundamental and comprehensive structure of the welfare and social security system already in place.15 ,28 ,29 Yet, faced with unavoidable cost reductions, including welfare costs, governmental responses gave prominence to redistribution, through taxes and the social protection system and labour market and debt relief measures aimed at middle-income and low-income groups.29
For healthcare, government cuts in spending in relation to GDP were deep, down from an average of 9.2% in 2000–2008 to 8.8% in 2009–2013, compounded by a decreased GDP and depreciation of the local currency. For the same two periods, out-of-pocket payment of total healthcare costs was on average 18.3% and 19.2%, respectively. To monitor the potential impact of the economic collapse on the health and well-being of the population, the government set up, in February 2009, a large independent advisory body (Velferðarvaktin (Welfare Watch)) including representatives from non-governmental organisations, labour market, municipalities, institutions and government ministries.30
Box 1 summarises some selected policy measures in response to the crises with relevance to the health services for children.
Selected policy measures with implications for healthcare services for children and their families following the economic collapse
Cuts in healthcare costs
▸ Human resources
Cuts in number of staff
No recruitment in case of vacancy because of disease or leave
Less continuous professional education
Fewer posts for training of students
▸ Salaries
Full-time staff to part-time, or cuts in salaries
Fringe benefits of health workers cut, for example, extra hours, travel allowance and other subsidies
▸ Organisational changes
Reorganisation that included mergers of healthcare organisations or departments
▸ Healthcare insurance
Private specialists increased user-charges following no agreement with the Icelandic Health Insurance on remuneration (agreement in place since 1 January 2014)
▸ Drugs
Emphasis on rational drug prescribing and lower procurement costs
▸ Logistics
Maintenance postponed and purchase of new equipment delayed, if possible
▸ Physical structures
No new constructions and maintenance delayed
Plans for a renovated and expanded University Hospital have been delayed
▸ Maternity/paternity leave
Compensation cut to about 42% compared with the level before the collapse
Time frame for its use increased from 18 to 36 months after birth.
Protected and improved healthcare services
▸ Preventive and curative services
Continued policy of free maternity care, and preventive and curative healthcare services for children (<18 years of age) in state-funded health institutions
Policy of free dental services, introduced in 2013, for children aged 3 years, and since January 2015 also for those children aged 8–17 years who have signed up with a family dentist
Continued policy to earmark funds for public health activities, that is, 1% of alcohol tax and 0.9% of the tobacco tax.
▸ Expanded and improved national guidelines and tools
Maternity care, revised national guidelines launched in April 2008
Preventive healthcare services for children <6 years of age, launched in September 2009, with later improvements
Electronic Health Records for preventive healthcare services for children aged <6 years, and school health services for children aged 6–15 years, revised and improved in 2009/2010, and onwards
▸ Immunisation
Human papillomavirus vaccination introduced in 2011 for girls aged 12 years
▸ Mental health and well-being
Mental health services for children within primary healthcare and hospital services expanded and improved
Parental training programmes expanded
Multisystemic therapy for children and adolescents with mental, behaviour and drug abuse problems introduced in 2008, and later strengthened and improved.
Maternal and child healthcare services
Organisation
Healthcare services in Iceland are comprehensive, state-centralised, with universal access, regardless of social status, financial ability to pay or geographical location.31 State-funded primary healthcare (PHC) centres are found all around the country and offer high-quality services provided by general practitioners (GP), nurses and midwifes, and in some instances other health professionals. Maternity care and birth, and preventive and curative services for children <18 years in state-funded health institutions are free of charge, including hospital services. This national network of services is linked together with Electronic Health Records (EHRs) that include records designed for preventive child health promotional activities.32 Private medical specialists complement the state-run services, mostly in the Reykjavik Capital Region, and apply user charges on top of contractual remuneration by the state. In a recent comparison of health policy performance in 43 European countries based on available data closest to the year 2008, that is, before the economic collapse, the Icelandic healthcare system ranked third, after Sweden and Norway.33
Maternity care
Pregnant women in Iceland are offered free maternity and delivery services in line with national guidelines, thoroughly revised in 2008 prior to the collapse (box 1). These recommend 10 visits for primipara and 7 visits for multipara. In the period 2003–2008, primipara attended the services on average 11.8 times per pregnancy compared with 10.8 times for multipara; in the period 2009–2014, with the figures being 9.9 and 9.2, respectively.
