Article Text

Abstract
Background Clinical assessment of newborn heart rate (HR) at birth has been reported to be inaccurate. NeoTapAdvancedSupport (NeoTapAS) is a free-of-charge mobile application that showed good accuracy in HR estimation. This study aimed to evaluate the impact of NeoTapAS on timing of HR communication and resuscitation interventions.
Methods This was a randomised controlled cross-over (AB/BA) study evaluating HR assessment using auscultation plus NeoTapAS compared with auscultation plus mental computation in a high-fidelity simulated newborn resuscitation scenario. Twenty teams each including three paediatric residents were randomly assigned to AB or BA arms. The primary outcome was the timing of the first HR communication. Secondary outcomes included the timing of the following four HR communications and the timing of resuscitation interventions (positive pressure ventilation, chest compressions, intubation and administration of first dose of epinephrine).
Results NeoTapAS reduced the time to the first HR communication (mean difference −13 s, 95% CI −23 to −4; p=0.009), and the time of initiation of chest compressions (mean difference −68 s, 95% CI −116 to −18; p=0.01) and administration of epinephrine (mean difference −76 s, 95% CI −115 to −37; p=0.0004) compared with mental computation.
Conclusions In a neonatal resuscitation simulated scenario, NeoTapAS reduced the time to the first HR communication and the time of initiation of chest compressions and administration of epinephrine compared with mental computation. This app can be especially useful in settings with limited availability of monitoring equipment, but further studies in clinical scenarios are warranted.
Trial registration number NCT03730025.
- NeoTapAS
- mobile application
- neonatal resuscitation
- heart rate
- timing
Statistics from Altmetric.com
What is already known on this topic?
Heart rate (HR) is the most important clinical indicator to evaluate the status of a newborn and to drive neonatal resuscitation.
Previous studies showed that NeoTapAdvancedSupport had good accuracy in estimating HR and could be a useful tool in resource-constrained settings.
What this study adds?
NeoTapAdvancedSupport reduced the time to the first HR communication and the time of initiation of chest compressions and administration of epinephrine compared with mental computation.
NeoTapAdvancedSupport could be a useful tool in settings with limited availability of monitoring equipment.
Introduction
Heart rate (HR) is the most important clinical indicator to evaluate the status of a newborn and to guide neonatal resuscitation.1 2 Furthermore, HR during the first minutes of life could be a predictor of early neonatal mortality and morbidity.3 International guidelines on neonatal resuscitation recommend assessing the HR by auscultation along the left side of the chest and by counting the number of beats in 6 s and multiplying by 10.1 2 Pulse oximetry and three-lead ECG monitor can also be used to assess HR in delivery room,1 but some limitations (ie, motion artefacts and delay in HR display when using pulse oximetry, and availability of three-lead ECG in delivery rooms) hamper their use especially in low-resource settings.
Assessing the HR by auscultation can be limited due to imprecise auscultation and/or errors in mental computation,4 5 leading to inappropriate or delayed resuscitation.1 Previous studies evaluated a free-of-charge mobile application (NeoTapAdvancedSupport, NeoTapAS)6 to help HR assessment in a simulated scenario of neonatal resuscitation.7 8 NeoTapAS showed good accuracy in estimating HR and could be a useful tool in resource-constrained settings.8
Another potential advantage of using NeoTapAS may be the faster communication of HR during resuscitation, because it avoids mental computation and possible errors due to the stressful situation.9 In addition, prompt HR assessment may lead to reducing times of initiation of resuscitation interventions. However, these hypotheses remain to be demonstrated.
The aim of this study was to evaluate the promptness in HR communication using NeoTapAS compared with mental computation in a high-fidelity simulated newborn resuscitation scenario. In addition, the impact of NeoTapAS on timing of resuscitation procedures was investigated.
Methods
Study design
This was a randomised controlled cross-over (AB/BA) study evaluating the promptness in HR communication using auscultation plus NeoTapAS compared with auscultation plus mental computation in a high-fidelity simulated newborn resuscitation scenario (ClinicalTrials.gov NCT03730025). The AB/BA scheme is uniform within sequences and periods, thus removing any period and sequence effects.10 The Ethics Committee of ‘Maggiore della Carità’ Hospital (Novara, Italy) deemed that a formal ethical approval was not required since the study used manikin data (Prot 759/CE). Participants gave their consent to record the scenario and to use the data.
