Article Text

Abstract
Objective Providing skin-to-skin care (SSC) to preterm infants is standard practice in many neonatal intensive care units. There are conflicting reports on the stability of oxygen saturation (SpO2) during SSC, which may create a barrier to a wider implementation of SSC to infants receiving respiratory support. Regional cerebral oxygenation (rcO2) measured using near-infrared spectroscopy can serve as a surrogate parameter for cerebral oxygen delivery and consumption. We hypothesised that rcO2 during SSC would be similar to standard care in preterm infants receiving respiratory support.
Design Prospective observational non-inferiority study.
Setting Single tertiary perinatal centre in Australia.
Patients Forty preterm infants (median (IQR) of 27.6 (26.0–28.9) weeks' gestation) receiving respiratory support were studied on day 8 (5–18).
Interventions Ninety minutes of SSC, with infants in incubators acting as their own control. Parents and caregivers were blinded to the measurements.
Main outcome measures Mean difference in rcO2 between SSC and incubator care; as well as heart rate (HR), SpO2, fraction of inspired oxygen (FiO2) and temperature, were compared using a paired t-test.
Results rcO2 was similar during SSC (mean (SD) 74.9 (6.5)%)% compared with incubator care (74.7 (6.1)%, mean difference (95% CI) 0.2 (−0.8 to 1.1)%, p=0.71). No clinically important differences in HR, SpO2, FiO2 or temperature were observed in the whole cohort and by mode of respiratory support (endotracheal tube mechanical ventilation, continuous positive airway pressure and high-flow nasal cannulae).
Conclusions Cerebral oxygenation and other physiological measurements in ventilated preterm infants did not differ between SSC and incubator care.
Trial registration number 12615000959572.
- Intensive Care
- Neonatology
- Neurology
- Physiology
Statistics from Altmetric.com
What is already known on this topic?
There are conflicting reports on the stability of oxygen saturation (SpO2) during skin-to-skin care, which may be a barrier for implementation in very preterm infants.
Both excessive and insufficient oxygen supply to the brain might contribute to morbidity and mortality in preterm infants.
Regional cerebral oxygenation (rcO2) measured non-invasively using near-infrared spectroscopy (NIRS) can serve as a surrogate parameter for brain oxygen supply and consumption.
What this study adds?
rcO2 during skin-to-skin care is stable and the intervention is non-inferior compared with incubator care for very preterm infants receiving respiratory support.
There was no difference in physiological parameters by mode of respiratory support or oxygen requirements.
Extremely preterm and very low birthweight infants are not more vulnerable to physiological instability during skin-to-skin care.
Background
Skin-to-skin care (SSC) is defined as placing an infant prone clad only in a nappy onto their mother's or father's bare chest. The approach originated in Bogota due to a shortage of staff and equipment1 to care for preterm infants and is increasingly being used in high-income countries.
SSC is beneficial to both term and preterm babies. It enhances breastfeeding success during the early postpartum period2 and increases the duration of breastfeeding after discharge.3 In very low birthweight (VLBW) infants, SSC has been associated with improved weight gain,4 a reduction in mortality, severe infection and length of hospital stay compared with standard care.5 ,6 Moreover, SSC in newborns immediately after birth stabilises cardiorespiratory adaptation7 and decreases duration of infant crying.8
Short-term studies of the physiological impact on preterm infants during SSC are conflicting. More frequent oxygen desaturations and a decrease in regular breathing patterns,9 or no difference10 or even fewer oxygen desaturations or bradycardic episodes during SSC have been reported.11 The uncertainty regarding physiological stability may be a barrier to wider implementation of SSC and more evidence, especially in extremely preterm infants is needed.12
Near-infrared spectroscopy (NIRS) measures tissue oxygenation at a depth of 1–2 cm using the absorptive characteristics of near-infrared light, by calculating the ratio between oxygenated and total haemoglobin.13 ,14 The technology can measure the regional oxygenation of most major organs but in newborns it is most commonly used to measure regional cerebral oxygenation (rcO2) using a sensor placed on the patient's forehead.15
There is a paucity of knowledge about rcO2 during SSC in preterm infants during their first days after birth during respiratory support. The aim of our study was to measure and compare rcO2, oxygen saturations (SpO2), heart rate (HR) and fraction of inspired oxygen (FiO2) before, during and after SSC in preterm infants receiving respiratory support. We hypothesised that rcO2 during SSC (intervention) would be non-inferior to incubator care (control).