Maternal and infant health
There was no change in the average fertility rate of 2.1 children born to women of fertile age in two 5 year periods, before and after the collapse; it peaked with 2.22 in 2009 but was down to 1.93 in 2014. The economic crisis has had no discernible impact on maternal, perinatal, neonatal, infant or child mortality rates.19 ,34 ,35 To evaluate the impact of the economic collapse on birth outcome, all singleton births of Icelandic women in the period 2008–2009 were analysed in quartiles for that period.36 The incidence of low-birth weight increased significantly only for women giving birth in the period between April and June 2009, that is, about 6–9 months after the bank collapse. Yet, the average proportion of children with an International Classification of Diseases (ICD)-10 diagnosis of small-for-gestational age (SGA) increased from 2.0% in the period 2003–2008 to 3.4% in 2009–2014.
Health promotional child health services
The health promotional services for children are comprehensive and build on national guidelines. These include a variety of free services in the home and in healthcare centres to families and children 0–5 years of age and in compulsory schools for children aged 6–15 years. After the economic collapse, the fundamental structure of service delivery has mostly been protected, and in some aspects the service provision has even been improved (box 1). For example, revised EHRs include new modules for growth monitoring, developmental surveillance and health promotional interviews of school health nurses with children at 6, 9, 12 and 14 years of age.32
There was no notable impact of the crisis on breastfeeding rates; at 6 months of age about three-fourth of the mothers are breastfeeding. Yet, the annual average number of home visits per newborn child (<9 weeks) has diminished from about 2.5 up to the year 2009 to 1.8 since 2010. Immunisation rates remained high, for example, measles at 4 years, on average 91% (89–93) for children born in the period 2005–2011.
Curative services for children
After the collapse, curative services in state-funded health institutions for children <18 years of age continued to be free of charge (box 1). Number of visits to GPs in PHC increased from 1.46 visits per child to 1.60 (9%) in the period 2005–2013. In the same period, consultations of private paediatricians who apply user-charges increased from 0.54 to 0.66 (21%) per child.
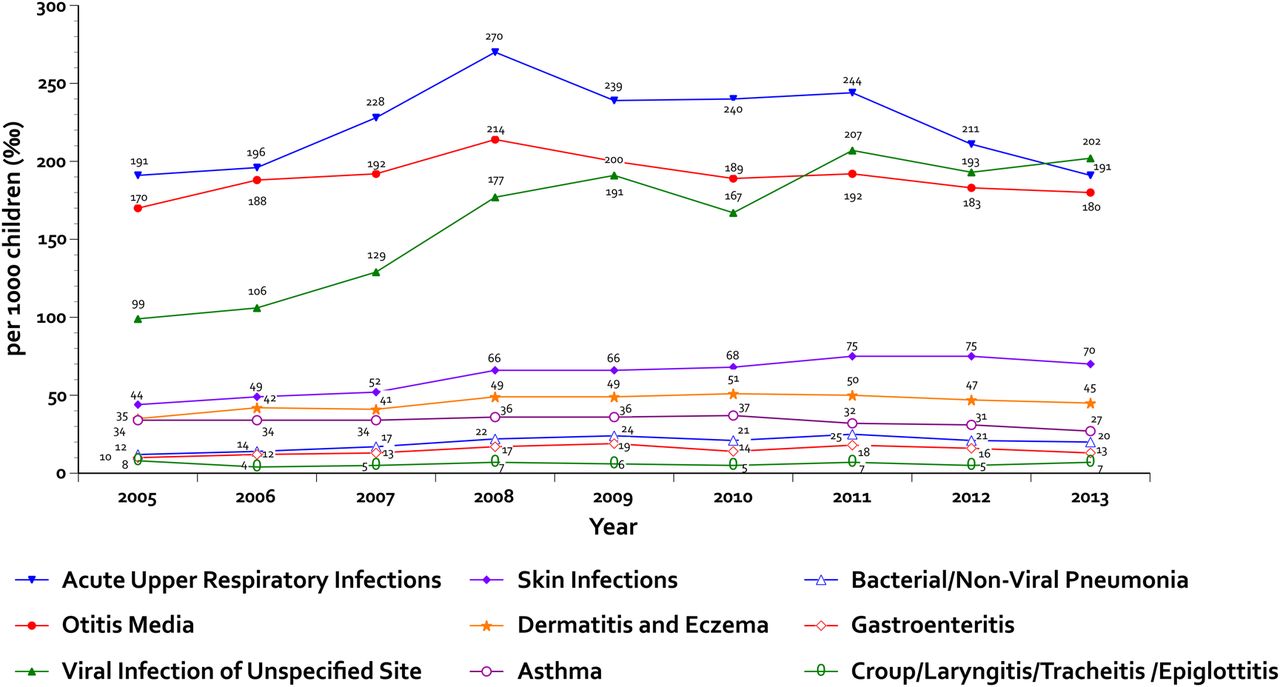
