Article Text

Abstract
Objectives To examine if therapeutic hypothermia reduces the composite outcome of death, moderate or severe disability at 18 months or more after mild neonatal encephalopathy (NE).
Data source MEDLINE, Cochrane database, Scopus and ISI Web of Knowledge databases, using ‘hypoxic ischaemic encephalopathy’, ‘newborn’ and ‘hypothermia’, and ‘clinical trials’ as medical subject headings and terms. Manual search of the reference lists of all eligible articles and major review articles and additional data from the corresponding authors of selected articles.
Study selection Randomised and quasirandomised controlled trials comparing therapeutic hypothermia with usual care.
Data extraction Safety and efficacy data extracted independently by two reviewers and analysed.
Results We included the data on 117 babies with mild NE inadvertently recruited to five cooling trials (two whole-body cooling and three selective head cooling) of moderate and severe NE, in the meta-analysis. Adverse outcomes occurred in 11/56 (19.6%) of the cooled babies and 12/61 (19.7%) of the usual care babies (risk ratio 1.11 (95% CIs 0.55 to 2.25)).
Conclusions Current evidence is insufficient to recommend routine therapeutic hypothermia for babies with mild encephalopathy and significant benefits or harm cannot be excluded.
- hypoxic ischaemic encephalopathy
- therapeutic hypothermia
- meta-analysis
- newborn
Statistics from Altmetric.com
What is already known on this topic?
Therapeutic hypothermia for 72 hours reduces death and improves survival without disability during infancy and mid childhood after moderate or severe neonatal encephalopathy and is now the standard care therapy for these babies.
A therapeutic drift to extending the cooling therapy to babies with mild encephalopathy has been reported in the UK and other high-income countries.
What this study adds?
Adverse neurological outcomes at 18 months or more, occur in 20% of babies with mild encephalopathy.
Pooled data from five cooling trials inadvertently recruiting babies with mild encephalopathy do not exclude significant therapeutic benefits or harm
Introduction
Although therapeutic hypothermia is only recommended as the standard therapy for babies with moderate or severe neonatal encephalopathy (NE), a therapeutic creep has been reported worldwide.1 In the UK, 67% of the cooling centres routinely cool babies with mild NE, and at times for shorter durations than the recommended 72 hours for moderate or severe NE.1 There are concerns with such practices, as the cessation of cooling therapy prior to 24 hours following an apparent clinical recovery may be associated with residual brain injury and adverse outcomes.2 Furthermore, cooling therapy in the absence of NE may induce apoptosis.3 In contrast to the systematic review of cooling in mild NE reported by Conway et al, our review includes additional published studies, as well as raw data provided by the study authors.4
In this systematic review and meta-analysis, we examined the efficacy of cooling therapy in improving neurological outcomes after mild NE.
Methods
We used the Cochrane methodology for the review. Three investigators (UK/JT/ST) searched the MEDLINE, Cochrane database, Scopus and ISI Web of Knowledge databases (1995–2018) using the keywords ‘hypoxic ischemic encephalopathy’, ‘newborn’ and ‘hypothermia’ and clinical trials as study type.
All randomised controlled trial (RCT) and quasi-randomised controlled clinical trials comparing selective head or whole-body cooling with usual care in term or near-term infants (≥36 weeks) with mild NE after perinatal asphyxia were eligible. Perinatal asphyxia required at least one of the following criteria: evidence of intrapartum catastrophe, fetal or neonatal metabolic acidosis and/or resuscitation at birth. Mild NE was not defined separately but was based on a clinical neurological examination performed within 6 hours of birth, as reported in the individual studies. Primary outcome was the composite of death or moderate or severe disability at or beyond 18 months of age.
Three authors (UK/RP/TM) independently extracted the raw data from the full text or supplementary information of the eligible studies. Additional data were obtained from the corresponding authors. Two assessors (NL/RP) independently examined the study quality using the Cochrane Risk of Bias Tool (https://methods.cochrane.org/bias/resources/cochrane-risk-bias-tool) (online supplementary eTable 1). We used a fixed effects model for meta-analysis (RevMan V.5.1.4).
Supplemental material
Results
We identified 91 papers on initial screening, of which 14 RCTs met the inclusion criteria. Seven included mild NE, of which outcome data were available from five (online supplementary eFigure 1).
Supplemental material
The inclusion criteria for participants in the studies were similar and primarily based on a modified Sarnat clinical encephalopathy examination. Thayyil et al used the Thompson encephalopathy score,5 while Gluckman et al (Coolcap Trial) required abnormal amplitude integrated electroencephalography (aEEG) in addition to the clinical neurological examination.6 Hence, the Coolcap Trial6 included eight babies with mild NE of whom five had moderate aEEG voltage abnormalities and three had severe voltage abnormalities.
Two studies used whole-body cooling and three used selective head cooling. The cooling devices used in these studies were ice packs (n=1) and phase change material (n=1) for the whole-body cooling group (target core temperature 33.0°C–34.0°C) and cooling caps (n=3) for the selective cooling group (target core temperature 34.5°C–35.0°C) (table 1).
Details of studies meeting the eligibility criteria
All except one study was of fair quality (online supplementary eTable 1). Infants in the control group were cared for under overhead radiant warmers, which were servo-controlled to the infant’s abdominal skin temperature to maintain normothermia, although the individual temperature profiles were not available. Infants in both groups received similar clinical care, monitoring of vital signs and surveillance for organ dysfunction, irrespective of the intervention.