Methods
Study design and oversight
The single-centre observational non-inferiority trial was conducted at the Royal Women's Hospital (RWH), Melbourne, which is a tertiary perinatal centre with >7500 births and over 280 admissions of very preterm infants (<32 weeks' gestation) to the neonatal intensive care unit each year. Approval was obtained from the RWH Human Research and Ethics Committee. Written informed prospective parental consent was obtained and the study was registered with the Australian and New Zealand Clinical Trial Registry: identifier 12615000959572.
Patients
Infants were eligible if they were born <33 weeks' gestation and were receiving respiratory support (mechanical ventilation through endotracheal tube (ETT), nasal continuous positive airway pressure (CPAP) or high-flow nasal cannula (HFNC)). Exclusion criteria were any cerebral malformations, posthaemorrhagic ventricular dilatation or grade III–IV intraventricular haemorrhage.16 Our hospital guidelines do not recommend SSC while infants have umbilical catheters in situ or cardiovascular instability (eg, treatment with inotropes) and so these infants were excluded.
Equipment
NIRS and definitions
The rcO2 was measured continuously using NIRS (Fore-sight, CAS Medical Systems, Branford, Connecticut, USA). With rcO2 and SpO2, the cerebral fractional tissue oxygen extraction (cFTOE) can be calculated (cFTOE=SpO2–rSO2)/SpO2) to estimate the balance between oxygen delivery and oxygen consumption.17 cFTOE was calculated for each time point. Variability in rcO2 was assessed using the SD around each infant's mean rcO2. The proportion of time spent in ‘cerebral hypoxia’ (rcO2 <55%) and ‘cerebral hyperoxia’ (rcO2 >85%)18 were calculated for each infant and study period.
Other physiological measurements and definitions
SpO2 and HR were measured by oximetry (Radical7 V5; Masimo, Irvine, California, USA). Bradycardic events were defined as HR <100 bpm for >5 s, hypoxic events were defined as SpO2 <80% for >5 s. The FiO2 was measured with a Teledyne oxygen analyser (AX300, Teledyne Analytical Instruments, California, USA) inserted into the inspiratory limb of the CPAP, HFNC or mechanical ventilation system. All signals (rcO2, SpO2, HR, FiO2) were digitised and recorded at 200 Hz using the NewLifeBox Neo-RSD physiological monitor (Advanced Life Diagnostics UG, Weener, Germany). Axillary temperature was recorded just after incubator care and SSC (digital clinical thermometer, Livingstone, New South Wales, Australia).
