Article Text

Abstract
Aims To assess the impact of different oxygenation policies on the rate and severity of retinopathy of prematurity (ROP).
Methods Between January 2003 and December 2006, infants of 1500 g birthweight (BW) or less and/or 32 weeks gestational age (GA) or less, and larger, more mature infants with risk factors for ROP were examined through three different time periods: period 1: high target oxygen saturation levels (88–96%) and treatment at threshold ROP; period 2: low target oxygen saturation levels (83–93%) and treatment at threshold ROP; period 3: low target oxygen saturation and treatment at type 1 ROP.
Results Type 1 ROP was detected more frequently in babies of 32 weeks GA or less (50/365, 13.7%) than in more mature babies (15/1167, 1.3%; p<0.001). The rate of type 1 ROP in period 1 was 6.9%; period 2, 3.6% and period 3, 1.8%. Rates of stage 3 ROP declined over time in both BW/GA groups (from 9.0% to 4.1% to 2.0%) as did rates of plus disease (from 7.5% to 3.6% to 1.8%). Mean BW and GA declined from period 1 to period 3, and death rates remained unchanged. 74.4% of babies received all the examinations required; 48.1% of treatments were undertaken after discharge from the neonatal unit.
Conclusions Lower target oxygen saturation was associated with a lower rate of severe ROP without increasing mortality, and changed the characteristics of affected babies. Screening criteria need to remain wide enough to identify all babies at risk of ROP needing treatment.
- Child health (paediatrics)
- Public health
- Retina
Statistics from Altmetric.com
Introduction
Retinopathy of prematurity (ROP) is a largely preventable cause of blindness. In highly developed countries the population of premature infants at risk has changed over time and the majority needing treatment now weigh less than 1000 g at birth.1 In light of this, most screening programmes in high-income countries include only infants with birthweights (BW) of less than 1500 g and gestational age (GA) of less than 32 weeks.2–4 More mature infants are only examined when considered necessary by the neonatologist. However, Gilbert et al1 have shown that these criteria do not apply in countries with low and moderate levels of development, where ROP is emerging as a major cause of childhood blindness and where wider criteria are needed. In Argentina ROP is the commonest cause of blindness in children due to high birth rates and rates of premature births, lack of resources and trained personnel in neonatal care and insufficient screening programmes.1 ,5 ,6
New national policies for oxygen administration were introduced in our level 3, government sector neonatal unit in Córdoba, in August 2004, in line with guidelines developed by the Ministry of Health and professional organisations.7 This entailed training staff on the new target saturation levels, and providing additional equipment for oxygen monitoring so that all preterm babies receiving supplemental oxygen could be monitored adequately, which was not previously always possible. The purpose of this study was to determine the rate and severity of ROP among premature infants admitted to the unit and to assess the impact, if any, on rates of ROP needing treatment and the population at risk, before and after the new policies on oxygen administration were introduced.
Materials and methods
The study took place in a level three neonatal intensive care unit (NICU) in a government hospital, which has an average of 6500 births a year, in Córdoba, Argentina, between January 2003 and December 2006. The NICU is a referral unit for high-risk infants and receives sick preterm and full-term babies from the Province of Córdoba and neighbouring provinces. The following babies were examined in the ROP programme: those with BW of 1500 g or less and GA of 32 weeks or less (according to UK criteria),8 as well as larger, more mature infants who had an unstable clinical course or who were exposed to known risk factors for ROP. Only babies born in the hospital or those referred from another hospital within 24 h of birth were included in the analysis.
All infants were examined with a binocular indirect ophthalmoscope and a +20D lens by two ophthalmologists experienced in ROP screening (JAUZ, EGK). The first examination was performed 3–6 weeks after birth and examinations continued every 1–2 weeks until the retina was fully vascularised or there was spontaneous involution of ROP, or treatment was indicated. ROP stages and severity were classified according to guidelines from the international classifications of ROP.9 ,10 Internationally recognised guidelines for the timing and frequency of eye examinations were followed, and findings were documented on the stage and zone of any ROP as well as the presence of plus disease in each eye at each examination. In line with the majority of other studies of ROP, we analysed data on rates of ROP needing treatment as well as by the maximum stage of ROP in the most affected eye, and whether plus disease developed at any time.
