Article Text

Abstract
Bone development is usually seen as a process of bone mineral accretion or increase in bone mass, and treatment of bone disorders usually consists of attempts to maximise bone mass accumulation by nutritional means only. However, from a functional perspective, bones should not be as heavy as possible, but rather as stable as necessary. It is therefore important to create conditions that stimulate bones to become more stable.
- skeletal development
- premature
- bone physiology
Statistics from Altmetric.com
The prevention and treatment of bone disorders is an important aspect of the care of preterm babies and, accordingly, a considerable amount of literature has been dedicated to this topic.1–3 However, the focus is almost exclusively on nutritional considerations. Although there can be no doubt that a sufficient and balanced supply of energy, proteins, vitamins, calcium, phosphorus, and other nutrients is an essential prerequisite for normal bone development, the basic facts about bone physiology often receive little consideration. The purpose of this contribution is to highlight some of these topics rather than to give an exhaustive review of bone disease in prematurity.
DEFINITIONS
What is bone density?
In physics, density was defined by Archimedes as the mass of a body divided by its volume (called “physical density” here). In clinical practice and science, “bone density” usually has a different meaning: the degree to which a radiation beam is attenuated by a bone, as judged from a two dimensional projection image (= areal bone density). It is important to remember that the attenuation of a radiation beam not only depends on physical density, but also on bone size—that is, the length of the path that the beam takes across the bone. A small bone therefore has a lower areal bone density than a larger bone, even if the physical density is the same (fig 1). This is true for both the subjective estimation of bone density from standard radiographs and its quantitative assessment by widely available densitometric methods, such as single photon absorptiometry and dual energy x ray absorptiometry.4 A low areal bone density value can therefore simply reflect the small size of an otherwise normal bone.

Comparison of density, as defined in physics, and radiological (areal) bone density, as commonly used in the clinical setting. The two bones have the same physical density, but the larger bone appears denser when projected on to a screen. The reason is that it absorbs more radiation because of the longer path length of the radiation beam through the bone. This is analogous to comparing the shadows of two differently sized bottles placed in the sun. The larger bottle will have a darker shadow, even if the two bottles are made of the same material and contain the same liquid. Similarly, the areal bone density of a premature infant with a birth weight of 1000 g is lower than that of a healthy term newborn, even if the physical density of the bones is identical.
What is bone mineralisation?
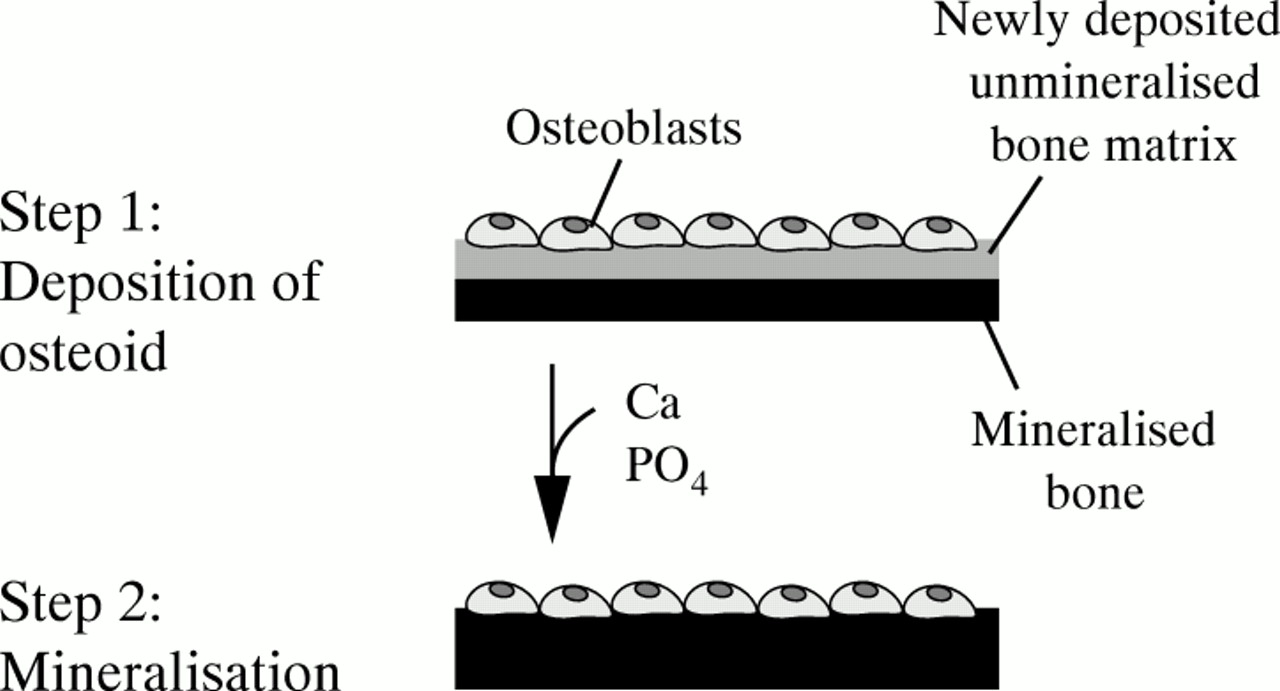