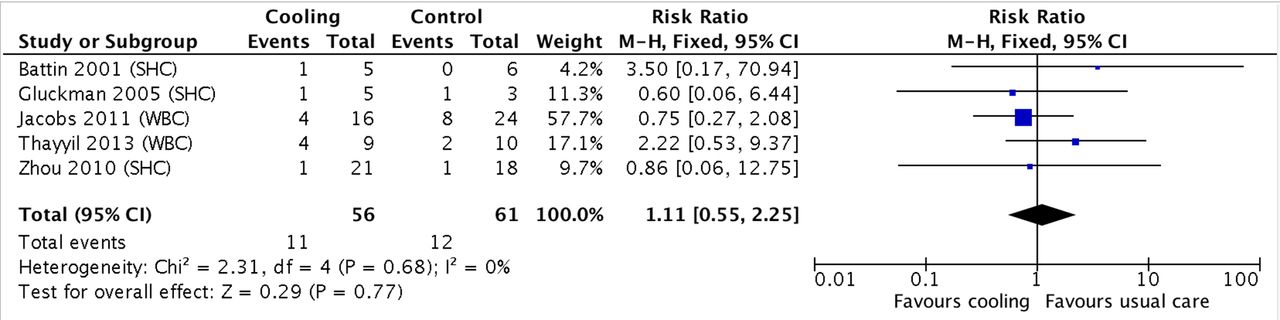
Primary outcome (death or moderate or severe disability at ≥18 months of age) was available from 117 of 133 babies (table 1) for meta-analysis (56 cooled vs 61 non-cooled). Pooled data did not show any significant difference in the adverse outcomes between the two groups (11/56 (19.6%) of the cooled babies and 12/61 (19.7%) of the usual care babies (risk ratio (RR) 1.11 (95% CIs 0.55 to 2.25). No statistical heterogeneity was observed on meta-analysis (χ2=2.31; p=0.68) (figure 1). The data on other short-term morbidities were not available.
{kind=link}
Effect of cooling on death or moderate or severe disability after mild encephalopathy. SHC, selective head cooling; WBC, whole body cooling.
Discussion
The pooled data, including a total of 117 babies with mild NE, did not show a reduction in adverse outcomes (RR 1.12, 95% CI 0.42 to 2.98). However, the CIs were wide, suggesting that a significant benefit or harm from cooling therapy cannot be excluded. The observation of adverse outcomes in 20% of the babies (in both usual care and cooled groups) confirms the emerging concerns about the ‘non-benign’ nature of mild NE.
It is possible that the underlying mechanism of brain injury after moderate or severe NE may be different to that after mild NE and so the therapeutic efficacy of hypothermia cannot be taken for granted in this population. For example, secondary energy failure is seen in preclinical models of moderate or severe NE, which is prevented by therapeutic hypothermia,7 and this is not thought to be a feature of mild NE. Furthermore, most investigators have reported that the patterns of brain injury in mild NE are different to those of moderate or severe NE, indicating the underlying mechanisms may be different.8
The number of babies with adverse outcomes, and the total number of studies included in our meta-analyses is different to that of Conway et al.4 However, it did not affect the overall pooled data. As the raw data were not available from some of the published papers, we obtained these from the corresponding authors, which may explain these differences.
Our systematic review has some limitations. Although the included trials were of high quality, they were designed to recruit only babies with moderate or severe NE, and the babies with mild NE were inadvertently recruited. Therefore, it is possible that these babies had additional or alternative pathologies, for example, stroke, and hence may not be representative of the typical mild NE population. Second, there is no uniformly accepted definition of mild NE, particularly when the diagnosis is made within 6 hours of birth, and it is likely that criteria varied within the individual trials. This may explain the surprisingly high event rates (death or moderate or severe disability) and the lack of treatment effect of hypothermic neuroprotection in our meta-analysis.
Data from studies that included babies with mild NE have variable results. In a prospective study of 63 non-cooled babies with mild NE on modified Sarnat examination performed within 6 hours of birth, Chalak et al reported adverse outcome at 18–22 months in 16% of babies.9 Only one baby with mild NE developed seizures after 6 hours of age and progressed to moderate NE.9 In contrast, Lally et al found no adverse outcome in cooled mild NE babies recruited to the Magnetic Resonance Biomarkers in Neonatal Encephalopathy study.10 In the secondary analysis of this study, cooling babies with mild NE was associated with improved magnetic resonance spectroscopy biomarkers.11 Well designed and adequately powered RCTs are needed to address the risks, benefits and efficacy of therapeutic hypothermia in mild NE.
Conclusion
Although up to 20% of babies with mild NE may have the adverse outcome of death or moderate or severe disability at 18 months of age, current evidence is insufficient to recommend routine therapeutic hypothermia for this condition. Our meta-analysis suggests that significant benefits or harm of therapeutic hypothermia in mild NE cannot be excluded. Therapeutic hypothermia in mild NE should not be considered as the standard of care until further evidence from adequately powered clinical trials is available.
References
Footnotes
Contributors UK searched the literature, extracted the data and drafted the manuscript along with PM and PJL. RP and TM extracted the data and examined the study quality with NL. JT searched the literature. VO, AS and SS interpreted the data and assisted in developing the manuscript. ST conceived the idea, performed the meta-analysis and supervised the entire work.
Funding PM is funded by an MRC doctoral fellowship, VO by an NIHR doctoral fellowship and PJL by an NIHR clinical trials fellowship. This research was supported by the NIHR Biomedical Research Centre based at Imperial College London.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.
Linked Articles
- Fantoms