Study intervention
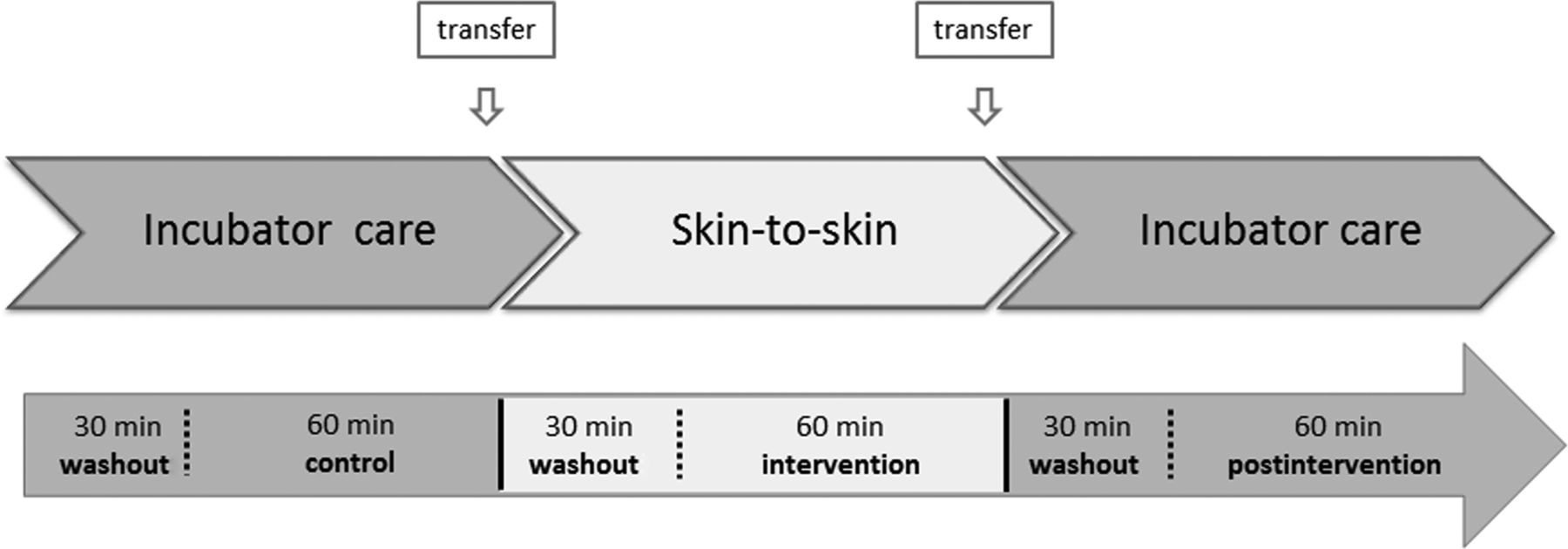
Continuous recordings were performed and divided in different study periods (figure 1). In this way, every infant served as his/her own control. We anticipated some physiological instability during transfer of the infant between incubator and SSC (and vice versa) and a predefined washout period of 30 min was incorporated into the protocol. Previously published washout periods in more stable preterm infants were 10 min.10 Time of transfer was defined from start of handling until the end of handling after transfer. The NIRS sensor was placed on the right temporoparietal area of the scalp above the ear and held in place by a firm fitting hat (figure 2). No replacement of the NIRS probe was necessary between or within the study periods. Parents and caregivers were blinded to the rcO2 measurements. To avoid changes in rcO2 due to position (supine, prone or degree of head-up),19 every effort was made to ensure that all infants were kept in the head-tilt prone position with their body elevated by about 15° in the incubator as well as during SSC by standardising the angle of the recliner during SSC. SSC was performed for a minimum of 90 min and for as long as the parent felt comfortable, with the first 60 min following washout used in the analysis. During SSC, infants were naked except for a nappy and a hat and held in the kangaroo position covered by blankets. Infants received their feeds at 2–3 hourly intervals via a nasogastric tube. The study was timed according to parental availability and not according to the feeding schedule. Therefore, no analysis of the effect of feeding on physiological parameters was performed.

Graphical presentation of the study design with its different study periods.

Preterm infants during skin-to-skin care with the near-infrared spectroscopy sensor placed on the right temporoparietal area of the scalp fixed by a firm fitting hat.
Study outcomes
The primary outcome was each infant's mean rcO2 during each period (intervention (SSC) and control (incubator care)). Prespecified secondary outcomes included SpO2, HR, FiO2, cFTOE and axillary temperature, each estimated as the mean for each infant during each time period.