The physiological process of mineralisation represents the incorporation of mineral (Ca, P, and others) into organic bone matrix (osteoid), after it has been synthesised and deposited by osteoblasts (fig 2).5, 6 However, many reports on bone development in premature babies use statements such as “bone mineralisation has increased” to describe the radiological finding that areal bone density or bone mineral content (the mass of mineral per unit bone length) has increased from one measurement to the other. The meaning of the term “mineralisation” in these two circumstances is by no means identical. An increase in areal bone mineral density or bone mineral content can occur after the incorporation of mineral into pre-existent bone matrix, but can also result from an increase in bone size, thickening of bone cortex or trabeculae, or synthesis of new trabeculae. The latter processes represent formation of new bone tissue, where the incorporation of mineral into organic matrix is just one of several steps (fig 2). The main point here is that mineralisation can only occur where organic bone matrix has previously been deposited. Therefore, what is commonly called “decreased bone mineralisation” can reflect one of two things: either not enough organic matrix has been deposited (step 1 in fig 2) or not enough mineral has been incorporated into the matrix (step 2). These two possibilities correspond to the two most common pathological conditions of the premature skeleton: osteomalacia and osteopenia.

Schematic representation of the bone formation process. Firstly, a team of osteoblasts synthesises organic bone matrix and deposits it on an already existing surface of mineralised bone. This can be the surface of a trabecula or of the bone's cortex. In a second step occurring several days later, mineral is added to the newly deposited organic matrix.
What is osteomalacia?
Osteomalacia is a disorder of the physiological process of mineralisation—that is, the incorporation of mineral into the organic bone matrix is disturbed (step 2 in fig 2).7 This leads to an accumulation of unmineralised bone matrix, because osteoblasts continue to secrete osteoid for some time. The average mineral content of bone matrix is therefore decreased and the bone is soft, as is often clinically apparent from occipital flattening. The mineralisation defect is not limited to bone tissue, but also involves the growth plate cartilage, causing the clinical picture of rickets. Thus “osteomalacia” denotes defective mineralisation of organic bone tissue, whereas “rickets” describes defective mineralisation of growth plate cartilage and its morphological consequences.7 As long as growth plates are open, both conditions almost always coexist.7 Bone mineral density (both physical and areal) and bone mineral content are decreased in osteomalacia (fig 3), and the trabeculae have a washed out appearance on radiographs. Rickets can be recognised on radiographs from the irregular border between growth cartilage and the bony metaphysis and, where secondary ossification centres are present, by an increased width of the epiphyseal plate.8

Conditions affecting bone mineral content and density in premature infants. Shown are schematic bone cross sections. Mineralised bone matrix is indicated in black, and unmineralised bone matrix in grey. The small bone has a lower bone mineral content and areal bone mineral density than the normally sized bone, although it is otherwise completely normal. In osteomalacia, there is too much unmineralised bone matrix because not enough mineral has been incorporated into the matrix (mineralisation defect). In osteopenia, there is not enough bone matrix, but the matrix that is there has been filled with mineral in a normal fashion (no mineralisation defect).