Indications for treatment changed over the course of the study period as a result of the findings of the early treatment trial of ROP:11 between January 2003 and July 2005 treatment was indicated at threshold disease, while between August 2005 and December 2006 treatment was indicated when type 1 ROP was detected. There were also two different periods concerning oxygen administration. The first period included those infants examined from January 2003 to July 2004 in whom the upper target oxygen saturation levels were 88–96%. The second period included infants examined between August 2004 and December 2006, when targets were 83–93%. Mortality rates, defined as the number of deaths during the first month of life per 1000 live births, were calculated for each period.
In this study there were, therefore, three distinct periods: period 1, when higher saturation targets were used and babies were treated at threshold; period 2, lower saturation targets were used and babies were still treated at threshold; and period 3, lower saturation targets continued to be used and babies were treated when they developed type 1 ROP. For each study period data are presented using the same definition of ROP, ie, type 1 ROP, defined as any stage with plus disease in zone 1; stage 3, without plus disease in zone 1; stage 2 or 3, with plus disease in zone 2.11 No other new policies or practices were introduced over the study period and staffing levels remained constant.
Informed consent was obtained from parents of all infants in the study, which was approved by the institutional review board of the Materno-Neonatal ‘Ramon Carrillo’ Hospital, and conducted in accordance with the tenets of the Declaration of Helsinki.
Statistical analysis was performed by means of the Student's t test. Statistical significance was considered with p<0.05. Logistic regression was performed for categorised data.
Results
A total of 1532 infants was examined at least once; 392 (25.6%) infants did not receive all the eye examinations required (table 1): 176 (11.5%) were lost after discharge from the NICU and 216 (14.1%) only attended some examinations as outpatients. Overall, there was no statistically significant difference in completeness of examination rates across the three time periods (χ2=0.51; 2 d.f.; p=0.78). However, smaller, less mature babies were significantly more likely to default than more mature babies (34.5% vs 22.8%; p<0.001) in all three time periods (table 1).
Number of babies completing and not completing examinations, by screening criteria and study period
Any stage of ROP was detected in 344 infants (22.5%), being more frequent among smaller babies who fulfilled UK criteria (214/365, 58.6%) than those who fell outside UK criteria (130/1167, 11.1%; p<0.001). Type 1 ROP was detected in 65/1532 (4.2%) infants overall, occurring more frequently in smaller babies (50/365, 13.7%) than in more mature babies (15/1167, 1.3%; p<0.001; table 2). In period 1, 6.9% of babies developed type 1 ROP, which declined to 3.6% in period 2 and 1.8% in period 3, representing a 75% reduction between periods 1 and 3. Only 0.6% (5/757) of bigger babies developed type 1 ROP during periods 2 and 3 compared with 2.4% (10/410; p=0.02) in period 1 when higher oxygen saturations were being used. The equivalent data for smaller babies was 10% (20/198) compared with 18% 30/167; p=0.04).
Proportion of babies developing severe ROP and the proportion treated (%), by study period
The data were also analysed by the maximum stage of ROP reached in the most affected eye, and whether plus disease developed or not (figure 1). These data confirm that the severity of ROP declined in both BW/GA groups over the three time periods.

Rates of stage 3 retinopathy of prematurity (ROP), and rates of plus disease (aggressive posterior ROP included in these cases), by birthweight (BW)/gestational age (GA) group in the different time periods. ‘Smaller’ groups included babies who fulfilled UK criteria (BW 1500 g or less and GA of 32 weeks or less), and ‘bigger’ groups, those that fell outside UK criteria (BW over 1500 g and GA of more than 32 weeks).
Fifty-four of the 65 babies developing type 1 ROP were treated. The 11 babies not treated were examined in periods 1 and 2 when threshold disease was the indication for treatment. Almost half of all treatments were undertaken after the baby had been discharged (26/54, 48.1%; table 3). Bigger babies were more likely to be treated after discharge than smaller babies (83.3% vs 38.1%; p=0.01). Six (11%) smaller babies had an unfavourable outcome.