Statistical analysis
Continuous data were summarised as mean (SD) if symmetrically distributed or median (IQR) if skewed for each participant and according to the predefined study periods. Categorical data were summarised as counts and percentages. For the primary and secondary outcomes, we analysed the difference of physiological parameters between control (incubator care) and intervention (SSC) using a paired t-test and 95% CI for the difference of paired means (the differences followed a normal distribution). In a subgroup analysis, we used the mean difference of physiological parameters (eg, mean difference of rcO2) as an outcome to compare different groups such as infants on different modes of respiratory support, infants needing supplemental oxygen, extremely preterm infants (<28 weeks' gestation) and extremely low birthweight infants (ELBW infants, <1000 g). We also compared each infant's mean values for all physiological data between intervention (SSC) and postintervention (incubator care) and between control (incubator care) and postintervention (incubator care). Student's t-test was performed to compare the mean differences between two groups, whereas one-way analysis of variance and Scheffe's test was used to compare mean differences between more than two groups. A p value of <0.05 was considered to be statistically significant. All analyses were performed using STATA software (Intercooled V.13, StataCorp, College Station, Texas, USA).
Sample size
The primary outcome was the paired difference in percentage rcO2. The required sample size was therefore dependent on the SD of these paired differences. Before we began the study, we had no estimate as to the probable size of this SD, so we calculated our required sample size (68 patients) based on effect size assuming SSC was 0.1 SD worse than incubator care, and a non-inferiority margin of 0.5 SDs. A provisional analysis after the first 15 patients were enrolled showed the SD of the paired differences in our sample to be 1.8. At this point, the sample size was recalculated using conservative estimates of SD (2.0) and a non-inferiority margin of 1.5%. With 40 patients, the study would have greater than 90% power that the lower end of the 95% CI for the paired difference in rcO2 will be more than −1.5%, assuming that the true difference between SSC and incubator care is −0.2%, and the SD of the paired difference in rcO2 is 2.0.
Results
From September 2015 to April 2016, 40 preterm infants receiving respiratory support were recruited. Characteristics of the study group at time of SSC are summarised in table 1.
Subject demographics
Physiological parameters at all study time points, including the transfer from incubator care to SSC, are summarised in table 2.
Physiological measurements during study period
Comparison between intervention and control
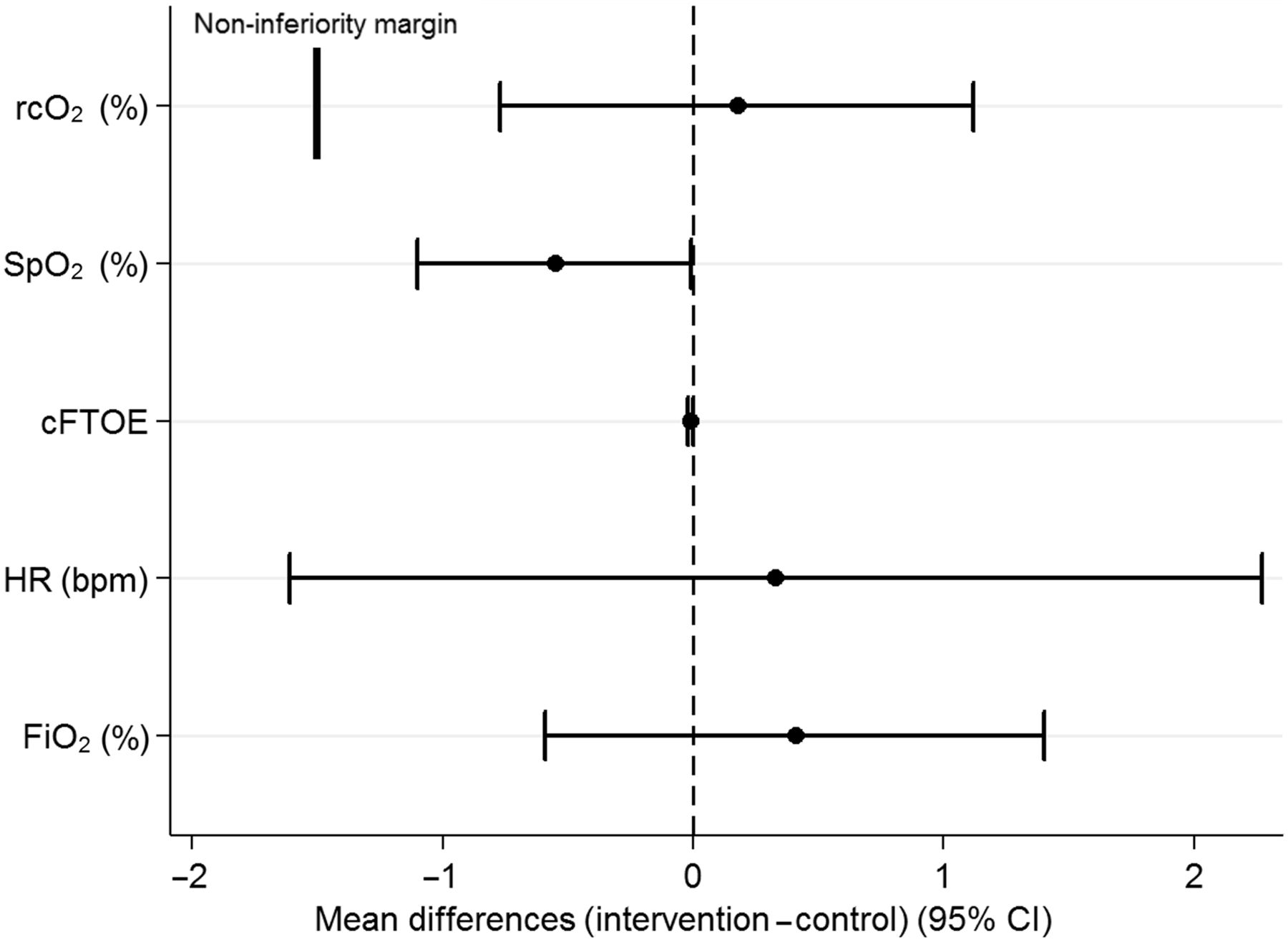
There was little evidence of a difference in the primary outcome (rcO2) during the intervention (mean (SD) 74.9 (6.5)%) compared with the control (74.7 (6.1)%, mean difference (95% CI) 0.2 (−0.8 to 1.1)%, p=0.71). There were no clinically important differences in cFTOE (p=0.23), HR (p=0.74), FiO2 (p=0.41), but a statistically significant and also not clinically important decrease in SpO2 during the intervention (93.6 (2.8)%) compared with control (94.1 (3.0)%, p<0.05). Mean differences and 95% CI are shown graphically in figure 3.