Setting
This simulation study was performed at the SIMNOVA Center of the University of Piemonte Orientale in Novara (Italy). The scenario consisted of an asphyxiated term infant needing a complex resuscitation including positive pressure ventilation, endotracheal intubation, chest compressions and emergency medications (neonatal simulator manikin: Newborn HAL S3010; Gaumard Scientific, Miami, Florida), as described elsewhere.8 Briefly, HR, respiratory rate and breath sounds were controlled remotely and could be assessed by auscultation of the thorax and observation of chest movements. Oxygen saturation via pulse oximetry (SpO2) was displayed on the bedside monitor about 40 s after the positioning of the oximeter probe whereas HR was not available. The external observer provided verbal feedbacks during the scenario only if specifically required by the resuscitation team and not provided by the manikin (ie, the presence of secretions). A bedside Apgar timer was available for the resuscitation team.
Randomisation
All paediatric residents from third to fifth year of residency of the University of Piemonte Orientale who were trained on neonatal resuscitation participated in the simulation. They were divided into teams including three residents (one from each year of residency, in order to balance team experience) and were asked to assume the roles of team leader and assistants. After a short training on NeoTapAS and familiarisation with the manikin, residents were involved in the scenario. Teams were randomly assigned to AB or BA arms in a 1:1 ratio. Randomisation was performed using a computer-generated random assignment list. Arm assignments were included in sealed opaque envelopes sequentially numbered.
Procedures
Teams in AB arm were assigned to HR assessment by auscultation and tapping on NeoTapAS, followed by HR assessment by auscultation and mental computation. Participants in BA arm were assigned to the reverse sequence. A washout period of 1 day was included to reduce any carry-over effect.
During each simulation, the same resident responsible for HR assessment estimated the HR every 30 or 60 s by listening to the praecordium with a stethoscope. Ventilation and chest compressions were shortly paused during HR assessment. When using NeoTapAS, he/she simultaneously tapped the same pace on the screen of an iPad with the NeoTapAS app installed8 and verbally communicated the HR displayed on the screen. When using mental computation, he/she mentally calculated the HR based on auscultation (by counting the number of beats in 6 s and multiplying by 10) and verbally communicated the calculated HR.
All resuscitations were performed according to the Neonatal Resuscitation Program seventh edition algorithm, including the timing of HR assessment.11 All scenarios were video recorded, stored and reviewed by the same researcher (MB) to confirm the data collected during the simulation.
NeoTapAS is a free-of-charge mobile application specifically designed for registration of neonatal resuscitation events.6 It is based on a screen tapping method and calculates the HR after a minimum of three taps, allowing a fast recording of HR and a real-time event registration.8
Outcomes
The primary outcome was the timing of the first HR communication. The secondary outcomes included the timing of the following (second, third, fourth, fifth) HR communications and the timing of resuscitation interventions (positive pressure ventilation, chest compressions, intubation and administration of first dose of epinephrine).
Sample size
Assuming a true mean difference of 10 s (SD 15) in the primary outcome between the two methods, with type I error of 0.05 and a power of 0.80, 20 teams (10 in AB arm and 10 in BA arm) were required to be enrolled in the study.
Statistical analysis
Continuous data were expressed as mean and SD, and categorical data as number and percentage. The study included a washout period that was chosen to reasonably prevent carry-over effects. Since tests for carry-over effect are generally underpowered, the inclusion of an adequate washout period is strongly recommended to prevent carry-over effects.12 Primary and secondary outcomes were compared using the two-sample t-test approach on paired data (ie, two-sample t-test applied to the differences between period in the two arms).13 Period effects were also tested for with a similar approach (ie, two-sample t-test applied to the differences between methods in the two arms).13 All tests were two sided and a p value <0.05 was considered statistically significant. Statistical analysis was performed using R V.3.3.0 (R Foundation for Statistical Computing, Vienna, Austria).14
Results
Primary outcome
Timing of first HR communication is shown in table 1. Time to the first HR communication was shorter with NeoTapAS compared with mental computation (mean difference −13 s, 95% CI −23 to −4; p=0.009). No period effect was found (p=0.38).
Timing of heart rate communications
Secondary outcomes
Timing of second to fifth HR communications is shown in table 1. Time intervals to the second (mean difference −16 s, 95% CI −33 to 1; p=0.07) and to the third (mean difference −24 s, 95% CI −48 to 1; p=0.06) HR communications were slightly shorter with NeoTapAS compared with mental computation. No period effect was found (p=0.76 and p=0.77, respectively). NeoTapAS and mental computation had similar time intervals to the fourth and to the fifth HR communications (p=0.81 and p=0.53, respectively; table 1). No period effect was found (p=0.57 and p=0.85, respectively).
