Article Text

Abstract
Aim This longitudinal study investigated protective factors for social-emotional well-being in refugee children in Australia.
Methods Newly arrived refugee children aged 4–15 years were recruited between 2009 and 2013 and assessments were conducted at two points, at years 2 and 3 postarrival. Social-emotional well-being was assessed using the Strengths and Difficulties Questionnaire (SDQ). Protective factors were assessed by structured interview and the Social Readjustment Rating Scale (SRRS); scores <150 reflect fewer stressful life events in the previous year.
Results Forty-three eligible refugee children were recruited. The SDQ was completed by parents in 90% and protective factor data in 80% at years 2 and 3 of follow-up. Protective factors for normal SDQ scores were: originating from Africa (p=0.01), father present on arrival (p=0.019) and family SRRS scores <150 at year 2 (p=0.045). The median number of protective factors was 4 (range 1–8). Better SDQ scores were associated with ≥4 protective factors (p<0.006). Furthermore, more protective factors increased the child’s likelihood of a stable or improved SDQ score over time (p<0.04). Modifiable protective factors likely to promote social-emotional well-being include stability in the child’s school and residence, parental employment, financial and marital stability, proximity to one’s own ethnic community and external community support.
Conclusions Cumulative protective factors, some of which are potentially modifiable, can predict social-emotional well-being in newly arrived refugee children. Children with four or more protective factors are at low risk of poor social-emotional well-being.
- refugee child
- risk factors
- protective factors
- social-emotional wellbeing
- strengths and difficulties questionnaire (SDQ)
- longitudinal cohort
Statistics from Altmetric.com
- refugee child
- risk factors
- protective factors
- social-emotional wellbeing
- strengths and difficulties questionnaire (SDQ)
- longitudinal cohort
What is already known on this topic?
Refugee children are known to be highly resilient.
Refugee children have multiple risk and protective factors for social-emotional well-being.
Social-emotional well-being over time and protective factors that predict it are seldom studied.
What this study adds?
Social-emotional well-being can be measured over time in refugee children and mostly improve over time.
Cumulative protective factors can predict social-emotional well-being in refugee children and some are modifiable.
Refugee children with fewer than four protective factors may benefit from proactive follow-up.
Introduction
The global refugee crisis requires that researchers, policymakers and clinicians comprehend the impact of forced displacement on health and well-being and the factors that moderate them.1 Most extensively studied to date are the associations between adverse exposures and abnormal mental health in clinical populations.1 2 These studies, including meta-analyses and systematic reviews, highlight remarkably similar risk factors for poor health and well-being outcomes, including female gender, unaccompanied child status, time in immigration detention, premigration and/or postmigration violence exposure, family separation, psychological morbidity of carers, negative school and peer experiences, perceived discrimination, parental unemployment, fall in socioeconomic status and financial stress.1–9
However, to explore protective factors associated with well-being, a population-based approach with longitudinal study design and prospective measurement is needed.1 2 10 The few published prospective longitudinal studies of refugee children and/or youth are from the USA, Denmark, Sweden and Australia, with follow-up periods of 6–12 years. Sample sizes range from 27 to 131 subjects, with limited examination of possible protective factors.7 8 11 12 Findings include that subjects were highly resilient, mental health outcomes improved over time and postmigration stressors were more predictive of psychological problems than adverse experiences before arrival, suggesting there is opportunity for intervention by resettlement countries to improve long-term outcomes.1 2 12
Resilience is an individual’s capacity to thrive, mature and develop competence despite adverse circumstances, and the ability to adapt under conditions of severe hardship and prolonged adversity.13 Resilience and protective factors can be conceptualised as the antithesis to vulnerability and risk. This study focuses on protective and modifiable factors that may be useful to clinicians and policymakers.
We conducted the first population-based, longitudinal study of newly arrived refugee children in an Australian setting, using a standardised outcome measure (Strengths and Difficulties Questionnaire, SDQ) of social-emotional well-being and measured prospectively the factors likely to impact on well-being over the first 2–3 years of settlement.14 15 We aimed to investigate potentially modifiable protective factors for social-emotional well-being in newly arrived refugee children. The hypothesis was that 70% of children would improve in social-emotional well-being over time, and the remaining 30% would have ongoing social-emotional difficulties associated with the absence of identifiable protective factors.1 2 14
Methods
A population cohort of all newly arrived refugee children in a regional health district was visited at home by refugee nurses and invited to participate in this study between 2009 and 2013. Parents of recruited children aged 4–17 years completed the parent-report version of the SDQ at year 2 (average 11 months; range 5–24 months) and year 3 (average 31 months; range 21–40 months) postarrival. Face-to-face interpreters were used for all assessments; translated SDQs were used for literate Arabic and Farsi-speaking participants.
