Article Text

Abstract
Objective Indomethacin prophylaxis (IP) reduces the risk of intraventricular haemorrhage (IVH) and patent ductus arteriosus (PDA) in preterm infants. However, the optimal time to administer IP has not been determined. We hypothesised that IP at ≤6 h is associated with a lower incidence of IVH or death than if administered at >6–24 h of age.
Methods We performed a retrospective cohort study of extremely low birth weight infants (≤1000 g birth weight) treated in the neonatal intensive care units in the Neonatal Research Network from 2003 to 2010 and who received IP in the first 24 h of age. Infants were dichotomised based upon receipt of IP at ≤6 or >6–24 h of age. The primary outcomes were IVH alone and IVH or death. Secondary outcomes were PDA alone and PDA or death. We used multivariable analyses to determine associations between the age of IP and the study outcomes expressed as an OR and 95% CI.
Results IP was given at ≤6 h to 2340 infants and at >6–24 h to 1915 infants. Infants given IP at ≤6 h had more antenatal steroid exposure, more inborn and less cardiopulmonary resuscitation (p<0.01). After multivariable analyses, age of IP receipt was not associated with IVH, and IVH or death but PDA receiving treatment/ligation or death was lower among IP at ≤6 h compared with IP at >6–24 h (OR 0.83, 95% CI 0.71 to 0.98).
Conclusions IP at ≤6 h of age is not associated with less IVH or death, but is associated with less PDA receiving treatment/ligation or death.
- Neonatology
- Intraventricular Hemorrhage
- Patent Ductus Arteriosus
- Extreme prematurity
Statistics from Altmetric.com
What is already known on this topic
Prophylactic indomethacin reduces the incidence of intraventricular haemorrhage (IVH) in preterm infants.
Indomethacin prophylaxis for IVH also reduces the risk for patent ductus arteriosus (PDA).
In clinical practice, prophylactic indomethacin timing can be variable.
What this study adds
Timing of indomethacin prophylaxis does not affect the incidence of IVH or death.
Indomethacin prophylaxis at ≤6 h of age is associated with lower incidence of PDA receiving medical or surgical treatment or death.
Introduction
Intraventricular haemorrhage (IVH) is a major cause of poor neurodevelopmental outcome among extremely premature infants.1 ,2 More than 50% of all IVH in very low birth weight (VLBW) infants occurs in the first 6–8 h of age.3 Indomethacin prophylaxis (IP) reduces the risk of IVH and patent ductus arteriosus (PDA) in preterm infants.4–6 Two time points have been used for IP in different randomised controlled trials, that is, between 6 and 12 h of age in the trial by Ment et al5 and <6 h of age in the trial by Schmidt et al.6 However, the initial dose of indomethacin may be administered over a wide time interval in clinical practice. To the best of our knowledge, the optimal time for IP has not been established.
In the Neonatal Research Network (NRN) database, a large proportion (46%) of VLBW infants (2003–2007) developed a PDA; 71% of these infants received medical treatment and 27% of them received surgical ligation.7 The effect of IP timing upon the incidence of symptomatic PDA receiving medical or surgical treatment has not been examined.
Since the risk for IVH is reported to be highest in the initial hours following the birth, we hypothesised that administering IP within 6 h of age is associated with a lower incidence of IVH or death among extremely low birth weight (ELBW) infants compared with administration after 6 h of age. We also evaluated the effects of IP administered at ≤6 h compared with after 6 h of age on the incidence of PDA receiving treatment (medical or surgical) or death in ELBW infants.
Patients and methods
This retrospective cohort study included infants with birth weights ≤1000 g who received IP up to 24 h of age and were admitted to the 18 participating neonatal intensive care units (NICUs) in the Eunice Kennedy Shriver National Institute of Child Health and Human Development NRN. The NRN is a consortium of academic tertiary care NICUs in the USA with a research focus on neonatal care, particularly ELBW infants. Exclusion criteria included death within 12 h after birth, unknown time of indomethacin administration, genetic syndromes, congenital anomalies or an unavailable head ultrasound report. We dichotomised the study cohort into groups based upon the timing of the first dose of prophylactic indomethacin, that is, indomethacin administration ≤6 h of age or >6–24 h of age.