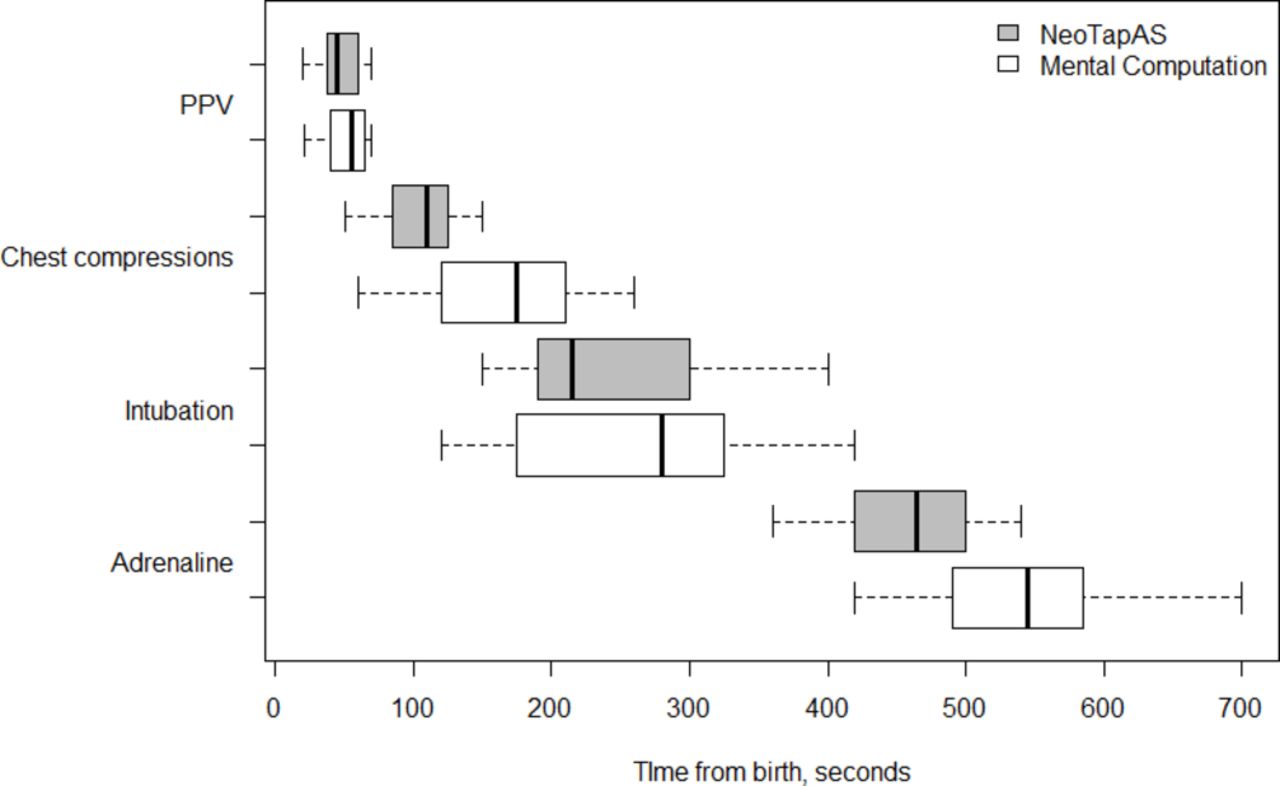
Timing of resuscitation interventions is shown in table 2 and figure 1. Start of positive pressure ventilation was similar with NeoTapAS and mental computation (mean difference −6 s, 95% CI −15 to 3; p=0.20). No period effect was found (p=0.93). Chest compressions started earlier with NeoTapAS compared with mental computation (mean difference −68 s, 95% CI −116 to −18; p=0.01). No period effect was found (p=0.30). Timing of intubation was similar with NeoTapAS and mental computation (mean difference −29 s, 95% CI −87 to 30; p=0.29). No period effect was found (p=0.10). First dose of epinephrine was administered earlier with NeoTapAS compared with mental computation (mean difference −76 s, 95% CI −115 to −37; p=0.0004). The period effect was close to statistical significance (p=0.07).