Number of babies treated and where they were treated, by screening criteria
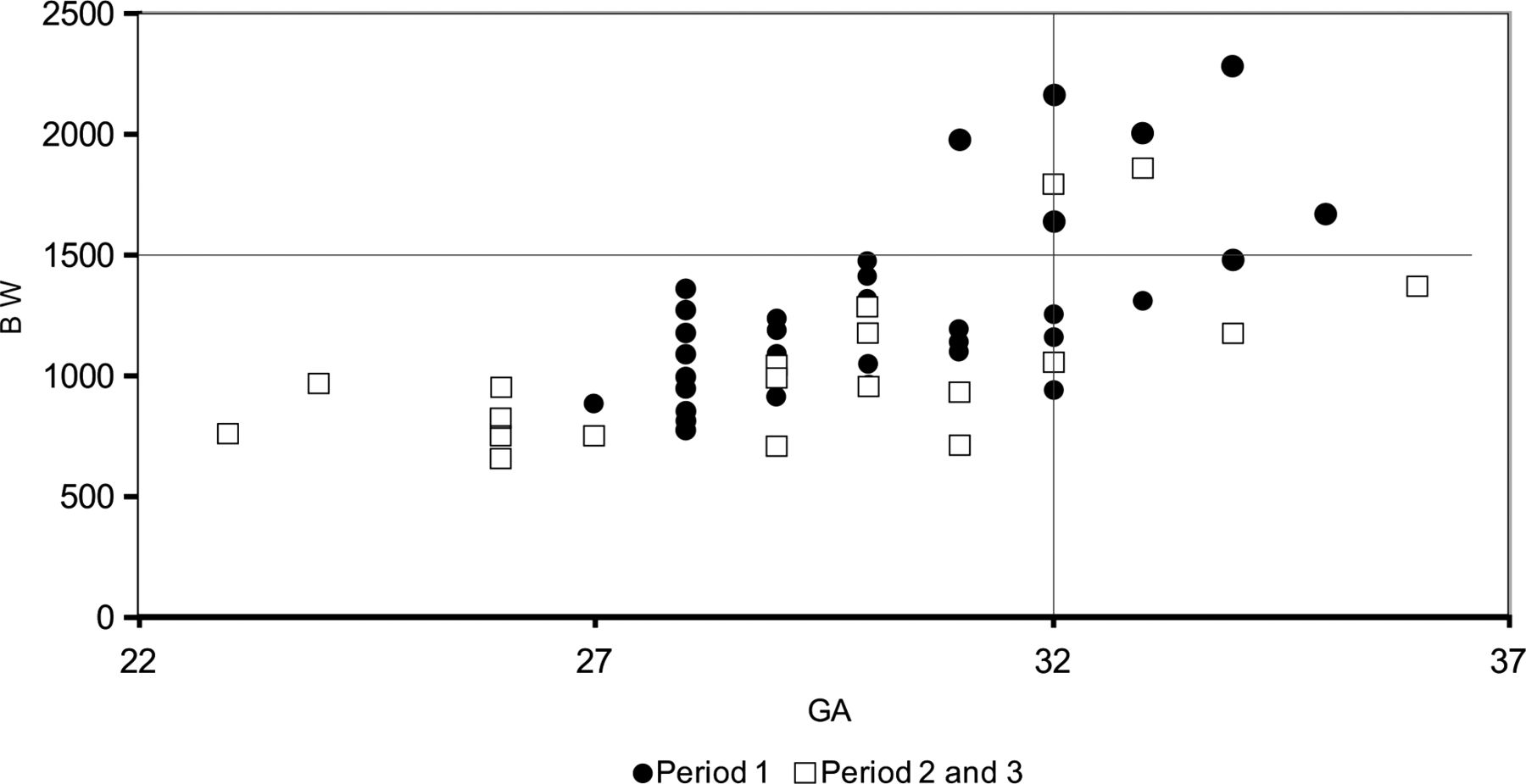
The mean BW of the 65 babies developing type 1 ROP declined from 1250 g in period 1 to just over 1000 g in periods 2 and 3 (table 4; figure 2). The mean GA also declined from over 30 weeks in period 1 to less than 30 weeks in periods 2 and 3.
Mean birthweight and gestational age of babies developing severe ROP, by study period

{kind=link}
{kind=link}
Birthweight (BW) and gestational age (GA) of treated infants. The horizontal and vertical lines indicate the upper limits of the developed countries’ screening criteria.