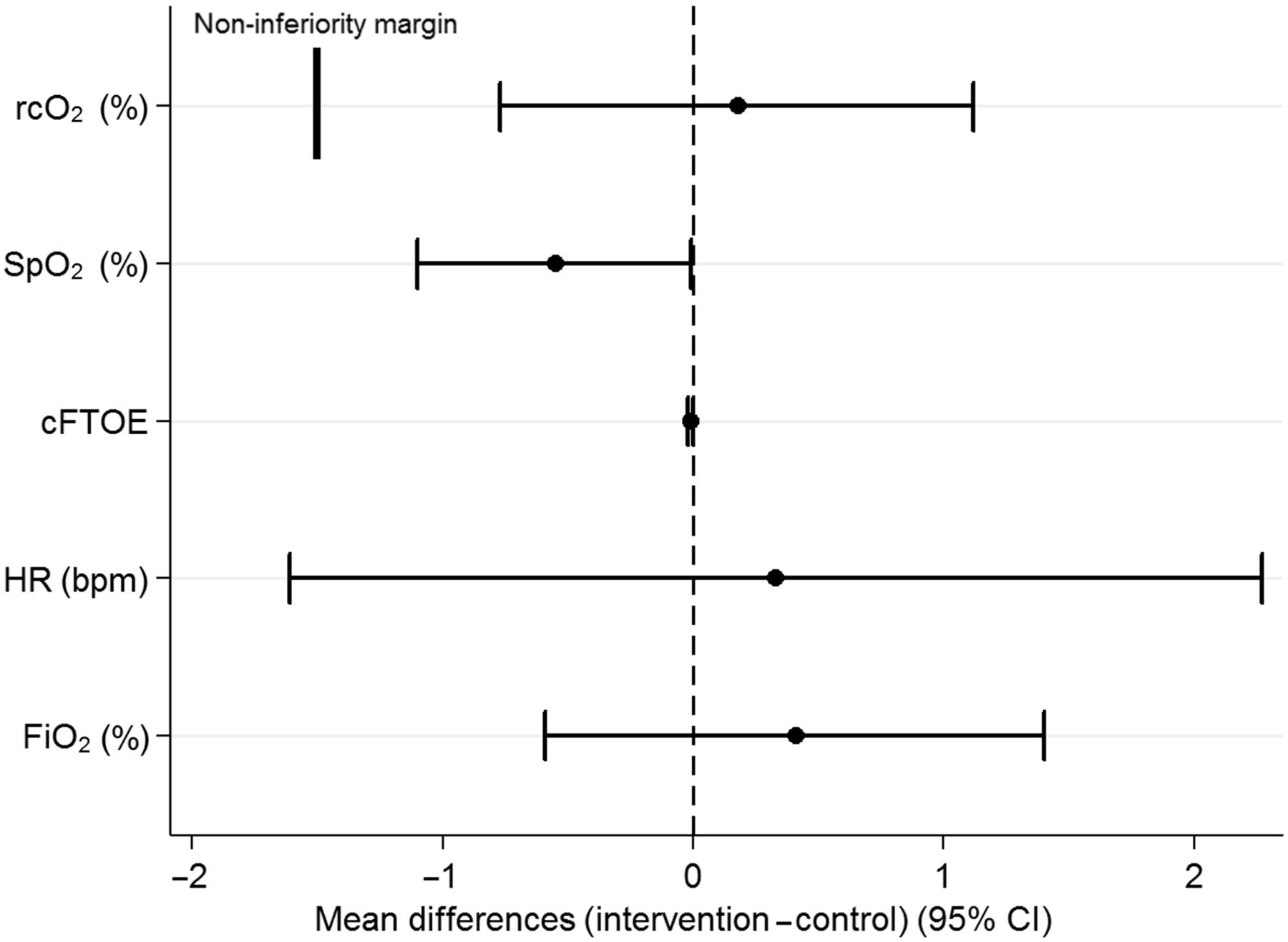
Absolute mean differences (95% CI) in regional cerebral oxygenation (rcO2), oxygen saturations (SpO2), heart rate (HR), fraction of inspired oxygen (FiO2) and cerebral fractional tissue oxygen extraction (cFTOE) between skin-to-skin care and incubator care.
There was little evidence of a difference in temperature (intervention: 36.8 (0.4)°, control: 36.8 (0.3)°, mean difference 0.04 (−0.1 to 0.2)°, p=0.58).
Comparison between intervention and postintervention
There is a small but statistically significant decrease in rcO2 during postintervention (mean (SD) 73.7 (6.9)%) compared with intervention (74.9 (6.5)%, mean difference (95% CI) −1.2 (−2.1 to −0.3)%, p<0.01). In comparison, SpO2 increases during postintervention (94.1 (2.9)%) compared with intervention (93.5 (2.7)%, 0.6 (0.1 to −1.0)%, p<0.05). There was little evidence of a difference in HR (p=0.35) or FiO2 (p=0.18).