Ethics approval
The study received ethics approval from the Human Research Ethics Committee Northern Hospitals Network, South Eastern Sydney Illawarra Area Health Service (HREC Ref No 09/163).
Protective factors
Using an adapted ecological risk model,16 17 protective factors were explored by parent completion of a structured questionnaire (online supplementary appendix 1) and the Social Readjustment Rating Scale (SRRS) (online supplementary appendix 2), which measures stressful life events in the last year. Scores <150 have a low risk of stress-related illness.18 19 Protective factors were classified into child, family and settlement factors (table 1).14 15
Supplementary file 1
Supplementary file 2
Potentially protective factors for SDQ scores, prevalence over time and univariate analysis of protective factors
Outcome measure
The SDQ was selected as a tool with high sensitivity and specificity and validated for assessing social-emotional well-being across cultures.15 It includes 25 items with five symptom scales and a total difficulties score, each with means and SD for the Australian population.20 High SDQ scores indicate increased risk of social-emotional problems.21 22 Since both protective factors and outcomes were measured at both year 2 and year 3, protective factors measured at year 2 were considered potentially predictive of outcomes at year 3.
Data analysis
Data were analysed using SPSS V.22.0 (IBM). For all analyses, p values were considered statistically significant if <0.05. The SDQ total difficulties score was treated as either a continuous variable, or categorised into: (1) normal and (2) borderline and abnormal. Paired tests were used to examine changes in SDQ score over time. Using the SDQ as a continuous variable, children with an increased score by 6–14 points on the SDQ between years 2 and 3 were regarded as ‘worse’; the rest were ‘stable’ or ‘improved.’14 15 Associations between the SDQ score and categorical variables were investigated using non-parametric tests (Mann-Whitney U tests and Kruskal-Wallis tests). Cross-tabulations (exact Χ2 values) were used to assess univariate associations between categorical variables. Χ2 trend tests (linear by linear association) were used to assess linear trends for SDQ with increasing exposure to protective factors.
Protective factors with the highest p values on univariate analysis were selected for inclusion in computing protective factor scores for normal SDQ at year 3. Protective factors were serially added to a cumulative protective factor score in order of increasing p value from the univariate analysis and the score tested at each addition against whether children had a normal or abnormal SDQ at year 3. The process was halted with eight protective factors included in the score, after which no further prediction value for abnormal SDQ was found.
Due to small numbers of children with abnormal/borderline SDQ it was not possible to create a multivariate score with factors weighted on importance. For postarrival factors, children required all three variables for a score to be calculated.
Power calculation
With power set at 0.8, significance at 0.05 and with the prevalence of risk factors of interest ranging from 11% to 97%, we required a sample size of 43 children to demonstrate significant associations with change in SDQ given a 30% difference in outcome between exposure groups.
Results
Between May 2009 and April 2013, a total of 228 refugee children aged <15 years arrived in the study region, 158 met the overall eligibility criteria and 61 (39%) aged 6 months to 15 years were recruited to the study. Of these 43 were eligible for the SDQ (ages 4–17 years) and form the basis of this analysis. Children retained in the study over 2–3 years were similar to those not recruited and lost to follow-up in terms of gender, WHO region of origin and language spoken at home.15 Fewer children were initially recruited than anticipated due to shortage of appropriate language interpreters available to conduct the extensive research regimen (n=52, 33%), families/children declining to participate (n=24, 15%), relocation out of the area (n=13, 8%) or not contactable (n=8, 5%). Sample characteristics, physical and developmental health are described elsewhere.14 15
The SDQ was completed in 39 of 43 (91%) and 38 of 42 (90%) eligible children at years 2 and 3, respectively. Protective factor data were completed in 31 (80%) and 33 (79%) children at years 2 and 3. At year 2, five (13%) children were in the abnormal range for total difficulties SDQ scores (mean 8.5; SD 6.7), and over 20% of children were experiencing emotional symptoms and/or peer problems. By year 3, problems had decreased to below 10% (mean 7.4; SD 6.2), below the rate expected for the general Australian population for total difficulties (mean 8.2; SD 6.1) and across all subscales. Mean SDQ total difficulties scores did not differ from those in the general Australian population at both years (p=0.75; p=0.47). For children with SDQ scores at both years, 18 (67%) remained normal, 6 (22%) improved over time, 2 (7%) remained abnormal and only 1 child worsened.14 SDQ total difficulties score at year 2 predicted SDQ score at year 3 (p=0.013). Of children who were normal at year 2, 95% were normal at year 3. Children who scored in the abnormal or borderline ranges were referred to their general practitioner; none had specific interventions.