Data items collected were part of the Generic Data Base (GDB), which is an ongoing survey of neonatal morbidity and mortality. Trained research nurses abstracted data from medical records guided by the predefined criteria in a manual of operation and electronically transmitted the data to the NRN data centre (RTI International, North Carolina, USA). Data from each centre were reviewed monthly with a series of edits by the data centre to ensure reliability. Data were retrieved from the GDB for calendar years 2003–2010 from all participating centres in the NRN that included maternal characteristics and problems of pregnancy, neonatal demographics, delivery room events and morbidities during the course of hospitalisation.
The primary outcomes were IVH (all grades), IVH or death, severe IVH (grades 3 and 4) and severe IVH or death. Secondary outcomes were PDA, PDA or death, PDA receiving medical or surgical treatment, and PDA receiving medical or surgical treatment or death. The diagnosis of IVH was based upon head ultrasound results. Ultrasound findings were used to establish the severity of IVH as described by Papile et al.8 The NRN database contains the results of the worst head ultrasound within the first 28 days of age. The diagnosis of PDA was based upon the echocardiography requested for clinical indications: universal echocardiographic screening for PDA was not performed. A decision for treatment of a PDA (medical or ligation) was also based upon the clinical assessment of the providers in each centre.
Maternal and neonatal variables were compared between groups using Student's t tests for continuous variables and χ2 comparisons for categorical variables. Unadjusted ORs were calculated for IVH, IVH or death, severe IVH and severe IVH or death. Unadjusted risk for the primary outcome by indomethacin timing was also assessed by gender and gestation. Multivariable analyses were performed to adjust for the following covariates: network centre, gestational age, maternal hypertension, maternal antibiotics, any antenatal steroids (either one or two doses), caesarean section, race, male sex, small for gestational age (SGA), chest compressions in delivery room, outborn, PDA and admission temperature. Results of multivariable analyses are reported as OR and 95% CIs.9 ,10 Adjusted ORs were assessed for interactions by sex or gestation for IVH, IVH or death, severe IVH and severe IVH or death.
The incidence of PDA and PDA receiving medical treatment or ligation was determined in both groups (indomethacin at ≤6 h and >6–24 h). Multivariable analyses were performed using the same covariates as the analyses for IVH.
The analyses listed above for IVH and PDA indicated a higher proportion of outborn infants in the group receiving IP >6–24 h compared with those in the ≤6 h group (15% vs 3%). Due to the unmeasured variables that may be associated with outborn status, a second set of multivariable analysis was performed for the outcomes of IVH, IVH or death, PDA and PDA or death among inborn infants only.