What is osteopenia?
This term refers to a decreased amount of bone tissue (osteopenia = scarcity of bone). The structural basis of osteopenia is decreased thickness or number of trabeculae and/or decreased thickness of the bone cortex (fig 3).5, 9 Osteopenia is caused by either insufficient deposition (step 1 in fig 2) or increased resorption of organic bone matrix. In contrast with osteomalacia, the incorporation of calcium and phosphate into organic bone matrix is not affected. Accordingly, mineralisation of growth plate cartilage proceeds normally and there is no sign of rickets. However, similarly to osteomalacia, both physical and radiological bone mineral density and bone mineral content are decreased (fig 3).
It is a matter of some confusion that in the neonatological literature the term “osteopenia” is often used to describe the finding that radiological (areal) bone mineral density is decreased, whatever the cause. Thereby three different pathophysiological conditions are lumped together: decreased bone size, osteomalacia, and osteopenia (fig 3). It is important to clearly separate these three entities, as strategies for prevention and treatment are different.
What is osteoporosis?
According to criteria used in adults, osteoporosis is present when areal bone mineral density is below −2.5 standard deviations from the mean of young healthy adults.10 As areal bone mineral density depends on bone size (fig 1), this definition cannot be used in neonatology—all newborns would be diagnosed as having osteoporosis. At present, there is no generally acknowledged definition of osteoporosis in paediatrics. In our view, osteoporosis is present when bone stability is not adapted to mechanical requirements because bone mass is inadequately low and fractures have occurred after minor trauma. This means that osteoporosis should only be diagnosed when there is a history of such fractures.
PHYSIOLOGY AND PATHOPHYSIOLOGY OF POSTNATAL BONE DEVELOPMENT
Normal skeletal changes in the early postnatal period
The physical density of long bones such as the femoral diaphysis decreases by about 30% during the first six months of life.11 This is mostly due to an increase in marrow cavity size, which is faster than the increase in the cross sectional area of the bone cortex (fig 4). These radiographic changes have been classically called “physiological osteoporosis of infancy”.12 However, the most important criterion for the presence of osteoporosis according to our tentative definition given earlier—increased bone fragility—is absent.

Normal postnatal changes in the cross section of the femoral diaphysis. During the first six months of life, external bone size (bone diameter, d) increases by about 50%, whereas the thickness of the bone cortex decreases slightly. The total physical density of the femoral shaft—that is, density averaged over the whole cross section—decreases by about 30%, although the physical density of the cortex—that is, density averaged over the compartment shown in black—decreases only by 7%. The difference is due to the relatively larger marrow cavity which does not contain bone mineral. Even though total physical density decreases, the absolute amount of mineral increases (in this example total mineral content is calculated for a hypothetical 2 mm thick slice of the femur). However, the functionally most important aspect of these developments is that bone strength increases about threefold because of the changes in bone geometry.11
These postnatal adaptations of the skeletal system to extrauterine conditions should also occur in premature infants, with the difference that they happen earlier than in term babies. It is therefore of questionable use to compare the bones of preterm infants at expected term with those of term babies at birth, as has been done in many studies. The premature babies will already have started the process of postnatal adaptation, while the term newborns have not. Consequently one can expect to find differences between the two groups, and this is not necessarily a sign of bone disease in the preterm babies.
The reasons for the postnatal adaptations of the skeleton are not entirely clear, but it is obvious that the skeleton is exposed to different conditions before and after birth. Firstly, the mechanical stimulation is likely to be higher in utero. The regular fetal kicks against the uterine wall represent an intrauterine form of resistance training. After birth, the infant's movements typically occur without much resistance, thus putting smaller loads on the skeleton. Secondly, the hormonal situation is different postnatally, because the placental supply of oestrogen and many other hormones has been cut off. Despite these differences between intrauterine and extrauterine conditions, many authors postulate that the care of premature infants should aim to achieve intrauterine calcium accretion rates. It is, however, unknown whether the infant actually benefits from reaching this goal. It appears that, in the long run, the skeleton of these infants will adapt to the mechanical requirements, whether intrauterine calcium accretion rates are achieved or not.13–20
Causes of osteomalacia/rickets in premature infants
Both osteomalacia/rickets and osteopenia can occur after premature birth, but the causes of these disorders are different. As in older children, osteomalacia/rickets is generally due to a deficient supply or uptake of mineral. When premature babies are fed human milk, the supply of both calcium and phosphorus is low, but the critical factor leading to osteomalacia/rickets is the lack of phosphorus.21 Serum phosphate levels decrease and there is not enough substrate for incorporation into the organic bone matrix.
