Article Text

Abstract
Background Thyrotoxicosis is both rarer and more severe in children than in adults, rendering management difficult and often unsatisfactory.
Objective To ascertain outcome in a geographically defined area of Scotland between 1989 and 2014.
Method Retrospective case note review with follow-up questionnaire to family doctors for patients with Graves’ disease and Hashimoto’s thyroiditis.
Results Sixty-six patients (58 females:8 males) comprising 53 with Graves’ disease and 13 with Hashimoto’s thyroiditis were diagnosed at median 10.4 (2.9–15.8) years and followed up for 11.8 (2.6–30.2) years. Antithyroid drug (ATD) therapy was stopped electively in 35 patients after 4.5 (1.5–8.6) years, resulting in remission in 10/13 Hashimoto’s thyroiditis and 10/22 Graves’ disease. Side effects occurred in 12 patients receiving carbimazole, six of whom changed to propylthiouracil; no adverse events occurred in the latter patients.
Second-line therapy was given to 37 patients (34 with Graves’ disease), comprising radioiodine (22) at 15.6 (9.3–24.4) years for relapse (6), poor control/adherence (14) or electively (2); and surgery (16) at 12 (6.4–21.3) years for relapse (4), poor control/adherence (5) and electively (7). Adherence problems with thyroxine replacement were reported in 10/33 patients in adulthood.
Conclusions Hashimoto’s thyroiditis should be distinguished from Graves’ disease at diagnosis since the prognosis for remission is better. Remission rates for Graves’ disease are low (10/53 patients), time to remission variable and adherence with both ATD and thyroxine replacement often problematic. We recommend (a) the giving of long-term ATD rather than a fixed course of treatment in GD and (b) meticulous and realistic counselling of families from the time of diagnosis onwards.
- Endocrinology
- Pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Thyrotoxicosis is rarer and more severe in children and adolescents than in adults, with lower remission rates after antithyroid drug treatment.
Management of paediatric thyrotoxicosis is controversial, particularly concerning the length of time that antithyroid drugs should be administered.
What this study adds?
Thyrotoxicosis caused by the hyperthyroid phase of Hashimoto’s thyroiditis must be carefully distinguished from Graves’ disease since the former carries a better prognosis for spontaneous remission.
Time taken for Graves’ disease to remit is too variable for a standard interval (eg, 2–3 years) for stopping antithyroid treatment to be set.
Adherence difficulties are common not only before but also after second-line treatment when long-term thyroxine replacement is required. This has implications for management, including the initial education and counselling of families.
Introduction
Child and adolescent thyrotoxicosis is both less common and more severe than in adults.1 As a result, its management is controversial and often unsatisfactory.2–4 Treatment guidelines have been published in Japan, but these relate exclusively to Graves’ disease.5
A 12–18-month course of antithyroid drug (ATD) has been reported to result in remission in roughly 50% of patients.6 In adult practice, it is common to treat with ATD for this period before checking to see if remission has occurred.7 8 However, prolonged low-dose ATD administration has been shown to prevent relapse of Graves’ disease in adults >35 years of age.9
The American Thyroid Association acknowledges that the treatment of children with Graves’ disease varies considerably but states that medical therapy for 1 year is ‘still considered first line treatment for most children’.10 By contrast, Lippe et al quote a 25% per 2-year remission rate in paediatric Graves’ disease and support the approach of awaiting remission rather than stopping treatment at a defined time period in order to assess disease status.11 More recently a study of 154 French children with Graves’ disease showed a cumulative remission rate of 20% after 4 years, rising to 49% after 10 years.12 Rivkees has highlighted the potential hazards of ATD therapy, particularly with propylthiouracil (PTU).4
In 2005, the British Society for Paediatric Endocrinology and Diabetes (BSPED) launched a study examining outcome of thyrotoxicosis in patients treated with either dose titration (DT) or the block and replace (BR) regime, stopping therapy at 3 years to assess remission status.13 The purpose of our study was to examine the outcomes of an unselected Scottish population of children and adolescents with thyrotoxicosis in relation to aetiology, duration of treatment, achievement of spontaneous remission and adherence both with short-term ATD and long-term thyroxine replacement.
