Article Text

Abstract
We performed a quality improvement initiative to reduce unnecessary treatments for acute bronchiolitis (AB) in primary care (PC) and the referral paediatric emergency department (ED). The quality improvement initiative involved two seasons: 2016–2017 (preintervention) and 2017–2018 (postintervention). We distributed an evidence-based protocol, informative posters and badges with the slogan ‘Bronchiolitis, less is more’. We also held interactive sessions, and paediatricians received weekly reports on bronchodilator prescription. The main outcome was the percentage of infants prescribed salbutamol. Secondary outcomes were epinephrine, antibiotic and corticosteroid prescription rates. Control measures were ED visit and hospitalisation rates, triage level, length of stay, intensive care admission and unscheduled returns with admission. We included 1878 ED and 1192 PC visits of which 855 (44.5%) and 534 (44.7%) occurred in the postintervention period, respectively. In the ED, salbutamol and epinephrine prescription rates fell from 13.8% (95% CI 11.8% to 16%) to 9.1% (95% CI 7.3% to 11.2%) (p<0.01) and 10.4% (95% CI 8.6% to 12.4%) to 9% (95% CI 7.2% to 11.1%) (n.s.), respectively. In PC, salbutamol, corticosteroid and antibiotic prescription rates fell from 38.3% (95% CI 34.6% to 42.0%) to 15.9% (95% CI 12.9% to 19.5%) (p<0.01), 12.9% (95% CI 10.5% to 15.7%) to 3.6% (95% CI 2.2% to 5.7%) (p<0.01) and 29.6% (95% CI 26.2% to 33.2%) to 9.5% (95% CI 7.2% to 12.5%) (p<0.01), respectively. No significant variations were noted in control measures. We safely decreased the use of unnecessary treatments for AB. Collaboration between PC and ED appears to be an important factor for success.
- quality improvement
- bronchiolitis
- treatments
- children
- pediatric emergency department
- primary care
Statistics from Altmetric.com
What is already known on this topic?
Although evidence-based guidelines for acute bronchiolitis recommend primarily supportive care, many unnecessary treatments remain well documented, contributing to a care quality problem of overtreatment.
What this study adds?
As our baseline use is probably comparable with current practice in other emergency department and primary care settings, our findings have implications for similar health areas wanting to undertake projects to improve the management of acute bronchiolitis.
Introduction
Acute bronchiolitis (AB) is the most common reason worldwide for non-elective hospital admission in infants <1 year of age.1 Although evidence-based guidelines recommend primarily supportive care,2 3 many unnecessary treatments remain well documented, contributing to a care quality problem of overtreatment.4 5 In addition, despite the high incidence, increasing morbidity and significant economic impact of AB, there is still great variability in clinical practice, both in the diagnosis and management of this illness.6–8
The implementation of evidence-based clinical practice guidelines (CPGs) has been reported to result in reductions in diagnostic and therapeutic resource use and improvements in clinical outcomes.9 10 Nevertheless, CPG implementation is complex, and there is still a gap between the evidence available and clinical practice.11–13 Specifically, despite a lack of supporting evidence, there continues to be a substantial amount of unnecessary testing and treatments with potential side effects and higher costs.13 14
Quality improvement (QI) initiatives implemented in response to overtreatment problems have been shown to decrease the use of non-evidence-based therapies and testing and also provide achievable benchmarks of care for clinical quality indicators, especially in hospital settings.14–17 Nonetheless, less evidence is available from other settings, such as primary care (PC), where standardising treatment also requires a multifaceted approach, which is still a challenge.17
The objective was to implement and assess a QI initiative to reduce the overuse of unnecessary treatments in infants with AB in PC settings and the referral paediatric emergency department (ED).
Patients and methods
Setting
We conducted a QI initiative, evaluating the use of pharmacotherapies in children diagnosed with bronchiolitis, in two health districts and the referral paediatric ED.
Our healthcare system provides comprehensive, free and universal coverage. The two health districts involve 20 PC centres with 39 paediatricians who care for 36 412 children, of whom 6371 (17.5%) are infants under 2 years old. The region where the study was carried out has two other health districts with 30 PC centres in which no interventions were performed.
The referral paediatric ED is located in an acute care teaching tertiary hospital near Bilbao, in the Basque Country (Spain). This department provides care to children under 14 years old, with a mean of 60 000 emergency visits a year. Around 2% of these visits are due to AB. There is an observation unit in the ED, which is a 24-hour unit with 10 beds, staffed by paediatric emergency physicians.