Protective factors associated with normal SDQ
Associations between SDQ scores and child, family and settlement factors
Table 1 shows both changes over time as well as comparison with and without protective factors. The proportion of normal SDQ scores increased over time, whether or not protective factors were present. For example, 92% of children with fewer stressful life events in the previous year (SRRS >150) had normal SDQ at year 2, improving to 100% normal at year 3. Only 56% of children with stressful life events in the previous year were normal, improving to 82%. This shows a 26% difference in those with and without the protective factor at year 2 as well as improvement over time for both groups.
Child factors
SDQ score was not associated with gender, body mass index or the presence of chronic disease on arrival (p>0.05). All the children under 6 years on arrival had normal SDQ scores at year 3.
Family factors
Children from the Africa region had SDQ scores 6.6 points lower than those from the Eastern Mediterranean region (p=0.01; 95% CI 1.5 to 11.7); all 12 children from Africa had normal scores by year 3. In children from South East Asia (predominantly Burma), difficulties were also largely resolved by year 3. SDQ scores were more likely to be abnormal at year 3 and to deteriorate over time in children from the Eastern Mediterranean region (predominantly Iran and Iraq) (p=0.01) (figure 1), with increased emotional symptoms (p=0.02) and peer problems (p=0.01). The few children who were deteriorated over time appeared more likely to have experienced significant prearrival trauma, had no siblings and parents with great difficulty with English.

Changes in SDQ scores over time by WHO region. SDQ, Strengths and Difficulties Questionnaire.
Presence of the child’s father on arrival was associated with lower SDQ scores at year 2 (0.02) but not at year 3 (p=0.07). SDQ subscales showed hyperactivity inattention, emotional symptoms and peer problems at year 2 (p<0.05) (table 2). Hyperactivity inattention and emotional symptoms persisted at year 3 in those with absent fathers (p=0.04). SDQ was not associated with the child’s birth in a refugee camp or parental self-disclosure of trauma prior to arrival (p=0.37; p=0.38).
Father’s presence/absence on arrival and mean SDQ scores at year 2 and year 3 (with 95% CIs)
Settlement factors
At year 2 children with family SRRS scores <150 were more likely to have normal SDQ scores (p=0.045; OR=9.6 (95% CI 1.02 to 90.34)); 92% had normal SDQ scores as compared with only 56% of children with SRRS scores >150 (figure 2). Children with family SRRS scores >150 were more likely to have conduct problems at both year 2 (p=0.007) and year 3 (p=0.04). The most common stressful life events mentioned were changes in the child’s school and residence, death of a close relative or spouse, parental unemployment, marital separation and financial stress. SDQ scores were not associated with the perception of Australia as tolerant towards people of other religions, cultures and nationalities, parental education, study status, English language proficiency or access to healthcare on univariate analysis (p>0.05).

Stressful life events in the previous 12 months (SRRS) and SDQ scores at year 2 and year 3. SDQ, Strengths and Difficulties Questionnaire; SRRS, Social Readjustment Rating Scale.
Cumulative protective factors
Protective factors with the highest p values on univariate analysis were selected for inclusion in computing cumulative protective factors for normal SDQ at year 3 (table 3).