Patients and methods
The case notes of patients diagnosed with thyrotoxicosis under the age of 16 years in Greater Glasgow, Ayrshire & Arran, Argyll and Clyde and Lanarkshire between 1989 and 2012 were reviewed. Clinical and biochemical features and outcome in relation to treatment were documented. In April 2015, a questionnaire was sent to the patients’ family doctors requesting information on current thyroid status, treatment with ATD or thyroxine replacement, adherence with medication and the development of additional disorders.
Biochemical parameters studied included free thyroxine (fT4) and total T4 (TT4), the former largely replacing the latter by 2000; total tri-iodothyronine (T3); thyroid-stimulating hormone (TSH); antimicrosomal and thyroid peroxidase (TPO) antibodies, the latter replacing the former in 1999. Assays for these hormones and antibodies were carried out using commercial kits. TSH receptor antibody (TRAB) was initially measured as percentage displacement of TSH binding using an in-house assay as described by Wilson et al.14 From 1999, this assay was replaced by THYBIA TSH-receptor antibody RIA kit manufactured by Diasorin. Intra-assay and inter-assay coefficients of variation were <6% and <14%, respectively, at 20 and 45 U/L.
Thyrotoxicosis was defined as elevated thyroid hormones: free T4 >30 pmol/L or TT4 >160 nmol/L, T3 >3 nmol/L with TSH <0.1 mU/L, in a patient with clinical symptoms of thyrotoxicosis (eg, heat intolerance, increased sweating, palpitations and weight loss).
Specific criteria were set to distinguish between Graves’ disease and Hashimoto’s thyroiditis. Graves’ disease was defined as thyrotoxicosis with either eye signs or elevated TSH receptor antibodies (either ≥10% displacement of TSH binding or ≥10 U/L) with or without positive thyroid autoantibodies or both. Hashimoto’s disease was defined as thyrotoxicosis, usually with positive antithyroid antibodies—antimicrosomal antibody titre >1/400, anti-TPO antibodies>30 mU/L; in the absence of both eye signs and elevated TSH receptor antibodies. Presence of antithyroid antibodies was not a prerequisite for the diagnosis of Hashimoto’s disease since organ-restricted disease may occur.15 Patients with neonatal thyrotoxicosis and hyperthyroidism associated with dysmorphic syndromes were excluded.
Thyroid size, assessed clinically and supplemented where available by ultrasound measurements and clinical photographs, was graded as normal, and small, moderate or large goitre. Thyroid ophthalmopathy was defined clinically as absent; mild when the patient had some lid retraction and was considered by the family to have developed slight prominence of the eyes; moderate when there was clinically obvious orbital projection—exophthalmos; and severe when eye prominence was so obvious as to be unsightly, with or without oedema and injection of the conjunctivae.
ATD treatment was recorded according to type—carbimazole or PTU; mode—ATD alone (DT) or ATD with thyroxine (BR). Duration, side effects, adherence and date/age of stopping treatment were also recorded.
Remission was defined as no recurrence of thyrotoxicosis during the study period (end of July 2015) following cessation of ATD and relapse as recurrence of thyrotoxicosis at any time off treatment.
Continuous variables were described as median and ranges, and intergroup comparison was performed using Mann–Whitney U tests. χ2 test was used for categorical variables. P < 0.05 was considered to be statistically significant, and all analyses were performed using Minitab V.17.
Results
Between 1989 and 2012 inclusive, 77 patients with thyrotoxicosis were seen, of whom 11 were ineligible for the following reasons: Down (4) and DiGeorge syndrome (1), neonatal Graves’ disease (4), Hashimoto’s encephalopathy with incipient untreated hyperthyroidism (1) and case sheet unavailable (1). Three of the eligible 66 patients shown in table 1 were of Indian, Pakistani and Ghanaian origin, the remainder were Caucasian. Two patients were referred to ophthalmology with severe proptosis, both of whom were managed conservatively.
Clinical and biochemical features at diagnosis of 66 patients with thyrotoxicosis in the west of Scotland seen between 1989 and 2012 with a diagnosis of Graves’ disease or Hashimoto’s thyroiditis
Median (range) age at diagnosis and age on 1 January 2016 was 11.8 (2.8–16.9) and 25 (13.7–39.7). Excluding three patients lost to follow-up at 1.3, 2.4 and 4 years median (range) duration of follow-up was 11.8 (2.6–30.2) years. In total, 53 patients (45 girls: 8 boys) satisfied the criteria for Graves’ disease, and 13 patients (all girls) had Hashimoto’s disease. Patients with Hashimoto’s thyroiditis were older (P=0.01) with lower free T4 (P =0.02) than those with Graves’ disease.