We executed this QI initiative over two AB seasons: October–March of 2016–2017 (preintervention period) and October–March of 2017–2018 (postintervention period). All children under 2 years old with a diagnosis of bronchiolitis, defined as the first presentation with a viral respiratory tract infection with respiratory distress,3 were included, regardless of whether they had comorbidities (lung or congenital heart disease, immunodeficiency, neuromuscular, neurological or genetic disease). Exclusion criteria were a previous diagnosis of bronchiolitis ≥1 month before the index episode.
Interventions
We assembled a multidisciplinary team, which consisted of paediatric PC physicians, paediatric emergency physicians, paediatric residents, paediatric nurses, nurses’ aides and a clinical epidemiologist. A kickoff meeting was held to review data from previous bronchiolitis seasons and develop interventions (figure 1). A multifaceted plan was conducted in order to increase compliance with the CPGs and reduce unnecessary treatments in PC and the referral ED:

Key driver diagram. This tool displays the primary drivers (centre) or system factors affecting the project outcome listed in the aim (left). The interventions that were employed to address each primary driver are shown (right). AB, acute bronchiolitis; ED, emergency department; PC, primary care; CGs, clinical guidelines.
Educational campaign
Several briefings sessions were held, with staff and residents, informing them about the updates in our management protocol. In addition, we developed monthly interactive sessions with online data collection and feedback. The interactive sessions mainly consisted of reviewing the existing evidence on the treatment of AB and discussing barriers to applying what is known about this disease.
Informative tools
During epidemic months, informative posters for staff and families were placed in the common work area and also in the waiting room. Badges for uniforms with the project slogan ‘Bronchiolitis, less is more’ were distributed to staff.
Feedback on updated clinical quality indicators to paediatricians
Paediatricians received a weekly report with personal and global data on the prescription of bronchodilators in PC settings and the ED. In addition, they received monthly emails comparing their individual bronchodilator use rates to those of their unidentified peers.
Furthermore, global clinical quality indicators related to AB, such as rates of admission and unscheduled visits to the ED, were periodically updated and circulated via email to all paediatricians.
Update alerts in electronic health records
The option for a trial of bronchodilators was removed from the report templates associated with the diagnosis of bronchiolitis in the ED. Instead, reminder messages for clinicians were included about the recommendation on restricting the prescription of salbutamol.
Information for families
At the time of discharge, families were given an updated fact sheet with information on bronchiolitis including techniques of nasal washing and suctioning and how to recognise signs of distress.
Data collection system
A computerised search tool was used to identify patients with International Classification of Diseases-9 or 10 codes related to bronchiolitis for the respective time periods of data collection.
Demographic, clinical and medical prescription data were collected from the computerised database system of the Basque Health Service. Informed consent from parents was not considered necessary because the children did not undergo any interventions related to this study, and data were handled anonymously.
Outcome measures
The primary outcome measure was the rate of infants with AB receiving salbutamol in the ED and the rate of prescription of salbutamol in PC settings.
Secondary outcomes evaluated were the rate of infants with AB receiving epinephrine, antibiotics and corticosteroids and the use of X-ray in the ED and the rate of prescription of antibiotics and corticosteroids in PC settings.
To evaluate the possible unintended consequences of decreasing interventions, we studied several balance outcome measures, defined as followed:
Balance measure 1: overall rate of hospital admission.
Balance measure 2: rate of paediatric intensive care unit (PICU) admission.
Balance measure 3: length of stay in the ED.
Balance measure 4: rate of unscheduled returns within 72 hours.
Balance measure 5: rate of unscheduled returns with admission within 72 hours.
In addition, we obtain the rate of salbutamol prescription in PC settings during the two AB seasons for health areas in which no QI initiatives were performed.
Statistical analysis
Quantitative data were expressed as means and SD or medians and IQRs, depending on the distribution of the variables, and categorical variables using frequencies and percentages. Shewhart P charts18 were used to continuously evaluate outcome measures during the intervention phase. On each P chart, we plotted the outcome of interest on the vertical axis versus time on the horizontal axis. Each data point represents 7 days of data, and data from outside of bronchiolitis season were not included in the analysis. The control limits were based on the binomial distribution of proportions, as indicated when an outcome is not rare. The timing of each intervention is indicated on the charts.
Associations between qualitative variables were assessed using the χ2 test. Comparisons between variables with a normal distribution were made using the Student’s t-test. The level of statistical significance chosen was p<0.05. We carried out the statistical analysis using IBM SPSS Statistics for Windows (V.23).