Protective factors for normal SDQ at year 3; those included in protective factor analysis in bold
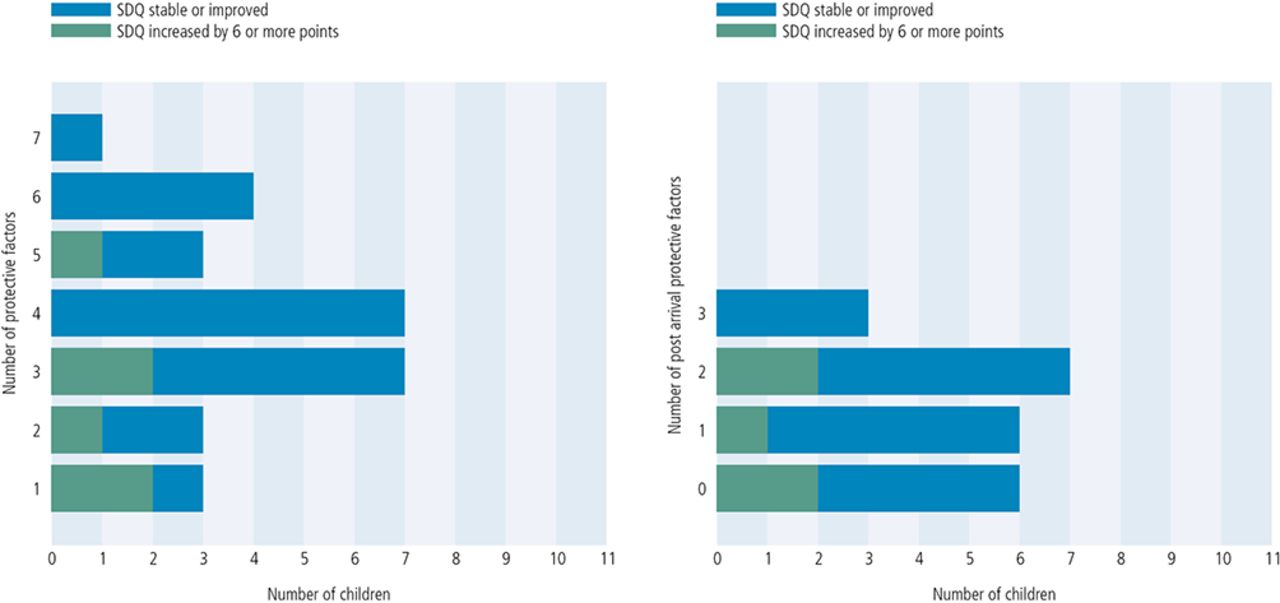
The median number of protective factors was 4 (range 1–8); 63% of children had ≥4 protective factors, all of whom had normal SDQ scores (figure 3). Increased protective factors were associated with lower mean SDQ score (figure 4) (p<0.006), and increased likelihood of a stable or improved SDQ score over time (p<0.04) (figure 5). For example, 100% of children with six or seven protective factors were stable or improved as compared with 33% with one.

Frequency of protective factors per child. SDQ, Strengths and Difficulties Questionnaire.

SDQ scores and protective factors. SDQ, Strengths and Difficulties Questionnaire.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in SDQ score between year 2 and year 3 and protective factors. SDQ, Strengths and Difficulties Questionnaire.
The most frequent protective factors included father present on arrival, Africa as the region of origin, having relatives in Australia prior to arrival, proximity to one’s own ethnic community, support from the general community and SRRS <150.
Postarrival protective factors
More protective factors postarrival were associated with lower mean SDQ score (p<0.001); 85% of children had one or more postarrival protective factors. Potentially modifiable postarrival protective factors included fewer stressful life events in the last year, proximity to one’s own ethnic community and support from the general community.
Discussion
This longitudinal study explores a wide range of protective factors associated with social-emotional well-being in refugee children 2–3 years after settlement in an Australian context. The most striking finding was that cumulative protective factors can predict social-emotional well-being at 2–3 years postsettlement and that some of these may be modifiable. More protective factors also increased the child’s likelihood of a stable or improved SDQ score over time. Furthermore, this study identifies children with fewer than four protective factors as at risk of poor social-emotional well-being, which is useful clinically to identify those children requiring additional follow-up. This is consistent with the evidence that social-emotional well-being can be modified by reducing cumulative risk in childhood, but suggests reframing to ‘protection’ may be beneficial in this context.23–25
Significant findings were that the Africa region of origin and presence of the child’s father on arrival predicted better social-emotional well-being. The father’s absence resonates with other studies as a risk factor for adverse developmental outcomes but associations between region of origin and well-being have been inconsistent.1 2 7 26 In contrast to the literature, male gender, prior parental education and English proficiency were not protective factors in our study, most likely due to insufficient power and limited variation in our population.