{kind=link}
Timing of positive pressure ventilation (PPV) and intubation, and in start of chest compressions and epinephrine: box and whisker plot. NeoTapAS, NeoTapAdvancedSupport.
Timing of resuscitation interventions
Discussion
In a neonatal resuscitation simulated scenario, NeoTapAS reduced the time to the first HR communication compared with mental computation. In addition, NeoTapAS shortened the time of initiation of chest compressions and administration of epinephrine compared with mental computation.
HR is the most important clinical indicator to guide appropriate interventions during neonatal resuscitation.1 2 HR evaluation by auscultation is currently recommended, but imprecise auscultation and/or errors in mental computation can reduce the precision of this approach.4 5 This limit can be overcome by the introduction of an instrumental aid. NeoTapAS is a free-of-charge mobile application6 that proved good accuracy in estimating HR in manikin studies.7 8 This application can be especially useful in settings where monitoring equipment (ie, pulse oximetry and three-lead ECG) is lacking.
Beyond good accuracy, using this application may allow to haste HR communication during neonatal resuscitation. Our study showed that NeoTapAS reduced the time to the first HR communication of a mean of 16 s compared with mental computation. Furthermore, NeoTapAS seemed promising in reducing the second and third HR communications, but these outcomes needed to be addressed in further studies.
The scope of shortening the times of HR communication is to reduce the time of initiation of resuscitation interventions. Our results indicated that NeoTapAS shortened the start of chest compressions (by a mean of 68 s) and the administration of the first dose of epinephrine (by a mean of 76 s) compared with mental computation. The magnitude of these time reductions may be clinically relevant in neonates needing advanced resuscitation, because the timing of cardiovascular support plays a crucial role in neonatal resuscitation.1 2 However, the benefit of NeoTapAS in shortening the time of epinephrine administration may be different in senior neonatologists and in paediatric residents.
Despite the times for positive pressure ventilation and intubation were shorter with NeoTapAS, the study was underpowered to demonstrate such differences. Surprisingly, NeoTapAS was not associated with early initiation of positive pressure ventilation, despite the faster communication of first HR. In our study, we observed that positive pressure ventilation was performed before first HR communication in 7 of 10 procedures, thus suggesting a decision based on observed apnoea. In fact, international guidelines recommend to start positive pressure ventilation in case of apnoea and/or gasping and/or HR below 100 bpm.1 2
Overall, the resuscitation interventions were performed in the appropriate sequence,1 despite wide heterogeneity of starting times of chest compressions, intubation and epinephrine administration. Readers should be aware that all times for procedures reported in our study were a result of scenario/human factors combined with NeoTapAS (and not exclusively the latter).
This is the first study evaluating the impact of a mobile application for HR assessment (NeoTapAS) on the times of HR communication and of resuscitation procedures in a high-fidelity simulated newborn resuscitation scenario. A recent study suggested that a quick and reasonably accurate HR assessment could be achieved by auscultation in low-risk newborns (ie, those not anticipated to need resuscitation and those with HR >100 bpm), but no conclusions could be drawn for infants needing resuscitation or in the setting of bradycardia.14 According to our findings and to the good accuracy reported in a simulated scenario of neonatal asphyxia,8 NeoTapAS can be a promising instrument for neonatal resuscitation, but further studies should evaluate its impact on real-life situation and neonatal outcomes.
This study has some limitations that should be considered when reading the results. First, findings from a simulation study might be different in a real-life situation where other clinical signs are available. Second, participants were paediatric residents with limited experience in neonatal resuscitation, while more experienced healthcare providers (ie, neonatal intensive care unit staff) may achieve different results. Third, accuracy and appropriateness of the interventions were not evaluated because they were beyond the scope of this study. Further investigation is needed to assess these important aspects.
Conclusions
In a neonatal resuscitation simulated scenario, NeoTapAS reduced the time to the first HR communication and the time of initiation of chest compressions and epinephrine administration compared with mental computation. This app can be especially useful in settings with limited availability of monitoring equipment. Further studies are needed to evaluate the impact of this app in real-life situation and neonatal outcomes.
Acknowledgments
We thank all paediatric residents who were involved in this study.
Footnotes
Contributors FC and DT carried out the analyses and drafted the work. MB, PLI, GG, SR and AM designed the work, acquired the data and reviewed the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The Ethics Committee of ‘Maggiore della Carità’ Hospital (Novara, Italy) deemed that a formal ethical approval was not required since the study used manikin data (Prot 759/CE).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.