Nine diseases associated with child poverty21 were analysed within the context of PHC and hospital admissions for children aged 0–17 years. There is no evidence of any significant change in incidence for the most common ICD-diagnosis given by GPs or paediatricians, neither within PHC (figure 3) nor hospitals. Further, separate age-standardised analysis for the age groups of <1, 1–4, 5–9 and 10–17 years gives the same result.
{kind=link}
{kind=link}
{kind=link}
Incidence per 1000 child population of nine most common clinical ICD-10 diagnosis, associated with child poverty, given by general practitioners (GPs) for children <18 years seeking care in healthcare centres during the period between 2005 and 2013. Data Source: Directorate of Health.
Despite the crisis, children suspected to have developmental, behavioural and/or mental health problems have gradually had improved access to appropriate services (box 1). These include interdisciplinary evaluation, more parental training programmes and annual increase in number of children on attention deficit hyperactivity disorder treatment with methylphenidate. Further, services for children with the most severe disabilities have continued with little notable impact of the economic collapse.
The 5 years survival rate after the diagnosis of acute lymphatic leukaemia has been suggested as a context neutral measure of the quality of clinical treatment for children.20 Despite low numbers and wide CIs, there are no indications of worse outcome in the period after the crisis; on the contrary, 5 years survival rates show continuous gradual improvement since 1989 (table 1).
Relative survival rate (%) of children aged 0–19 years diagnosed with acute lymphatic leukaemia for the period from 1989 to 2013*
Social and welfare services
Maternity/paternity leave
With each singleton birth, mothers and fathers are entitled to 3 months each of maternity/paternity leave, in addition to 3 months at their own disposal. Following the crisis, the benefit levels were reduced (box 1) and an increasing number of fathers did not take their legal share of the paternity leave. For the 2007 birth cohort, about 84% of them used at least 3 months compared with about 60% of the 2011 cohort, the last year with complete data.
Preschool attendance
After maternity/paternity leave, 85%–90% of children <6 years attend preschool. In an attempt to curtail costs, the largest municipality Reykjavik for example raised the price for the ‘9th hour’ as many parents did not make use of it despite being eligible to do so for a low fee. In response, about a quarter of parents decided to continue to pay the extra hour compared with about one-third before the collapse.