Our study reinforces that multiple contextual factors seem to act as moderators of social-emotional well-being, including economic and social conditions from which people are displaced, as well as into which resettled, and that child, family and settlement factors play a role.1 10 12 Predictive factors identified in other studies, such as premigration violence, may identify families in need of additional support, but these cannot be modified once refugee children have arrived in their settlement countries.1 Of most interest to clinicians and policymakers are modifiable postarrival factors associated with well-being, and our study identified stability in the child’s school and residence, parental employment, financial and marital stability, proximity to one’s own ethnic community and external support from the general community as potentially modifiable risk factors. Family cohesion, limited postmigration relocations and social inclusion are protective factors supported by the literature.1 2 10 12
Based on the findings of this and other studies, recommendations that are likely to optimise outcomes in accompanied refugee children settling in high-income settings include: (1) at the child and family level: integration of children and families into host communities; support for families to remain intact; and (2) at the community and societal level: stable settlement in the host country with minimal relocations; supported educational placements and employment; access to health, social and economic resources. Existing knowledge from other studies would add the prioritisation of reunion of children with families and reduction of postmigration exposure to violence and threat, including detention, racism and bullying.1 2 12
Strengths and limitations
Refugee child populations are inaccessible to researchers for many reasons, including prioritising other aspects of settlement above research participation.1 15 This study’s strength was in unbiased recruitment of a population-based cohort broadly representative of refugee children arriving in the region,15 successful retention of the sample over 2–3 years and measuring protective factors prospectively using standardised tools.
Unfortunately, this study had limitations that a larger cohort and resources to track and follow-up respondents for longer could address. That 20%–30% differences in social-emotional well-being between those with and without some protective factors were not statistically significant suggests the study was underpowered. Furthermore, children exhibited greater recovery to normal social-emotional well-being than expected (<10% had ongoing social-emotional difficulties compared with the 30% predicted), further reducing the power of the study to identify significant individual predictors. Failure to secure ongoing funding meant further recruitment or follow-up became prohibitive. Nonetheless, even this small sample demonstrated some important and clinically useful findings which add to the limited evidence base.
Psychological well-being of carers, violence exposure and intrafamilial conflict are risk factors for child well-being in many studies but were not measured in our study due to the presence of children in the family home during assessments.1 2 There was insufficient variation in the data to undertake meaningful analysis of associations between well-being and socioeconomic resources or access to healthcare across subjects as all families received similar government-funded entitlements. Furthermore, the refugee children enrolled in this study had universal access to primary healthcare, which may not be generalisable outside the Australian context.15 27
Other challenges with generalisability are that successive waves of refugees may differ significantly in terms of the nature and duration of war, violence and displacement which they have experienced, and its impact on their health, education and employment, as well as access to settlement support and social inclusion policies in host countries.
Conclusion
Most refugee children are functioning well and have normal social-emotional well-being 2–3 years postarrival. Cumulative protective factors can predict social-emotional well-being in newly arrived refugee children and some of these factors are modifiable. The ecological model17 provides a helpful conceptual framework as it emphasises that children develop in a social context in which family, community and society contribute to the quality of daily life. The use of this model and specific study findings justify exploration of policies such as the promotion of supportive educational environments and community integration initiatives.2 12 Elucidation of modifiable protective factors also allows the clinician to mobilise adaptive systems within the child, family and community.
Acknowledgments
The authors acknowledge participating families and children, Refugee Health Nurses Jenny Lane, Colleen Allen and Lisa Atkins, paediatric fellows Janka Paprckova, Meredith Sissons and Marion Mateos, and Statistician Jenny Peat.
References
Footnotes
Funding This study was funded by Foundation Markets Foundation for Children ($A158 000 July 2009–June 2011) and the South Eastern Sydney Multicultural Health Service ($A80 000 July 2012–June 2013). The funders had no involvement in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study received ethical approval from the Human Research Ethics Committee Northern Hospitals Network, South Eastern Sydney Illawarra Area Health Service (HREC Ref No 09/163).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data on this study that may not be published are available from the authors upon request.