Comparison between control and postintervention
There was little evidence of a difference in rcO2 (p=0.13), SpO2 (p=0.61), cFTOE (p=0.18), HR (p=0.39) and FiO2 (p=0.74) between control and postintervention.
Variability in parameters between control and intervention
There was little evidence of a difference between the SD around each infant's mean rcO2 between intervention (mean (SD) 2.7 (1.6)) and control (2.4 (1.3), mean difference (95% CI) 0.24 (−0.1 to 0.6), p=0.19). There was little evidence of a difference in the mean proportion of time spent in cerebral hypoxia between intervention (0.6 (2.8)%) and control (0.2 (1.1)%, 0.4 (−0.5 to 1.3)%, p=0.41) and similarly there was little evidence of a difference in the mean proportion of time spent in cerebral hyperoxia between intervention (4.3 (14.8)%) and control (3.2 (11.3)%, 1.1 (−1.2 to 3.3)%, p=0.35). The box plots in figure 4 illustrate the variability in rcO2 within the study population over different study periods in relation to rcO2 reference ranges.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plots showing regional cerebral oxygenation (rcO2) over different study periods. The dotted lines are the normal ranges of rcO2.
There was little evidence of a difference in the number of bradycardic events between intervention (0.0 (0.0)) and control (0.1 (0.2), −0.1 (−0.1 to 0.1), p=0.16) and similarly there was little evidence of a difference in the number of hypoxic events between intervention (2.1 (5.8)) and control (1.1 (2.8), 1.0 (−0.3 to 2.2), p=0.15).
Mode of respiratory support and oxygen dependency
There was little evidence of a difference in infants receiving mechanical ventilation through ETT (mean difference (95% CI) in rcO2 between intervention and control −0.2 (−2.7 to 3.1)%, n=10) compared with infants receiving nasal CPAP (−0.1 (−1.6 to 1.3)%, n=15) or HFNC (0.5 (−1 to 1.8)%, n=15, p=0.87). There was also little evidence of a difference between these three groups regarding SpO2, cFTOE, HR and FiO2.
There was little evidence of a difference in infants receiving supplemental oxygen (mean difference (95% CI) in rcO2 between intervention and control 0.3 (−1.2 to 1.8)%, n=24) compared with infants in air (−0.01 (−1.0 to 1.0)%, n=16, p=0.75). There was also little evidence of a difference between these two groups regarding SpO2, cFTOE, HR and FiO2.
Extremely preterm infants (<28 weeks' gestation)
There were 23 extremely preterm infants in our cohort and the mean difference (95% CI) in rcO2 between intervention and control was 0.6 (−0.8 to 2.0)%, compared with the 17 infants of ≥28 weeks' gestation, where the mean difference in rcO2 between intervention and control was −0.4 (−1.6 to 0.9)%, p=0.32. In the 21 extremely low birthweight infants, the mean difference in rcO2 between intervention and control was 0.3 (−1.2 to 1.9)%, compared with the 19 infants with birth weight ≥1000 g, where the mean difference in rcO2 between intervention and control was 0.01 (−1.2 to 1.2)%, p=0.74.
Transfer from incubator care to SSC
There was a statistically significant difference in rcO2 between transfer from incubator to SSC (mean (SD) 71.6 (7.9)%) compared with control (74.7 (6.1)%, mean difference (95% CI) −3.0 (−1.9 to −4.1)%, p<0.0001). Additionally, there was a decrease in SpO2 (−3.1 (−1.7 to −4.5)%, p<0.0001) and an increase in HR (8.5 (5.3 to 11.7) bpm, p<0.0001) and FiO2 (1.7 (0.4 to 2.9)%, p<0.05). cFTOE remained unchanged (0.01 (−0.01 to 0.02), p=0.43).
The duration of transfer to SSC was median (IQR) 4.0 (3.0–6.7) min and back to the incubator was 5.0 (3.5–7.7) min.