Biochemically, osteomalacia/rickets is characterised by an increase in serum levels of alkaline phosphatase. As a rule of thumb, the acceptable upper limit for alkaline phosphatase activity in premature babies can be taken to be about 5 times the upper reference range used for adults.21 However, it must be kept in mind that serum alkaline phosphatase activity is the sum of three isoforms (bone, liver, intestine). Therefore raised serum levels are not necessarily a sign of a mineralisation defect but can also be due to a high growth rate or a disorder of liver function.
Causes of osteopenia in premature infants
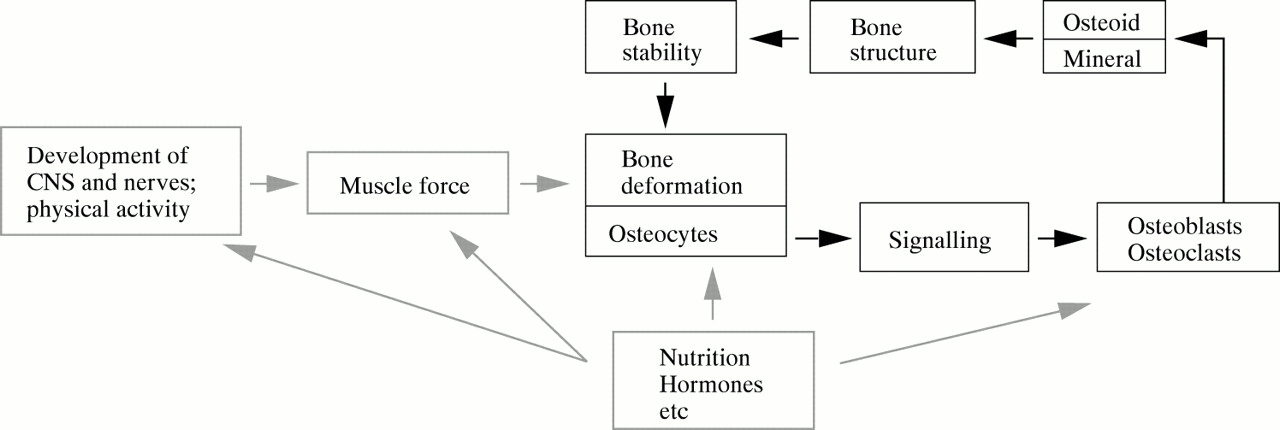
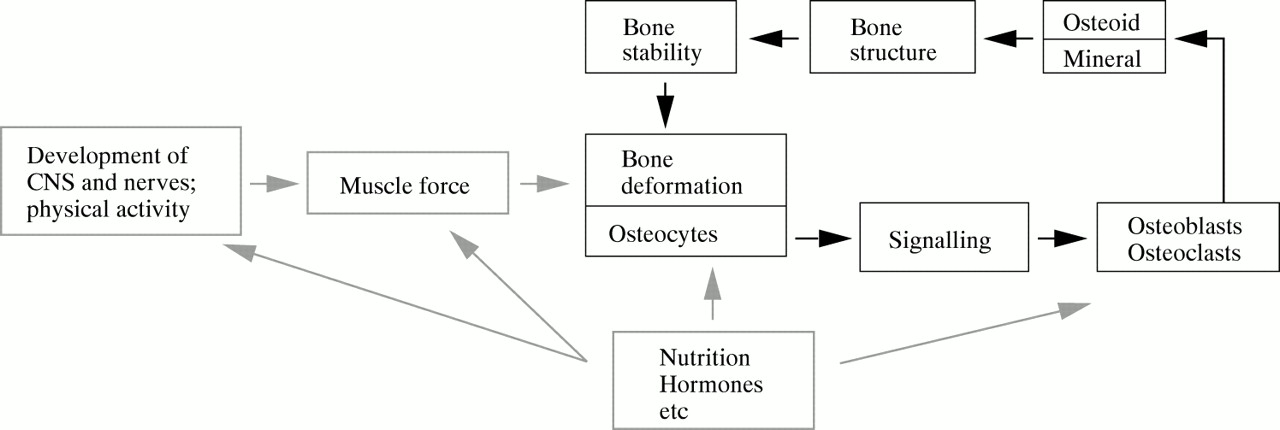
Osteopenia results from diminished synthesis and/or increased resorption of organic bone matrix. This can be caused by severe systemic disease, a drug side effect—for example, corticosteroids—or lack of mechanical stimulation (“disuse osteoporosis”). Although the first two items on this list are widely acknowledged, the importance of mechanical stimulation has long been neglected in neonatology. However, similarly to other organ systems, skeletal development is driven by functional requirements (fig 5). This means that bone strength increases when and where it is required to maintain bone stability. Under physiological conditions, the largest challenges to bone stability result from muscle contraction and not just from passive gravity, as is often assumed.22 Therefore, the stability of a bone must be adapted to local muscle force. The importance of this muscle-bone interaction is particularly obvious in newborns with muscular hypotonia of intrauterine onset, who often have fractures at birth.23, 24 However, lack of mechanical stimulation is not limited to these rare cases, but may be an important problem in neonatology.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The mechanostat model of bone development according to Frost.25, 26 The central regulatory unit of bone development is the feedback mechanism between bone deformation and bone stability (black boxes and thick black arrows). Osteocytes act as sensors of bone deformation. If deformation exceeds a preset threshold, osteocytes cause osteoblasts and osteoclasts to adapt the bone tissue to the increased load. Thereby bone stability increases and the bone is deformed less by the same load. In children, the loads on the bones increase continuously as the result of growth in length and increasing muscle force. Consequently, bone stability is continuously adapted “upwards”. However, during inactivity, bone stability can also be adapted “downwards”—that is, the bones get weaker. Nutrition, hormones, and other factors modulate the regulatory feedback loop at various sites (grey boxes and arrows).
An adequate supply of substrate (including minerals) is obviously a prerequisite for synthesis of bone tissue. However, the substrate will only be put to use, if it is actually needed for bone formation. These needs are determined by two factors: increase in bone length and increase in cross sectional bone strength (increase in bone width and cortical thickness, etc). As nutritional and mechanical factors have different roles in bone development, they cannot substitute for each other. Thus, when the mechanical challenge posed by muscles is lacking, the skeletal system “sees” no reason to increase its strength, and less new bone is added. In such a situation, it is questionable whether osteoblasts can be “talked into” increasing bone strength, just because large amounts of mineral are offered.
Bone disorders in premature babies are much less common now than in the 1980s, when extremely high fracture rates were reported.3 This is often perceived exclusively as a result of improved nutritional management.3 However, ventilation times and the concomitant immobilisation have decreased considerably during the same period, which may have played an important part in improving bone development. Further improvements in clinical care may be achieved by actively making use of the muscle-bone relation shown in fig 5. For example, Moyer-Mileur et al27 performed a physical activity programme in very low birthweight infants, who “exercised” their extremities against passive resistance for 5–10 minutes a day. The exercise group had greater gains in body weight, fat-free mass, forearm length, and bone mineral content than a non-exercising control group.
CONCLUSIONS
Bone development is traditionally viewed as a process of “bone mineral accretion” or an “increase in bone mass”. Therapeutic interventions are usually presented as attempts to maximise bone mass accumulation by nutritional means only. However, from a functional perspective, bones should not be as heavy as possible, but rather as stable as necessary. It is therefore important to create conditions that stimulate bones to become more stable. We suggest that functional bone physiology can be used to devise strategies for improved bone development in premature infants.