Child protection
In the period from 2003 to 2013, the number of children notified to the Child Protection Units gradually increased per year from 3.558 to 4.880, with peak in the year 2009 with 5.322 notifications. There are no indications that the economic collapse markedly changed the character of the services; rather increased attention to children and families may have increased awareness and sensitivity to their needs.37
Health and well-being of children and adolescents
In February 2009, a few months after the collapse, about 90% of school children aged 10–12 years reported that they felt rather well or very well during lessons, girls more so than boys.38 Despite some gender differences, in an analysis for the period 2000–2014,39 adolescents aged 14–15 years reported generally improved health and well-being after the crisis or no change (table 2).40 ,41 In 2010, children aged 11–15 years reported either improved satisfaction with their life situation or no change compared with 2006.42
Selected variables from the national survey Young People in Compulsory Schools for the period 2000–2014*
Discussion
The collapse of all three major banks in Iceland in a 2 week period in October 2008 is extraordinary, in a global as well as national context. An economic downturn of this scale can have negative implications for child health,8–12 ,16 and long-term consequences for later adult health.17 In this study on child health in Iceland before and after the economic collapse, governmental policy measures with focus on vulnerable groups,28–30 including children and families (box 1), may have alleviated some of the worst health effects of the crisis. The data presented indicate that the government and the society at large have been successful in this respect.
In Iceland, irrespective of socioeconomic status, all have easy access to healthcare services. Despite the crisis, a policy of free services was maintained in state-funded healthcare institutions for pregnant women and delivery, and for curative services and health promotional activities for children <18 years.31 In contrast to Greece,18 ,43 access to healthcare in Iceland is not linked to the employment status of parents, and there is little evidence of negative impact on commonly used child health indicators19–21 following the crises. One lesson to draw is the key role of well-organised welfare services in times of economic turmoil, and application of policies that aim to protect the overall health of the population, and in particular the needs of disadvantaged groups. Another lesson is the importance of universal access to high-quality health and educational services for all, irrespective of socioeconomic status. Despite Iceland's geographical location and small population, these are lessons of relevance for other countries as well.
At the end of 2010, one in five parents in Iceland were in financial distress, many because of imprudent lending of housing and motor vehicles before the collapse.44 Yet, the percentage of children living in poverty (<60% of median income) changed only modestly following the collapse.27 Yet, the impact is disproportionate, depending on age (figure 2) and type of household. This bears witness to partially successful policies to protect those most in need despite an economic downturn (box 1).28 ,29 This outcome has for example been facilitated by the work of the Welfare Watch, established in February 2009, and supported by several task forces on key themes of concern.45 Particular attention was given to the needs of those most vulnerable, for example, children and families, young people, unemployed, on social security and the elderly. The Welfare Watch informed the government continuously on its work and advised the parliament on appropriate actions to take.30
One example of misguided policy measure is the decreased benefit level for maternity/paternity leave (box 1), with the result that fathers have in increasing numbers not taken their legal share of the leave. Further, the number of home visitations to families of newborns has diminished after the crisis. A lesson learnt is that policy measures have to take the whole socioeconomic context of children and families into consideration. The early years of children need to be protected for later health and well-being, and productive life.46 ,47 In this context, the increased proportion of children with diagnosis of SGA needs further analysis, a work that is underway.
The incidence (‰) of the nine most common ICD-10 diagnosis with known socioeconomic gradient21 was analysed for children aged 0–17 years seeking care from their GPs in the period 2005–2013 (figure 3), and in hospitals. No discernible change in diagnostic profiles is seen during this period, indicating that the economic collapse has not severely impacted on morbidity, care-seeking behaviour or access to services for this age group. Further, relative survival rates for children diagnosed with acute lymphatic leukaemia are still improving (table 1), a sign of continued high-quality clinical services. Interestingly, there are examples of expanded services to children and families despite the collapse (box 1), for example, for children with behavioural and mental health problems.