Discussion
To the best of our knowledge, this is the first study comparing rcO2 during SSC with incubator care in preterm infants receiving respiratory support.
The rcO2 and other physiological parameters were unchanged during SSC compared with incubator care independent of the mode of respiratory support or oxygen requirement and size of infants (extremely preterm or ELBW). We observed some statistically significant changes in physiological parameters between SSC and postintervention (increase in rcO2 by ∼1% and decrease in SpO2 by ∼0.5%), these changes however are not of clinical importance. No changes were observed between both incubator periods (control and postintervention), which highlights that SSC did not cause long-lasting disturbance in physiological parameters.
Our findings replicate a previously published observational study reporting minimal differences in rcO2 during SSC, but these infants were studied at a much later age (postmenstrual age of 36 weeks).20 In contrast, our cohort was of lower gestational age, birth weight and postnatal age. In addition, infants in this study were receiving respiratory support, which may potentially render them to be more unstable during SSC and the transfers between incubator, SSC and vice versa.
The effect of SSC on stability of HR and oxygenation varies across studies. Bohnhorst et al reported an increased rate of bradycardic and hypoxaemic events in preterm infants during SSC.9 Our findings are similar to others who reported no deteriorations in HR, SpO221 or temperature22 during SSC. One hypothesis for these discrepancies might be that respiratory stability of the premature infant is influenced by the caregiver’s cardiac rhythm during SSC.23
This is the first study to report physiological parameters during the transfer of infants from the incubator to the parental chest for SSC. Transfer of the infant to and from SSC resulted in a small drop in infant's SpO2 and rcO2 with increased HR and FiO2 but unchanged cFTOE, which levelled out during SSC. This observation highlights the sensitivity of preterm infants to handling. Optimising procedures for the transfer to and from SSC without loss of positive end expiratory pressure (PEEP) might further improve the stability of infants (and parental confidence) receiving SSC by potentially preventing minor deteriorations in SpO2 and rcO2. Our data are however reassuring as cFTOE, which describes the balance between oxygen delivery and oxygen consumption,17 remained stable even during the transfer to and from SSC. Moreover, the changes observed during transfer (drop in rcO2 and SpO2 by ∼3%, increase in HR by ∼8% and increase in oxygen requirement by ∼2%) are unlikely to be of clinical importance.
The strength of this study is that highly vulnerable preterm infants receiving different modes of respiratory support were studied at an early postnatal age and stage of their SSC experience. Similarly, others demonstrated feasibility of providing SSC to extremely preterm infants (mean gestational age of 25 weeks) in the first 6 days after birth.24 A limitation of our study is that it was not powered to show differences in the subgroups (eg, infants receiving different modes of respiratory support).
There is still a lack of evidence in physiological stability during SSC in extremely preterm infants within the first 72 hours after birth. However, we provide some physiological evidence that SSC in preterm infants receiving respiratory support is feasible while maintaining stable brain oxygen saturations levels.
Conclusion
SSC provides comparable physiological stability to incubator care in preterm infants receiving respiratory support. Using rcO2, SpO2, HR, FiO2 and skin temperature as markers of physiological stability, providing SSC to preterm infants receiving respiratory support is feasible and should be encouraged.
Acknowledgments
We would like to acknowledge the staff at the Royal Women's Hospital neonatal unit and also all the parents and infants who participated in the study.
References
Footnotes
Funding Research fellowship from the German Research Society for Dr Laila Lorenz (DFG-grant nr. LO 2162/1-1). The National Health and Medical Research Council (NHMRC) funding Professor Peter G Davis (App ID 1059111), Dr C Omar F Kamlin (App ID 1073533), Associate Professor Jeanie Cheong (App 1053787), Associate Professor Susan Jacobs (App 1073103), NHMRC programe grant for PGD, COFK, JAD, Australia.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval Royal Womens Hospital Human Research and Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.