Results
Population characteristics
During the study period, 1878 episodes of AB were recorded in the ED (1023 in the preintervention period and 855 in the postintervention period) and 1192 in PC centres participating in the initiative (658 and 534, respectively). Among the episodes seen in the ED, 392 (38.3%) in the preintervention season and 333 (38.9%) in the postintervention season came from the PC centres in which the interventions were performed. Overall, 1636 (87.1%) episodes seen in the ED and 888 (74.5%) episodes seen in PC settings were under 12 months of age, without significant differences between the two AB seasons.
Outcome measures
In the ED, there was a fall in the percentage of infants receiving salbutamol from 13.8% (95% CI 11.8% to 16%) to 9.1% (95% CI 7.3% to 11.2%; p=0.01) (figure 2) and epinephrine from 10.4% (95% CI 8.6% to 12.4%) to 9% (95% CI 7.2% to 11.1%; not significant). The use of antibiotics did not vary significantly (2.4%; 95% CI 1.6% to 3.5% vs 3.1%; 95% CI 2.1% to 4.5%). The use of corticosteroids was less than 1% in the ED. The rate of X-ray did not vary significantly (7.7%; 95% CI 6.2% to 9.5% vs 7.8%; 95% CI% 6.2 to 9.8%).

P chart showing decrease in the percentage of infants receiving salbutamol in the emergency department after implementation of the QI initiative. QI, quality improvement.
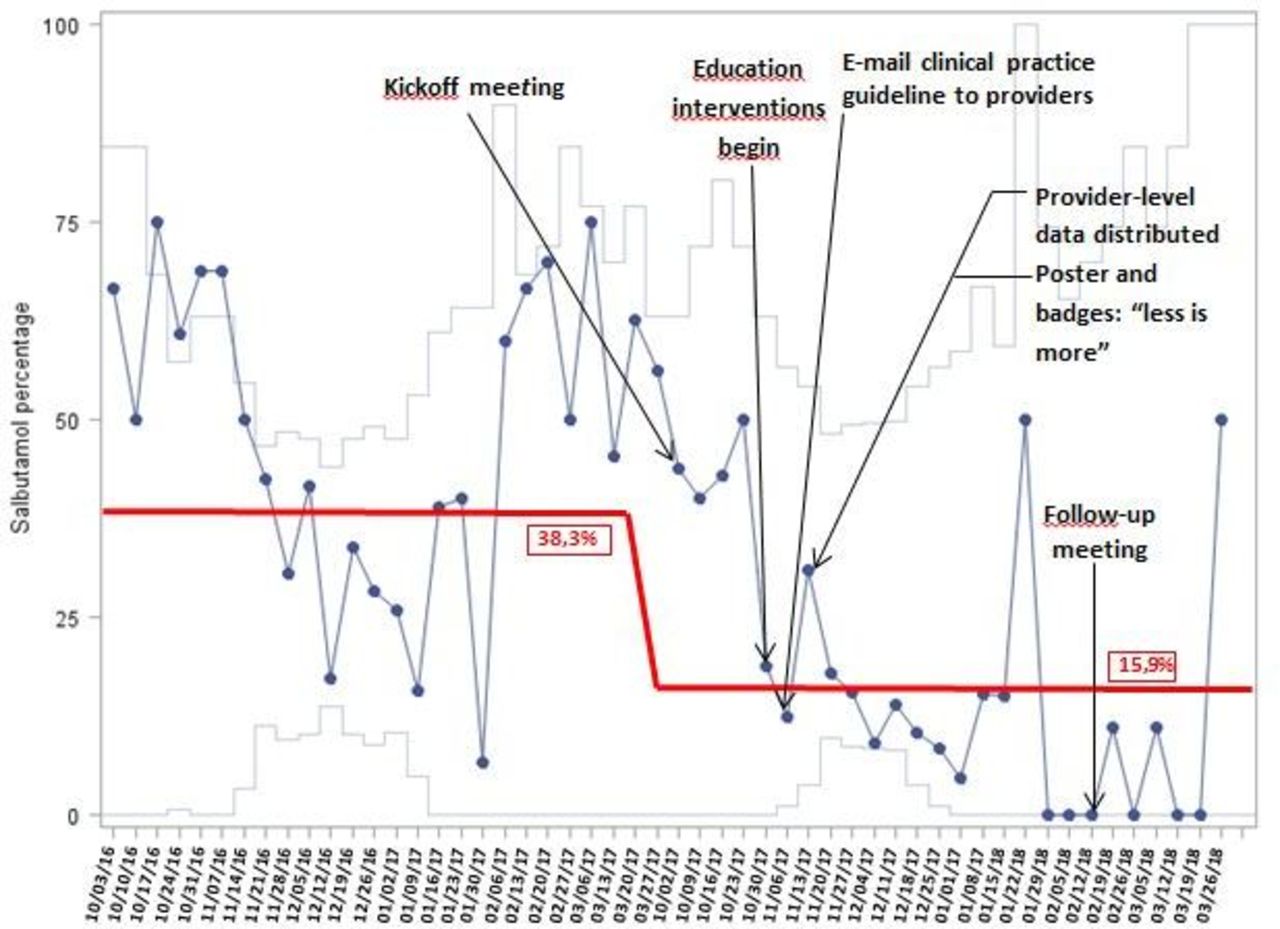
In PC settings, the rates of prescription of salbutamol, corticosteroids and antibiotics fell from 38.3% (95% CI 34.6 to 42.0%) to 15.9% (95% CI 12.9% to 19.5%) (p<0.01) figure 3, from 12.9% (95% CI 10.5% to 15.7%) to 3.6% (95% CI 2.2% to 5.7%) (p<0.01) and from 29.6% (95% CI 26.2% to 33.2%) to 9.5% (95% CI 7.2% to 12.5%) (p<0.01) (table 1), respectively. The decrease in the use of salbutamol occurred in the 20 PC settings where the intervention was performed with great variability in the prescription rates (online supplementary figure).