Associated disorders in Graves’ disease comprised diabetes mellitus which had developed after diagnosis in four girls and pauciarticular juvenile idiopathic arthritis developing before diagnosis in one. Two patients with Hashimoto’s disease developed systemic lupus erythematosus and mild Behçet’s syndrome in adulthood.
Completed questionnaires were received from 43 (66%) family doctors. Eleven patients had changed their thyroid status with development of diabetes mellitus (one), relapse of Graves’ disease (three) and development of hypothyroidism (six). Of the 23 patients in whom questionnaires were not received, 10 were known to be on thyroxine replacement following radioiodine (5) or surgery (5) while thyroid and treatment status was known in a further 4 patients up to the end of 2014 leaving 9 patients in whom thyroid status could not be confirmed. Also, 5 of the 48 patients had had nine children, including a twin pregnancy in which one baby was stillborn.
Outcome with ATD therapy

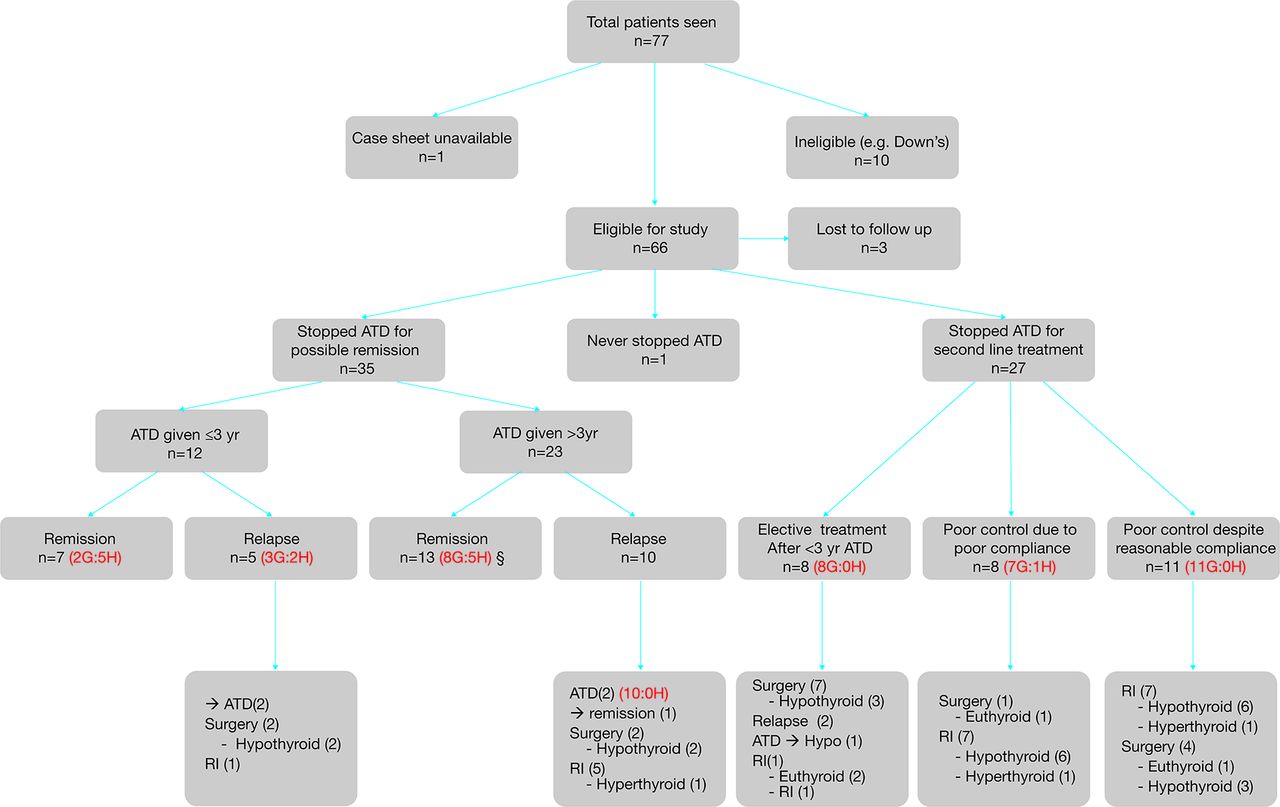{kind=link}
Flow diagram showing outcome in 77 children and adolescents with thyrotoxicosis seen in the west of Scotland 1989-2012. ATD, antithyroid drugs; GD, Graves’ disease; HT, Hashimoto’s thyroiditis; RI, radioiodine therapy.