Results
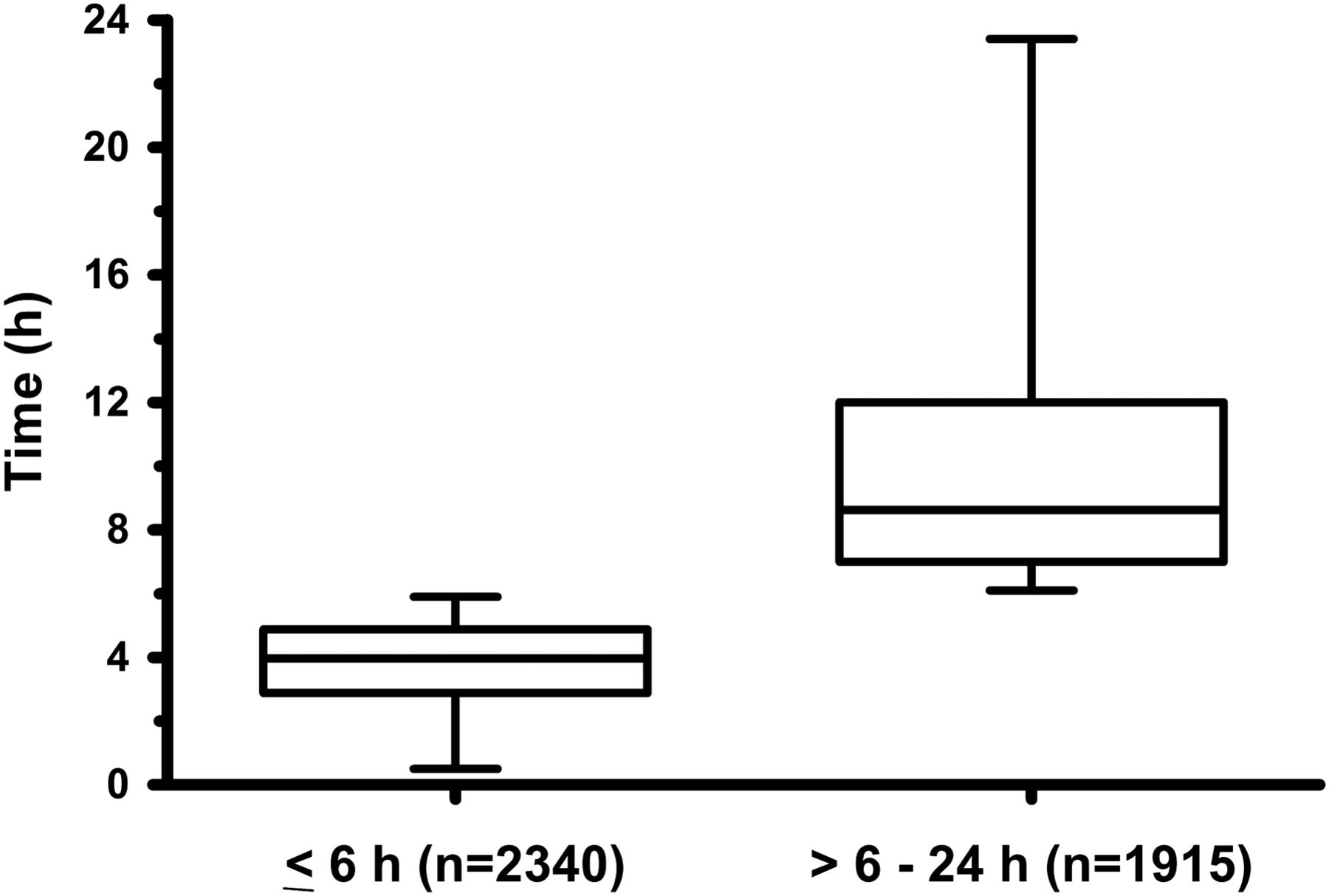
During the study period (2003–2010), 13 754 infants with a birth weight ≤1000 g were admitted to the participating centres in the NRN. IP was not given to 9172 infants. The latter included infants who died prior to 12 h of age or had missing information regarding IP. Of 4582 infants who received IP, 327 infants were excluded due to congenital syndromes or anomalies (n=100), missing head ultrasound reports (n=6), unknown time of IP (n=187) or the administration of indomethacin after 24 h of age (n=34). This left 4255 infants available for analysis. The first prophylactic dose of indomethacin was given at ≤6 h of age in 2340 infants and at >6–24 h of age in 1915 infants. The median time for the administration of the first prophylactic dose of indomethacin was 3.9 h (IQR 2.8–4.8 h) for infants treated at ≤6 h and 8.7 h (IQR 7–12 h) for those treated between >6 and 24 h of age (figure 1).

{kind=link}
Median time for actual administration of indomethacin prophylaxis in the two groups at ≤6 h or >6–24 h.