Supplemental material
Comparison of outcome measures for patients seen in the emergency department and patients seen in the primary care settings where the intervention was carried out in the preintervention and postintervention acute bronchiolitis seasons

{kind=link}
{kind=link}
{kind=link}
P chart showing decrease in the percentage of infants prescribed salbutamol in the primary care settings after implementation of the QI initiative. QI, quality improvement.
Prescription rates of salbutamol in the preintervention and postintervention periods depending on age and acuity level at ED triage are shown in an online supplementary table.
Supplemental material
A total of 1348 and 1225 episodes were diagnosed with AB in the PC centres from the two health districts without intervention in the 2016–2017 and 2017–2018 seasons, respectively. The overall salbutamol rate in these PC settings in the 2017–2018 AB season was significantly higher than those observed in PC settings from the health areas participating in the interventions (32.4%; 95% CI 29.9% to 35.1% and 15.9%; 95% CI 13.0% to 19.2%, respectively; p<0.01). The overall prescription rate of salbutamol in these two areas in the preintervention AB season was similar than those observed in the intervened areas (33.6%; 95% CI 31.1 to 36.1% and 38.3%; 95% CI 34.6 to 42.0, respectively; p=0.04).
Balancing measures
In brief, there was no change in the overall rates of hospitalisation, PICU admission, revisits or readmissions and length of stay in the ED after the interventions (table 2).
Balance measures for episodes seen in the emergency department in the preintervention and postintervention acute bronchiolitis seasons
A total of 553 and 622 episodes were diagnosed with asthma in the ED in children under 2 years old in the 2016–2017 and 2017–2018 AB seasons, respectively.
Discussion
Our coordinated, multisite, multidisciplinary QI initiative significantly reduced the use of bronchodilators in children seen in PC settings and the ED for bronchiolitis without unintended consequences, such as hospitalisations, ED revisits, readmission or escalation of care in the PICU. To our knowledge, this is the first QI project in which researchers simultaneously implement improvement initiatives in PC and the corresponding hospital ED. Given that our baseline use is probably comparable with the current practice in other ED and PC settings, our study has implications for other similar health areas that want to undertake projects for the improvement in the management of AB.
Previous studies conducted in hospital settings have demonstrated the usefulness of implementing QI measures at a local level or with collaboration between different settings to improve the management of AB.14 19 20 A study conducted by Ralston et al to assess a collaborative multicentre strategy19 found a significant decrease in the use of bronchodilators and corticosteroids after the dissemination of the AAP guidelines and education through interactive webinars. Similarly, multifaceted educational bundles, such as the one described by Murch et al,21 can significantly improve adherence to guidelines. However, there is little knowledge about the use of pharmacotherapy and improvement initiatives for the management of bronchiolitis at the PC level. A study carried out in our area in 2017 showed a high use of bronchodilators and other medications in bronchiolitis in PC.7 In the same study, the authors showed that the implementation of a QI intervention was successful in reducing the use of pharmacotherapy in AB in PC settings. Nonetheless, they found that more than 30% of infants with AB continued to be treated with bronchodilators and other medications. A lack of knowledge of real-time data about the prescription of medications throughout AB season and the lack of communication between paediatricians working in PC settings can partially explain the difficulties of achieving a better result with the initiative undertaken.