Clinical and biochemical features relating to outcome in 35 of 66 patients with thyrotoxicosis, diagnosed in the west of Scotland between 1989 and 2012 who stopped antithyroid drug (ATD) treatment for possible remission prior to treatment with either surgery or radioiodine therapy
All patients received carbimazole initially using DT in 46 and BR in 20. Apart from the seven patients who were enrolled into the BSPED trial, there was no standard protocol for stopping ATD during the study period. Three patients were lost to follow-up after 4, 2.4 and 1.3 years. Adverse events associated with ATD were seen in 12 patients receiving carbimazole comprising rash (n=5), neutropenia (n=2) and sore throat (n=4). Six patients were switched to PTU with no reported side effects. One patient with Graves’ disease remained on ATD throughout the study period from 2.9 to 22 years.
Thirty-five patients (23 Graves’s; 12 Hashimoto’s) stopped ATD for possible remission, and their data are shown in table 2. Also, 12 had been treated for <3 (range 0.65–2.96) years and 23 for ≥3 (range 3.7–14.7) years.
Also, 20 patients (10 Graves’; 10 Hashimoto’s) remitted after 4.2 (0.5–8.9) years (n=17, duration unknown in 3), while 15 (13 Graves’; 2 Hashimoto’s) relapsed. Cause of thyrotoxicosis and total (but not free) T4 at presentation were the only significant differences between the two groups.
Outcome with second-line treatment
See figure 1.
Twenty-seven patients stopped ATD to receive second-line treatment; for poor disease control in 19 (associated with known adherence difficulties in 11) and pending elective treatment in 8.
Surgical treatment
Sixteen patients underwent thyroidectomy, the type being at the discretion of the surgeon responsible. Subtotal thyroidectomy was performed in 12 patients between 1992 and 2003 at 12 (6.4–20.2) years with recurrence in 2, remission in 2 and hypothyroidism in 8. Total thyroidectomy was performed in four patients between 2006 and 2014 at 12.9, 18.7, 20.1 and 21.3 years with hypothyroidism in all, and permanent hypoparathyroidism in the youngest patient. Keloid formation was seen in two patients.
Radioiodine treatment
Twenty-two patients received radioiodine in the dose of 450 (250–500) MBq at 15.6 (9.3–24.4) years. All but two became hypothyroid, mostly within 6 months of therapy. One patient with Graves’ disease required a second dose while two remained hyperthyroid, one diagnosed at 5.5 years and treated at 10.3 years for poor control who subsequently received BR therapy; the other diagnosed at 9.2 years and treated at 18.5 years and who remained off treatment with mild thyrotoxicosis.
Long-term follow-up
By the end of the study period, 33 of the 66 patients were known to be on thyroxine replacement. For these patients, adherence with treatment was not stated in 14, reported as reasonable or good in 9 and as poor in 10 with most recent TSH >20 mU/L in 3.
Discussion
This study of patients with paediatric thyrotoxicosis in the west of Scotland over a 25-year period has enabled long-term outcome to be assessed. It is of note that no serious side effects occurred during the 26 years of this regional study including none with PTU, although this medication should be avoided where possible in children.4 6
Inevitably, a study such as ours is limited by its retrospective nature and in particular the lack of a standard protocol, particularly concerning duration of treatment with ATD. Moreover, assessment of ophthalmopathy and thyroid enlargement was subjective. The relatively high prevalence (46/53) of eye signs in children with Graves’ disease compared with some studies16 may be explained by inclusion of mild signs such as lid lag rather than true proptosis. Of note, no patient developed eye disease of sufficient severity for steroid therapy or surgery to be contemplated.
This study highlights the importance of distinguishing between Hashimoto’s thyroiditis and Graves’ disease at presentation of hyperthyroidism. Many studies have focused on Graves’ disease alone as the cause of hyperthyroidism1–8 11 with some not mentioning Hashimoto’s disease in the differential diagnosis.6 8 The American Thyroid Association guidelines describe ‘painless thyroiditis caused by lymphocytic inflammation’ and refer to its variable prevalence from 0.5% to 22% in different studies.10 An absolute distinction between the two disorders may be difficult; indeed some workers consider them to be at different ends of a continuum.17 However, the criteria applied in this study have proved clinically useful. Thus of 13 (19.6%) patients classified as Hashimoto’s thyroiditis in our study, 10 remitted spontaneously in contrast with only 10 documented remissions in the 56 patients with Graves’ disease.