Despite economic downturn and times of insecurity, many indicators of health and well-being of Icelandic adolescents show either no change or improvement after the economic collapse compared with the period before it (table 2). Improvement is seen in parental support and relates positively with adolescents’ happiness,40 health behaviour and participation in sports. This is in contrast to results for their peers in some European countries experiencing economic difficulties.48 It is possible that parental stress and workload during the ‘boom years’ may have negatively impacted on attention given to their children. With less economic activity, parents seem to spend more time with their children. A lesson learnt is that despite economic downturn, and times of insecurity, many indicators of health and well-being of children and adolescents need not suffer if due consideration is given to families and their needs.
It has not been possible to analyse socioeconomic data and relate those to the outcome on health and well-being of young children and adolescents. Regular linkage of such data to information in other databases, including EHR,32 should be developed with a keen eye on inequality. Regular compilation of social indicators, initiated by the Welfare Watch in 2012,49 is a positive step in that direction. Continued national, annual surveys on the health and well-being of children and adolescents in compulsory39 and upper secondary schools are also necessary to monitor the medium and long-term impact of the economic collapse and to contribute to well-directed preventive actions.
The future
In the aftermath of the economic collapse in Iceland, many initiatives and policy measures were taken with the aim of protecting the health and well-being of children and their families.28–30 Yet, there are signs that give reasons for concern. Cuts in costs within the healthcare sector have been substantial and may threaten its future quality. Increased workload of staff, stressful working environment, low salaries, worn-down physical structures, inadequate equipment and emigration of skilled health workers, coupled with less than optimal recruitment of young health professionals, have impacted negatively on staff.50 This is exemplified by strikes by doctors from October 2014 to January 2015, the first of its kind, and other health professionals have followed suit. In the light of well-known negative consequences of privatised healthcare services,51 ,52 calls now for still greater involvement of private enterprise in the services are of concern. Thus, the Icelandic healthcare system is standing at a crossroads. The universal and high-quality services for all may not be guaranteed if actions are not taken to secure its future.
Acknowledgments
The compilation of data presented would not have been possible without the help of many people. The following persons are gratefully acknowledged for their contribution: Cancer Registry (Laufey Tryggvadóttir, Elinborg Olafsdottir); Central Bank of Iceland (Stefán Jóhann Stefánsson); Child Protection Services (Bragi Guðbrandsson); City of Reykjavik (Hildur Björk Svavarsdóttir); Directorate of Health (Anna Björg Aradóttir, Dóra Guðrún Guðmundsdóttir, Hildur Björk Sigbjörnsdóttir, Lilja Bjarklind Kjartansdóttir, Ólafur Einarsson, Ragnhildur Erla Bjarnadóttir, Sigríður Haraldsdóttir, Svanhildur Þorsteinsdóttir, Þórólfur Guðnason); Icelandic Centre for Social Research and Analysis—ICSRA (Hrefna Pálsdóttir, Jón Sigfússon); Maternity/Paternity Fund (Leó Örn Þorleifsson); Ministry of Welfare (Anna Sigrún Baldursdóttir, Lára Björnsdóttir (former employees)); Primary Healthcare Organisation of Greater Reykjavik Area (Gyða Haraldsdóttir, Lilja Bjarklind Kristinsdóttir, Ragnheiður I. Bjarnadóttir, Ragnheiður Ósk Erlendsdóttir, Sesselja Guðmundsdóttir); Statistics Iceland (Kolbeinn Stefánsson); State Diagnostic and Counselling Centre (Stefán J. Hreiðarsson); University of Akureyri (Ársæll Arnarson) and University of Iceland (Arna Hauksdóttir, Guðný Eydal, Gylfi Zoëga, Jónína Einarsdóttir, Stefán Ólafsson, Tinna Laufey Ásgeirsdóttir, Unnur Anna Valdimarsdóttir). All interpretations and opinions expressed are the sole responsibility of the author.
References
Footnotes
Competing interests The author was Chief Medical Officer for Iceland from 2010 to 2014.
Provenance and peer review Commissioned; externally peer reviewed.