The persistence of this high use of pharmacotherapy in our area was the main reason for carrying out the present study. Taking into account the experience accumulated during the previous improvement initiative, we planned a new QI cycle. For this new initiative, we decided to maintain the same objective, namely, to reduce the use of medications but incorporate new improvement measures. As has been observed in other disease processes, showing clinicians their performance data compared with peers likely positively influences their behaviour.22 23 In our study, the combination of having regular information on prescription data in the different PC settings and the ED and seeing individualised data may have effectively influenced clinician management decisions. Furthermore, initiatives to keep our project goals visible such us the placement of posters in the ED and PC centres and badges for staff uniforms with the project slogan ‘Bronchiolitis, less is more’ may have played a role in reducing the overuse of medication in AB.
Nonetheless, we think it is likely that the factor that has had the greatest impact on the results of our improvement initiative has been the collaboration between the ED and PC. It has been shown that a lack of consensus between different levels of healthcare increases variability in clinical practice.24 Since bronchiolitis lasts a minimum of 1–2 weeks, it is not unusual for patients with this disease to consult several times in different settings. This can increase the likelihood that a medication will be finally prescribed in one of these consultations. We believe that the global agreement on not using medications has been decisive in the success of our initiative.
Given the seasonal nature of AB, the lack of a control group has been noted as a limitation in ascertaining whether results obtained after an intervention are due to the improvement measures taken between two AB seasons.22 For the present study, we obtained data on the prescription of salbutamol in health districts in which no interventions were performed and these show high use of salbutamol, similar to that found in our study prior to the implementation of the improvement measures. This fact reinforces the conclusion that the results of our study are likely to be attributable to the interventions performed. However, our study shows that the results obtained after the improvement initiative carried out in a referral hospital do not imply a change in clinical practice in their geographical area of influence. In fact, despite the low use of salbutamol in the ED, PC settings without the interventions continued to have a high salbutamol prescription rate. This phenomenon has previously been described in the literature in relation to other disease processes. For example, while some studies have shown a decrease in the use of CT in paediatric head trauma in some North American hospitals,25 another reflects the lack of changes across the whole country in the same period of time.26
Limitations
Our study has various limitations. First of all, it only included two PC health districts and differences between these and those of other healthcare systems could lead to the same interventions having different outcomes elsewhere. Second, since we only obtained data on drug prescriptions for at-home use and did not investigate the potential administration of bronchodilators at the time of the PC visit, we may have underestimated pharmacological treatment overall. We believe that this potential underestimation would not, however, affect the primary outcome of these interventions, which is the decrease in prescription. Third, we did not review patient health records to assess whether clinicians used the McConnochie criteria for the diagnosis of AB,27 as recommended by the established protocol, and hence, differences between professionals in the diagnostic criteria applied could have led to differences in individual prescription rates. Lastly, fewer patients were diagnosed with bronchiolitis and more with asthma in the postintervention period. This fact could indicate a change in the diagnostic criteria of paediatricians and explain part of our results. Although some first wheezing episodes could be diagnosed with asthma, to justify bronchodilator treatment, we believe that repeated episodes of wheezing diagnosed with bronchiolitis in the preintervention period are more likely to be diagnosed with asthma in the postintervention period. It is important to note that one of the interventions carried out was to update the diagnostic criteria of bronchiolitis.
Future directions
To achieve greater applicability in different healthcare environments, future improvement projects should include the experience of families and professionals with the global process of bronchiolitis.28
Future research should explore provider attitudes, differences in acceptability by provider type, unintended consequences and the effectiveness of the collaboration between different steps of healthcare. Finally, studies in which researchers use implementation methodology are needed to determine which of our interventions were most effective in changing provider behaviour for which patients and through which mechanisms.29
Conclusions
Our QI intervention significantly reduced the prescription and overuse of medications in bronchiolitis in our health area without unintended consequences for patients. Collaboration between PC and ED appears to be an important factor for success.
References
Footnotes
Contributors MM conceptualised and designed the study, supervised data collection, analysed the data, wrote and critically revised the initial draft of the manuscript and approved the final manuscript as submitted. NP collaborated in the study design, wrote and critically revised the initial draft of the manuscript and approved the final manuscript as submitted. CS-H collaborated in the design of the study, participated in data collection and critically revised the manuscript. LM-I collaborated in the design of the study, analysed the data and critically revised the manuscript. SM collaborated in the design of the study, participated in data collection and critically revised the manuscript. JB conceptualised and designed the study, supervised data collection, analysed the data, wrote and critically revised the initial draft and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding Annual research grant from the Spanish Society of Pediatric Emergency Medicine in 2018.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committee of the Basque Country.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.