Maternal characteristics and delivery room events are summarised in table 1. Mothers of infants given IP at ≤6 h of age had more hypertension, receipt of antibiotics and antenatal steroids (p<0.001). The incidence of chorioamnionitis was higher in the group receiving indomethacin >6–24 h of age. Neonatal characteristics of the cohort are described in table 2. Infants receiving IP at ≤6 h of age had less chest compressions in the delivery room (p<0.001). Upon admission to the NICU, infants receiving IP at ≤6 h of age had higher admission temperatures and a lower percentage of outborns (p<0.0001).
Maternal characteristics and delivery room events
Neonatal characteristics of study cohort
Bivariate analyses indicated lower incidences of IVH or death and severe IVH or death in the group receiving IP at ≤6 h of age compared with IP at >6–24 h of age. The incidence of PDA or death, PDA receiving medical or surgical treatment or death was also lower when indomethacin was administered at ≤6 h of age (table 3).
Indomethacin timing and unadjusted risk for intraventricular haemorrhage (IVH) and patent ductus arteriosus (PDA)
However, there was no significant difference in the incidence of any IVH-related outcomes after adjustment using multivariable analyses (table 4).
Effect of indomethacin prophylaxis timing (≤6 h of age) on intraventricular haemorrhage (IVH) or death
After adjusting for covariates, the odds of infants with a PDA receiving medical or surgical treatment were lower among infants receiving IP at ≤6 h compared with later administration (OR 0.81, 95% CI 0.67 to 0.98). Similar ORs were found when PDA outcomes were combined with death (table 5).
Effect of indomethacin prophylaxis timing (≤6 h of age) on patent ductus arteriosus (PDA) or death
When analyses were limited to inborn infants, there was a total of 3904 infants; 2267 received IP at ≤6 h and 1637 infants received IP at > 6–24 h. Bivariate comparisons between these two groups showed differences in the same variables as the combined inborn and outborn cohort in tables 1 and 2, except that there were no differences in any or complete antenatal steroids. Multivariable analyses indicated that there were no associations between the time of IP and any of the IVH-related outcomes. Similar to the combined inborn and outborn cohort, IP at ≤6 h among only inborn infants was associated with a lower incidence of PDA receiving medical treatment or ligation (OR 0.79, 95% CI 0.65 to 0.96) and PDA receiving medical treatment/ligation and/or death (OR 0.81, 95% CI 0.69 to 0.97).
A secondary analysis was performed to examine potential interactions between time of IP and sex or gestation for outcomes involving IVH. Results of bivariate analysis by sex and gestation are summarised in the online supplementary appendix . No interactions were identified between gestation or sex and the time of IP administration for any outcome involving IVH after adjustment for covariates on multivariable analyses.
There were no differences in the incidences of necrotising enterocolitis (12% vs 13%, p=0.29), spontaneous intestinal perforation (SIP) (6% vs 5%, p=0.25), retinopathy of prematurity receiving treatment (11% vs 12%, p=0.2) and bronchopulmonary dysplasia (38% vs 36%, p=0.58) between the two groups.
Discussion
We previously reported no effect of early IP on the incidence of IVH among premature infants with a birth weight ≤1250 g; however, severe IVH among extremely premature (<27 weeks) female infants was lower when IP was administered at ≤6 h. This was an important but unexpected finding, and we questioned whether the finding reflected chance due to the small sample size.11 Data available from the National Institutes of Child Health and Human Development (NICHD) NRN Generic Database provided the opportunity to examine the time of administration of indomethacin in a larger cohort derived from multiple centres. We confirmed that IP before 6 h of age does not decrease the incidence of IVH or death compared with later administration up to 24 h of age. Similar findings were reported by Yanowitz et al.12 In this larger cohort, we did not find an interaction by sex or gestation and the incidences of any IVH-related outcomes in association with the timing of IP.