The mortality rate in period 1 was 130.3/1000 live births and 134.1/1000 for periods 2 and 3. In both time periods most deaths were not related to syndromes or congenital abnormalities, the latter being responsible for 46/1000 deaths in the first period and 72/1000 deaths in periods 2 and 3.
The case mix of babies examined in the three time periods did not differ substantially. Mean BW were 1752±569 g in period 1; 1782±576 g in period 2 and 1878±627 g in period 3. Mean GW were 33.0±2.3 weeks in period 1, 33.3±2.4 weeks in period 2 and 33.5±2.5 weeks in period 3. However, there were differences in characteristics between babies examined and not examined in the three study periods. In periods 1 and 3, babies not examined were significantly less mature than those completing all examinations (table 5).
Characteristics of babies who did and who did not complete all eye examinations, by study period
Discussion
The question of what constitutes optimal oxygen saturations in the first few weeks of life following preterm birth in terms of morbidity (including ROP) and mortality is receiving renewed attention. Indeed, there are suggestions that target saturations may need to vary, depending on GA/postconceptional age, but as yet there is only limited evidence in support of this. Several multicentre randomised clinical trials have or are being undertaken,12 ,13 and the results of other trials are awaited. However, translating the findings of well-conducted, rigorously monitored clinical trials into the real world of clinical care can be challenging. For example, maintaining oxygen saturations within levels recommended by policy can be difficult.14 Several observational studies have reported the beneficial effects of lower target oxygen saturation levels on the incidence and severity of ROP,15–18 but there is a lack of information from regions where the incidence of ROP and ROP blindness are still high, especially among larger, more mature premature infants.
The main findings of our study are that there was a significant reduction in both the rate of type 1 ROP and of stage 3 and of plus disease over the 4 years of the study and a decline in the mean BW and GA of affected babies. We decided not to combine data from 2004/5 with that from 2005/6 as the indications for treatment changed in August 2005. We know from the ET–ROP trial that the constellation of signs described in type 1 ROP have a 15% risk of progression to stage 4 or 5 compared with the constellation of signs that make up threshold disease, which has a 50% risk of progression. This means that the change in rates of ROP from period 2 to period 3 in our study (ie, from 3.6% treated at threshold in period 2, to 1.8% treated at type 1 ROP) represents a very dramatic decline in the severity of ROP between the two study periods. This is supported by the decline in rates of stage 3 ROP and of plus disease.
It is tempting to attribute the changes in the unit in Córdoba to the implementation of the policy of lower target oxygen saturation levels. However, without data on the practices and behaviours of nurses and doctors, and data on oxygen saturation levels among babies for the different time periods, it is not possible to attribute the change in ROP prevalence to implementation of the policy. Indeed, rates of ROP continued to decline in period 3 compared with period 2, suggesting that other factors were also playing a role. For example, staffing practices may have improved over the period of the study leading to better control of temperature or sepsis but no new policies or interventions were introduced. A potential confounding factor is that the case mix of babies examined may have changed over time, but the mean BW and GA of babies examined in each of the three time periods did not alter significantly. Indeed, a reduction in rates of ROP needing treatment has been reported in other studies when no specific interventions had been implemented, and it has been suggested that the frequent presence of an ophthalmologist in the unit helps to maintain awareness among staff of the need to monitor oxygen carefully. Another limitation is that exposure to other risk factors for ROP may have changed over time, such as early and late sepsis rates, surgery for patent ductus arteriosus, but these data were not available, unfortunately. Assessing ethnicity in Latin America is challenging, as a high proportion of the population are of mixed ethnicity and many preterm babies are delivered to unmarried teenagers. However, there were no other policy changes during the study period in relation to any intervention, such as erythropoietin administration, and no major changes to neonatal care.
