Article Text

Abstract
Background and objectives Recently, in adults, the incidence and severity of fatigue was found to exist rather independently from the somatic diagnosis. Since fatigue is distressing when growing up with a chronic disease, we aim to investigate: (1) the prevalence and extent of fatigue among various paediatric chronic diseases and (2) the effect of fatigue on health-related quality of life (HRQoL).
Design and setting Cross-sectional study in two children’s hospitals.
Patients Children and adolescents 2–18 years of age with cystic fibrosis, an autoimmune disease or postcancer treatment visiting the outpatient clinic.
Outcome measures Fatigue and HRQoL were assessed using the Pediatric Quality of Life Inventory (PedsQL) multidimensional fatigue scale (with lower scores indicating more fatigue) and PedsQL generic core scales, respectively. Linear regression analysis and analysis of covariance were used to compare fatigue scores across disease groups and against two control groups. The effect of fatigue on HRQoL was calculated. Data were adjusted for age, sex and reporting method.
Results 481 children and adolescents were assessed (60% participation rate, mean age 10.7±4.9, 42% men). Children and adolescents with chronic disease reported more fatigue than the general population (mean difference −6.6, 95% CI −8.9 to –4.3 (range 0–100)), with a prevalence of severe fatigue of 21.2%. Fatigue scores did not differ significantly between disease groups on any fatigue domain. Fatigue was associated with lower HRQoL on all domains.
Conclusions Fatigue in childhood chronic disease is a common symptom that presents across disease, age and sex groups. Fatigue affects HRQoL. Our findings underscore the need to systematically assess fatigue. Future studies should determine possible biological and psychosocial treatment targets.
- fatigue
- chronic disease
- autoimmune disease
- cystic fibrosis
- paediatric oncology
Statistics from Altmetric.com
What is already known?
Children with a chronic disease face several challenges that can include both somatic and psychosocial aspects.
Fatigue is often one such challenge and can have a significant impact on the well-being and participation in daily life of the child and his or her family.
In adults with chronic disease, the incidence and severity of fatigue was found to exist rather independently from the somatic diagnosis.
What this study adds?
Fatigue in childhood chronic disease is a common symptom that presents across disease, age and sex groups and affects quality of life.
Fatigue is highly prevalent—and therefore highly relevant—among children with chronic disease.
These results emphasise the need for systematic assessment of fatigue in children with chronic disease.
Introduction
Thanks to major advances in paediatric medicine, many paediatric diseases can now be stabilised or cured.1 As a result, children and adolescents with a chronic medical condition such as cystic fibrosis (CF) or an autoimmune disease, as well as children and adolescents who were successfully treated for a life-threatening disease with long-term consequences (eg, childhood cancer), often face several challenges while growing up; here, we define these conditions collectively as ‘childhood chronic diseases’. These challenges can include both somatic and psychosocial aspects.2 3 Fatigue is often one such challenge and can have a significant impact on the well-being and participation in daily life of the child or adolescent and his or her family.4–6
Recently, in adults, the incidence and severity of fatigue was found to exist rather independently from the somatic diagnosis.7 This emerging concept has not yet been studied in children and adolescents, although it has been reported that fatigue can persist despite low disease activity.7–9 In adolescence, fatigue is known to be more prevalent than in younger children and can partially be explained by physical and psychosocial changes in puberty, such as changing sleep patterns.10 Even though fatigue is generally recognised as a frequent and distressing symptom, the prevalence and extent of fatigue among various paediatric chronic diseases are currently unknown.8 9 11 Determining whether fatigue is a general rather than a disease-specific phenomenon is an important first step towards developing more general fatigue interventions. In children and adolescents, the ability to adequately assess and treat fatigue can improve their current well-being, as well as their future well-being and participation in daily life and can prevent fatigue from becoming persistent.12 13 Therefore, understanding the extent and nature of fatigue among various childhood chronic diseases is needed. To address this need, the primary aim of our study was to investigate the prevalence and extent of fatigue among children and adolescents with chronic disease and two control groups. In addition, we investigated the effect of fatigue on health-related quality of life (HRQoL).
Methods
Study design
A cross-sectional study was conducted in the outpatient clinics of the Wilhelmina Children’s Hospital and the Princess Máxima Center for Paediatric Oncology in the Netherlands, from December 2016 to September 2018. Fatigue in children and adolescents with a chronic disease was compared with fatigue in the general population as well as fatigue among children and adolescents with chronic fatigue syndrome (CFS).10 This study was classified by the institutional review board as exempt of the Medical Research Involving Human Subjects Act (16–707/C). Informed consent was obtained for the use of questionnaires for scientific purposes and for the extraction of data from the participating children’s medical records.
Participants
The group of children and adolescents (2–18 years old) with chronic disease included children with CF, children with an autoimmune disease, and children who completed treatment for cancer. The last group was included within 1 year after completing treatment; we refer to these children and adolescents as ‘children postcancer treatment’. The group of participants with an autoimmune disease consisted of children and adolescents with an autoimmune disease, an immunodeficiency or an autoinflammatory condition. We intended to create a cohort with a wide range of somatic diagnoses, both life threatening and non-life threatening, and both congenital and acquired, to cover a wide range of serious paediatric chronic diseases. Participants with an autoimmune disease or with CF were included at least 1 year after initial diagnosis. In the first year after diagnosis, disease activity is generally highest, and the new diagnosis, start of treatment and the disease itself can all cause significant fatigue. By choosing children at least 1 year after diagnosis, we aim to describe the fatigue that persists in a stable phase of the disease. The following exclusion criteria were applied: (1) insufficient understanding of the Dutch language to complete the questionnaires and (2) in case of childhood cancer, relapse of the primary diagnosis.
Study procedures
Patients and their parents were approached via email 3 weeks before their appointment. They were invited to register at home using a web-based tool (www.hetklikt.nu) through which they could complete the questionnaires electronically. If no response was received, they were reminded once via email and once via telephone. A research team was available to answer questions and assist with registration.
Questionnaires
Two validated questionnaires were used to assess fatigue and HRQoL. For children 2–7 years of age, their parents completed the questionnaires, whereas children and adolescents 8–18 years of age completed the questionnaires themselves. Children 8–11 years of age were offered assistance by their parents. In addition, all parents of children 8–18 years of age were asked to fill out the parent-reported version of the two questionnaires as well. If children 8–18 years of age did not want to participate or did not respond, the parent-reported version on the questionnaires was used.
The Dutch version of the Pediatric Quality of Life Inventory (PedsQL) multidimensional fatigue scale (PedsQL MFS) was used to assess fatigue. This questionnaire consists of three subscales (general fatigue, sleep/rest fatigue and cognitive fatigue) with 23 items, yielding a score ranging from 0 to 100 points; lower scores indicate more fatigue. The general fatigue scale contains questions about the subjective feeling of fatigue and about the energy to execute activities, the sleep/rest fatigue scale contains questions about the quantity and quality of sleep and rest and the cognitive fatigue scale contains questions regarding attention and memory. The Dutch version of the PedsQL MFS has good internal consistency.10 To compare our results to both ends of the fatigue spectrum, the data were compared with: (1) a group of children and adolescents from the general population, which served as a relatively non-fatigued group and (2) a group of children and adolescents with CFS, which served as a fatigued control group.10 The CFS control group was recruited from a cohort of children and adolescents with a diagnosis of CFS at the Wilhelmina Children’s Hospital. We used the data from the general population from an existing reference population collected by Gordijn et al that were collected at day care facilities and schools in the Netherlands, between October 2009 and May 2010.10
To quantify the number of severely fatigued children and adolescents, we used a cut-off value of 2 SD below the norm, taking into account sex and age category (2–4, 5–7, 8–11 and 12–18 years old). Children and adolescents who scored >1 SD below the norm were defined as ‘fatigued’. The PedsQL generic core scales 4.0 (PedsQL GCS) was used to assess HRQoL.14 Higher scores indicate higher HRQoL and better functioning. The PedsQL GCS consists of four subscales, with a total score ranging from 0 to 100: physical, emotional, social and school functioning. This instrument has good validity and reliability.14
Clinical assessments
Sex, age, diagnosis, time elapsed between diagnosis and assessment and disease status at assessment were extracted from the medical record of the child or adolescent. For participants with CF, forced expiratory volume in 1 s (FEV1) was used as a proxy for disease status and is expressed as the percentage of predicted FEV1. This predicted percentage is based on the reference values for spirometry of the global lung function 2012 equations by Quanjer et al,15 providing age-matched and sex-matched reference values, with 100% indicating normal lung function. For participants with juvenile idiopathic arthritis (JIA), the clinical Juvenile Arthritis Disease Activity Score and erythrocyte sedimentation rate (ESR) were used as a proxy for disease status; for participants with other autoimmune diseases, only ESR was used.
Data analyses
Descriptive statistics were used to summarise the clinical characteristics of the various groups and the prevalence of severe fatigue (>2 SD below the norm). Differences between participants and non-participants were analysed using the Student’s t-test or the χ2 test. Normally distributed data are presented as mean±SD; otherwise median and IQR were provided. Using linear regression, fatigue scores of children and adolescents with chronic disease were compared with the general population. These differences are described using the mean difference, or unstandardised beta, and 95% CI. Age, sex and reporting method (self-reporting vs parent reporting) have been reported as important determinants of fatigue, including chronic fatigue.16 17 Therefore, these three variables were used as covariates in all analyses.
Different multivariable analyses of covariance (ANCOVA) were used to study the differences in fatigue scores on different fatigue domains between the disease groups, with age, sex and reporter as covariates. Using linear regression, severely fatigued participants with chronic disease were compared with both the general population and to the group with CFS in order to gain further insight into their fatigue profile. Linear regression was used to describe the effect of fatigue on HRQoL. In sensitivity analyses, we excluded the cases in which the parent report was used for children 8 years or older. Differences in which the 95% CI did not include zero were considered statistically significant.
Results
Of the 800 children and adolescents who were eligible for inclusion, 481 (60%) participated and could be assessed for fatigue. Of these 481participants, 440 (91%) also provided informed consent for the use of data from the medical record of the child or adolescent. There was no difference between the participants and non-participants with respect to the distribution of sex, age, disease duration or disease activity, with the exception that non-participants with CF had significantly lower FEV1 values (81.1±16.6) than participants with CF (87.2±18.2). In the group 2–7 years old, 146 parents of completed the questionnaires, in the group 8–12 years old 125 children completed the questionnaires themselves and in the group 13–18 years old 201 adolescents completed the questionnaires themselves. For nine adolescents in the group 13–18 year old, parents completed the questionnaires instead. All participants completed the questionnaires entirely. Common reasons given for not participating were personal circumstances and participating in other research.
Clinical characteristics of the participants are summarised in table 1. The group of children and adolescents with chronic diseases consisted of patients who regularly visited the outpatient clinic. In total, 111 participants (23%) had CF, 277 (58%) had an autoimmune disease and 93 (19%) were postcancer treatment. The group of patients with an autoimmune disease and the CFS control group contained more women than men (with 65% and 75% women, respectively); the other two disease groups and the general population contained approximately equal numbers of men and women. Participants in the CF and autoimmune disease groups were significantly older than participants in the postcancer treatment group and the general population.
Baseline characteristics of the children with a chronic disease and two control groups
Among all children and adolescents with chronic disease, 21.2% scored severely fatigued (defined as >2 SD below the norm) and 37% scored ≥1 SD below the norm (figure 1). Fatigue scores per age group are provided in table 2 for children and adolescents with chronic diseases and the general population. The group of children and adolescents with chronic disease scored more fatigued compared with the general population with respect to total fatigue (mean difference: −3.9 points; 95% CI −5.8 to –2.0), general fatigue (mean difference: −6.6 points; 95% CI −8.9 to 4.3) and sleep/rest fatigue (mean difference: −5.8 points; 95% CI −8.0 to –3.6) but scored similarly for cognitive fatigue (mean difference: 0.9; 95% CI −1.5 to 3.3) (table 3). Within the total group of children and adolescents with chronic disease, both higher age and female sex—but not reporting method—were associated with lower general fatigue scores, with a mean difference of −0.8 points (95% CI −1.2 to –0.4) and −7.0 points (95% CI −11.1 to –3.0) for age and female sex, respectively, and −2.4 points (95% CI −6.8 to 1.9) for reporting method.
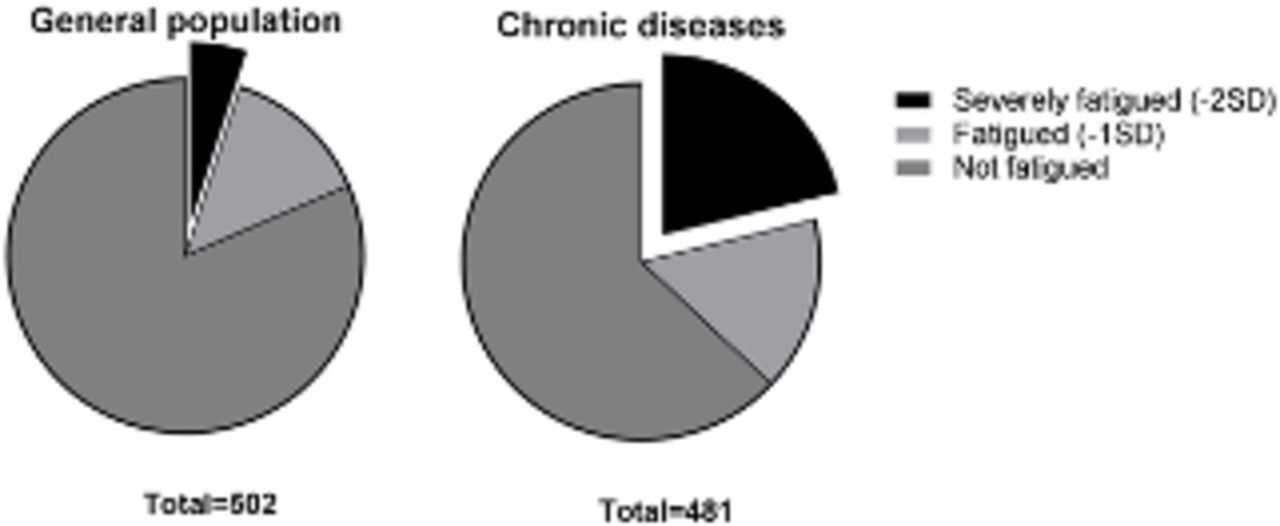
Distribution of severe fatigue in the general population (n=502 children) and in children 2–18 years old with a chronic disease (n=481).
Fatigue scores per age category for children and adolescents with chronic disease (n=481) and the general population (n=502)
Unadjusted and adjusted mean differences in fatigue scores between children with a chronic disease (n=481) and children in the general population (n=502)
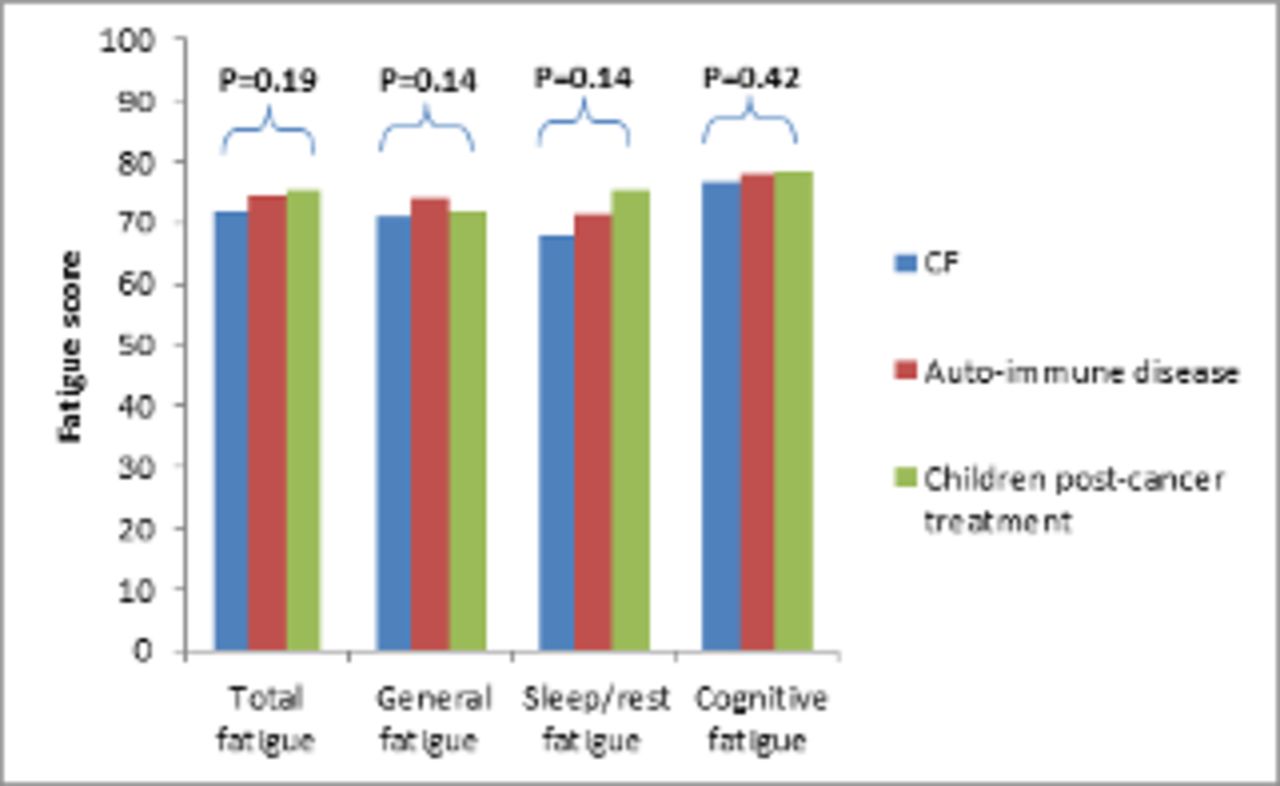
Multivariable ANCOVAs revealed that fatigue scores did not differ significantly between children and adolescents with CF, an autoimmune disease and postcancer treatment with respect to total fatigue (p=0.19), general fatigue (p=0.14), sleep/rest fatigue (p=0.14) or cognitive fatigue (p=0.42) (figure 2 and table 4).
{kind=link}
{kind=link}
Summary of mean fatigue scores for various childhood disease groups, adjusted for age, gender and reporting method (child or proxy). CF, cystic fibrosis.
Mean (±SD) PedsQL MFS scores for indicated disease groups and the general population group
Children and adolescents with chronic disease who were severely fatigued (>2 SD below the norm) scored an average of 29.0 points lower (95% CI −31.6 to –26.4) on the total fatigue score compared with the general population. Specifically, these children and adolescents scored lower for general fatigue (mean difference: −41.2 points; 95% CI −44.0 to –38.4), sleep/rest fatigue (mean difference: −27.4 points; 95% CI −30.6 to –24.2) and cognitive fatigue (mean difference: −18.9 points; 95% CI −22.8 to 15.0) compared with the general population (table 5). Moreover, the fatigue profile for these participants was similar to the participants in the CFS group (table 6).
Unadjusted and adjusted mean differences in fatigue scores between children with a chronic disease who are severely fatigued (defined as >2 SD below the norm; n=102) and the general population (n=502)
Unadjusted and adjusted mean differences in fatigue scores between children with CFS (n=56) and the general population (n=502)
Among children and adolescents with chronic disease, having a lower score on the total fatigue score was associated with a lower total HRQoL score. For each 1-point reduction in the PedsQL MFS score, the same child’s score for HRQoL was on average 0.70 points lower (95% CI −0.65 to 0.75). A similar association was found with respect to physical functioning (mean difference: −0.80; 95% CI −0.68 to –0.92), emotional functioning (mean difference: −0.70; 95% CI −0.62 to –0.78), social functioning (mean difference: −0.56; 95% CI −0.49 to –0.63) and school functioning (mean difference: −0.75; 95% CI −0.68 to –0.82) (table 7). In sensitivity analyses, all results were unaffected by the exclusion of the parent-reported cases in children 8 years or older.
Relationship between total fatigue and HRQoL for children with chronic diseases (n=481)
Discussion
Our results indicate that fatigue is highly prevalent—and therefore highly relevant—among children and adolescents with chronic disease. Fatigue in childhood chronic disease is a common symptom that presents across disease, age, and sex groups and severely affects quality of life. This is the first study to identify and quantify fatigue in a large and representative paediatric sample with various chronic diseases and to compare fatigue in this population with both the general population and patients with CFS. Our results therefore emphasise the need for increased awareness of fatigue—and the need to accurately assess fatigue—in children and adolescents with chronic disease.
Our finding that fatigue is more prevalent among children and adolescents with chronic disease compared with the general population is consistent with previous reports regarding children with JIA and survivors of childhood cancer.9 18 Other studies do not report more fatigue in long-term survivors of childhood cancer.18–20 It may be that the fatigue we found in our study represents the residual consequences of treatment and decreases over time. Also, Armbrust et al 4 did not report more fatigue in children with JIA, which may be due to the younger mean age of the children in their study.4 With respect to CF, fatigue has not been studied previously in children and adolescents. Studies involving adults have shown that fatigue is a prevalent and distressing symptom.8 21 Furthermore, our finding that fatigue has a major impact on HRQoL in children and adolescents with chronic disease is consistent with previous reports.4 22
Fatigue might not necessarily be a disease-specific process.7 23 Several studies reported that fatigue persists despite low disease activity.4 8 9 In addition, we found no significant differences in fatigue scores between disease groups on any fatigue domain. Subsequently, in our study, the pattern of fatigue was similar between severely fatigued children and adolescents with chronic disease and children and adolescents with CFS with no biological explanation for their fatigue, especially concerning cognitive fatigue. Fatigue is likely not simply a biological side effect of the disease and its treatment but also the result of the physical and psychosocial challenges of growing up with a chronic disease.7 23–25 We therefore suggest that interventions should focus on both the somatic and psychosocial aspects of fatigue as, for example, in cognitive–behavioural therapy (CBT).26 CBT has been proven to reduce fatigue in adolescents with CFS and in fatigued adults with various chronic diseases.26–28 Other promising interventions include education, exercise or relaxation or are designed to improve one’s self-efficacy or sleep pattern.4 29 30 Whether children and adolescents with fatigue and a chronic disease respond to CBT and other interventions in the same way as adolescents with CFS is of interest for future studies. Future studies should be designed to determine which biological and psychosocial targets would be suitable for more general fatigue interventions and which interventions are effective for fatigue in younger children, when CBT is not yet a suitable option.
A clear strength of our study is that we examined fatigue across a broad spectrum of chronic diseases, thus increasing the generalisability of fatigue among children and adolescents with chronic disease. Moreover, fatigue was measured in participants 2–18 years of aged, revealing that fatigue is also prevalent in young children; in contrast, most previous studies focused on fatigue in adolescents. If we wish to shift our focus from treating fatigue to also preventing debilitating fatigue, we must expand our focus to include younger children.
Our study had several limitations. First, we combined child-reported data and parent-reported data in our analysis, even though a parent’s reporting of their child can differ from the child’s own reporting.17 We attempted to compensate for this difference by adjusting our analyses for reporting method. We did not find any evidence that reporting method influenced the results. Second, non-participants with CF had lower FEV1 values than participants. Given that lower FEV1 values are associated with fatigue, it is reasonable to speculate that the actual prevalence of severe fatigue among children and adolescents with CF may be even higher than in our study.8 Third, the age and sex distribution in the reference group were not exactly the same as in the chronically diseased group. We compensated for this by adjusting all analyses for sex and age. In this study, we were unable to look at the influence of developmental stage besides chronological age. For future studies, looking at the relationship with developmental stage besides chronological age would be of interest. Female participants were over-represented in the CFS group and in patients with an autoimmune disease; however, this difference reflects clinical practice.4 16 Finally, within the postcancer treatment group, the percentage of participants with a solid tumour was higher than previously reported; this difference might be due to the start of a paediatric oncology centre in the Netherlands, which centralisation of care started with children and adolescents with solid tumours.31
With a symptom as prevalent as fatigue, the ability to implement a relatively simple, validated screening questionnaire such as the PedsQL MFS may be clinically valuable in an outpatient setting.32 Monitoring fatigue can improve patient-centred care and will help shift the clinician’s focus to the individual child’s needs.
Conclusions
Fatigue is highly prevalent—and therefore highly relevant—among children and adolescents with chronic disease. Fatigue in childhood chronic disease is a common symptom that presents across disease, age and sex groups and severely affects quality of life. Our findings underscore the need for systematically assessing fatigue in children and adolescents with chronic disease. Future studies should determine possible biological and psychosocial treatment targets.
Acknowledgments
The authors would like to acknowledge the contribution of the patients and parents who participated in this study and the involved caregivers who included patients and discussed the outcomes of the questionnaires with them. The authors would also like to thank Dr C F Barrett for his
assistance with English language editing.
References
Footnotes
Contributors MMN-vdV collected and analysed the data and drafted the paper. SN designed the study and coordinated and supervised data collection and reviewed the manuscript. EMvdP, MAG, KvdE and GWD designed and supervised the data collection and interpretation and reviewed the manuscript. MMvdH-E, NW, JFS and RRLvL critically reviewed the data analyses and reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available on reasonable request.
Patient consent for publication Not required.