The increased risks of IVH are associated with haemodynamic instability and changes in cerebral blood flow.13 ,14 These haemodynamic changes are more likely to occur with increased frequency during the early hours after delivery. Since indomethacin could attenuate the development of fluctuations in cerebral blood flow in the early hours after birth,15–17 we hypothesised that IP at ≤6 h would decrease the incidence of IVH. The results of the current study did not support our hypothesis.
We acknowledge that the gap in the median time of drug administration (3.9 vs 8.7 h) between the two groups was not large. However, it is unlikely that a wider gap exists with regard to IP timing as the practice is largely based upon two RCTs, in which indomethacin was administered either ≤6 h6 or between 6 and 12 h of age.5 Alternatively, advances in both obstetrical and neonatal practices may have changed the timing of highest risk for IVH. Thus, the benefit of IP in reducing IVH may extend to the time intervals beyond the initial few hours after the delivery.
We considered analysing the time of indomethacin administration as a continuous variable for the entire cohort. However, IP timing data were not normally distributed. Over the 24 h study period, there were multiple time points at which very few infants (<2% of the cohort) received IP. Due to the uneven distribution of data along the 24 h timeline, treating the time of indomethacin administration as a continuous variable was not felt to be more informative.
Indomethacin treatment within the first 48 h is associated with higher rates of PDA closure compared with indomethacin treatment after 48 h.18 However, differences in the rate of PDA closure have not been previously examined with reference to the timing of IP. Our adjusted results indicate a significant association between early IP (≤6 h of age) and a lower incidence of PDA receiving medical treatment or surgical ligation or death compared with administration at >6–24 h of age. These observations may reflect the decreased response of the ductus arteriosus to indomethacin with increasing postnatal age.19 This phenomenon has been attributed to increased endogenous production of nitric oxide in the ductal endothelium after the first 24 h of age19 and to the production of inflammatory cytokines, which can contribute to ductal vasodilatation.20
Since indomethacin can affect other organ systems,21 ,22 we compared the incidences of potential untoward effects of IP ≤6 h compared with > 6–24 h of age. There was no difference between the two groups in the incidences of necrotising enterocolitis, SIP, retinopathy of prematurity requiring intervention and bronchopulmonary dysplasia.
The strengths of this study include a large patient cohort from multiple centres. We have used data from NICHD NRN, which has predefined morbidities and have been abstracted by trained research personnel. There are several limitations to our study. This was a retrospective study of a non-randomised cohort and is subject to bias by unmeasured confounders. The infants in the early prophylaxis group appeared less sick compared with the infants in the group that was treated later, that is, less chest compressions and less exposure to antenatal steroids. Nonetheless, we have adjusted the results for differences in confounding variables. Although adjustment for illness scores would have been of interest to separate critically sick infants, the GDB does not capture an illness severity score.
Conclusion
We conclude that administration of prophylactic indomethacin at ≤6 h of age was not associated with a lower incidence of IVH or death in ELBW infants. However, medical treatment or surgical ligation of PDA or death was significantly less frequent among the infants who received IP ≤6 h of age compared with later administration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online appendix
Footnotes
Contributors HM, ARL, WO, BRV, BJS, SK, BSS and the members of Generic Database Subcommittee of the NICHD Neonatal Research Network fulfil the contribution criteria to the paper according to the ICMJE guidelines. Each one of the above-mentioned authors had substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work or revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Research reported in this publication was supported by the National Institutes of Child Health and Human Development (NICHD) via a multicentre Neonatal Research Network grant number 5U10HD027904-24.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NICHD Neonatal Research Network.
Competing interests None declared.
Ethics approval Each participating NRN site had Institutional Review Board approval for data collection for the NRN Generic Data Base (GDB)..
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This study was conducted in collaboration with The National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). NIH provides grant support for the Neonatal Research Network's Generic Database, which is available to all researchers in the participating centres. Multiple studies are published based on these common data. However, data analysis presented in our study was never published before.
Linked Articles
- Fantoms