The finding that even in period 3 bigger, more mature babies were still developing type 1 ROP than is currently the case in industrialised countries suggests that more could be done to improve exposure to modifiable risk factors for ROP.2 ,19 In a recent study, 13% of 1091 infants with severe ROP from 11 countries had BW and GA exceeding those recommended for screening in the UK.1 ,9 Similar findings have been reported from Iran,19 south India,20 Saudi Arabia,21 Vietnam,22 China23 and an earlier study from Argentina.24
Lower target oxygen saturations in periods 2 and 3 in our study did not result in a higher death rate than in period 1. This is in contrast to the SUPPORT study, a multicentre randomised trial that compared outcomes among 1316 preterm infants who were randomly assigned to oxygen saturations of either 85–89% or 91–95% within 2 h of birth.13 These targets were maintained up to 36 weeks postmenstrual age or until the infant was breathing room air without ventilation for more than 72 h.13 While severe ROP was less frequent among survivors in the lower saturation group (8.6% vs 17.9%), death before discharge was more frequent (19.9% vs 16.2%).13 However, babies in the SUPPORT study were considerably more premature than infants in our study (mean GA 26±1 weeks vs 33±2.5 weeks, respectively). Longer follow-up is required to establish the effects of lower oxygen saturation levels on neurodevelopment and other outcomes.
In our study over a quarter of all eligible infants did not undergo all the examinations required and almost half of all babies needing treatment were treated after discharge from the unit. Some babies who defaulted may also have developed ROP needing treatment. The variation in characteristics of babies examined and not examined in the three study periods may have biased the findings, as rates of ROP needing treatment may have been underestimated in periods 1 and 3. This would have had the effect of underestimating the difference in rates of ROP needing treatment between periods 1 and 2 and overestimating the difference between periods 2 and 3. To our knowledge, only two other studies have reported on the completeness of eye examinations in an ROP programme.25 ,26 In one study of two units in Houston, USA, almost 50% of infants with or at risk of ROP were not scheduled for a timely outpatient follow-up appointment, especially when appointments were not scheduled by hospital personnel before discharge.25 In the other study (from seven units in Brazil), 23% of eligible babies were either not referred to the ophthalmologist in the first place (10%), or failed to complete examinations after discharge (13%).26 In our unit, appointments for follow-up after discharge are arranged by hospital staff, principally the neonatologist in charge. Reasons for the high attrition need to be explored and interventions developed to ensure that all babies at risk are adequately examined, particularly after they have been discharged. This is important in settings where more mature babies are developing ROP needing treatment, as they are more likely to develop a disease needing treatment after discharge.
In conclusion, lower target oxygen saturation was associated with a lower rate of severe ROP and a change in the characteristics of affected babies without increasing death rates. Accounting for all important aspects of care is an acknowledged limitation of observational studies compared with the protocol-driven, controlled methodology of randomised clinical trials. However, observational studies and clinical trials both have their place in building up the evidence base, which informs clinical guidelines and policy, as they address different questions; clinical trials answer the question of efficacy, whereas observational studies address the question of effectiveness under non-trial settings. Further operational research is needed to assess how other interventions for the prevention of ROP, over and above using target oxygen saturations, can best be implemented within the resource constraints of neonatal care in middle-income countries. As long as more mature babies develop ROP needing treatment in our unit we will continue to maintain wider screening criteria than are currently being used in industrialised countries.
References
Footnotes
-
Contributors JAUZ: conception and design of the work, ophthalmological examination of patients and follow-up, treatment of patients, analysis and interpretation of data, writing of the manuscript and text editing. NC: acquisition, analysis and interpretation of data, statistical analysis, manuscript revision. EGK: ophthalmological examination of patients and follow-up, treatment of patients, design of the work, acquisition, analysis and interpretation of data, manuscript revision and correction. FAE: acquisition, analysis and interpretation of data, manuscript revision. EC: Supervision of patients’ care, implementation and supervision of oxygen saturation policies in the NICU and delivery room, acquisition and analysis of data. MEUZ: analysis and interpretation of data, manuscript revision and text editing. GST: clinical care of patients and follow-up, implementation and supervision of oxygen saturation policies in the NICU, acquisition and analysis of data. JIT: acquisition, analysis and interpretation of data. HMS: analysis and interpretation of data, manuscript critical revision and correction. CG: analysis and interpretation of data, manuscript critical revision and correction. HMS and CG contributed equally to this work. All authors read and approved the final manuscript.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board of the Materno-Neonatal ‘Ramon Carrillo’ Hospital, Córdoba, Argentina.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.