Since differentiation between Hashimoto’s thyroiditis and Graves’ disease requires thyroid receptor antibody measurement, the results of which will be received some time after the initial thyroid function tests, it is the clinician’s responsibility to ensure that these results are pursued so that the family can be counselled appropriately.
The question of duration of ATD is contentious. It has been argued that there is no evidence from randomised trials that prolonging medical treatment increases the chance of remission in Graves’ disease.18 However, the disease has a natural history of remission in some cases, one study showing spontaneous remission in 8 of 26 patients treated with propranolol alone.19 Léger et al showed evidence for cumulative increase in remission rates in children given repeated 2-year courses of treatment.11 A more recent study from Japan has reinforced this finding, with remission in 334/639 (46.2%) of children and adolescents (median age 16 years) with Graves’ disease, and an increasing prevalence of remission with the duration of ATD treatment.20 Moreover, restoring euthyroidism in itself minimises thyroid autoimmunity and increases the chance of remission.21 22 In our study, the number of patients with Graves’ disease achieving spontaneous remission was insufficient and the patient population was not treated in systematic and defined courses to allow calculation of a cumulative incidence of remission. However, our data do not support the implementation of a set cut-off time, for example, 3 years, for assessing remission off therapy. Rather, they are consistent with Léger’s recommendation that ‘continuous treatment, rather than treatment cycles of 2 years should be considered in future clinical trials’.’12
This study did not attempt to address the question of ATD regime—BR versus DT. The current evidence in adults favours DT since BR involves a higher ATD dose and hence a higher prevalence of adverse effects, with no proven benefit in terms of achieving remission.23 However, BR has the advantage of requiring less frequent monitoring and more consistent maintenance of euthyroidism than DT.24 The outcome of the BSPED prospective study should help to clarify this controversy.
A major problem encountered in this study is that of adherence both with ATD treatment and thyroxine replacement. Poor adherence with ATD was documented in at least 11 of the 27 patients receiving second-line treatment and might have been a factor in others with poor disease control. In adulthood, 10 of the 33 patients known to be on long-term medication with thyroxine were reported by their family doctors as having problems—a serious matter for women of childbearing age.25 Thus there is a risk that adherence problems with ATD may be exchanged for problems with long-term thyroxine replacement with ablative second-line treatment. Of note, the only patients receiving second-line therapy in this study to achieve remission were 2 of the 12 undergoing subtotal thyroidectomy. Although total rather than subtotal thyroidectomy is favoured in adult patients26 partly because of relatively high recurrence rates of 5.3% and 7.9% with the latter,27 28 this option might be considered for patients with a particularly poor track record of adherence to ATD treatment.
In conclusion, we advocate precise diagnosis followed by careful and realistic counselling in paediatric thyrotoxicosis. Families should be warned that ATD treatment may be required for many years in Graves’ disease; that the number of years of ATD treatment cannot be predicted and that if second-line treatment such as radioiodine and surgery is given lifelong treatment with thyroxine is almost always needed. Reduction in ATD dosage should be cautious and slow before testing for remission.6 With uncontrolled Graves’ disease, early recourse to second-line treatment will avoid years of educational disruption but adherence may remain a problem. The culture of daily tablet-taking at the same time of day should be encouraged, and we would reinforce the need for continuing education of the patient and family in clinic.12
References
Footnotes
Contributors Data for the study were collected by MK, MAT and SMcG, with help from the consultants caring for the patients: GS, SW and SFA. MDCD and MK devised the patient questionnaire and collated the results. MK carried out the analysis of data and wrote the paper with MDCD. All authors read and approved the final manuscript.
Competing interests None declared.
Ethics approval The research and development departments of National Health Service (NHS) Glasgow & Clyde, Ayrshire & Arran and Lanarkshire were informed of and approved the study. NHS Lanarkshire requested and obtained Caldicott Guardian approval. The study was registered as a quality improvement project with NHS Greater Glasgow and Clyde Clinical Governance unit.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial