Article Text

Abstract
Introduction Preterm infants with inadequate breathing receive positive pressure ventilation (PPV) by mask with variable success. The authors examined recordings of PPV given to preterm infants in the delivery room for prevalence of mask leak and airway obstruction.
Methods and patients The authors reviewed recordings of infants at <32 weeks' gestation born between February 2006 and March 2009. PPV was delivered with a T-piece or self-inflating bag and a round silicone face mask. Airway pressures and gas flow were recorded with a respiratory function monitor (RFM). Videos recorded from a web camera were used to review the resuscitation. The first 2 min of PPV were analysed for each infant. Obstruction was arbitrarily defined as a 75% reduction in delivered expired tidal volume (VTe) and significant face-mask leak as >75%.
Results The authors analysed recordings of 56 preterm infants. Obstruction occurred in 14 (26%) recordings and leaks in 27 (51%). Both obstruction and mask leaks were seen in eight (14%) recordings, and neither was seen in 15 (27%). Obstruction occurred at a median (IQR) of 48 (24–60) s after the start of PPV. A median (range) of 22 (3–83) consecutive obstructed inflations were delivered. Face-mask leaks occurred from the first inflation in 19/27 (70%) and in the remaining eight at a median (IQR) of 30 (24–46) s after the start of PPV. A median (range) of 10 (3–117) consecutive inflations with a leak >75% were delivered.
Conclusion Airway obstruction and face-mask leak are common during the first 2 min of PPV. An RFM enables detection of important airway obstruction and mask leak.
Statistics from Altmetric.com
Introduction
When preterm infants fail to breathe adequately immediately after birth, it is important to apply positive pressure ventilation (PPV) to create a functional residual capacity, facilitate gas exchange and initiate spontaneous breathing.1 2 However, the delivery of adequate PPV in the delivery room (DR) is dependent on a good face-mask technique. Guidelines suggest that the effectiveness of PPV should be gauged by the presence of increasing heart rate (HR) and adequate chest rise.3 Several factors can reduce the effectiveness of PPV. These include a poor face-mask technique resulting in a leak or airway obstruction, spontaneous movements of the baby, movements by or distraction of the resuscitator, and procedures such as changing the wraps or fitting a hat.4,–,7
What is already known on this topic
▶ Mask leak is common during ventilation in the delivery room.
▶ Assessment of airway obstruction during mask ventilation with a CO2 detector has been described.
▶ Respiratory function monitors (RFMs) are routinely used in intensive care units to monitor and target tidal volume.
What this study adds
▶ A mask leak and airway obstruction are common during mask ventilation.
▶ An RFM can be used to recognise and correct these problems.
Manikin studies have shown that face-mask leak varies widely during PPV.6,–,9 An observational study in the DR reported similar results10 where resuscitators had a median (range) mask leak of 29% (0–100%). Most resuscitators were unaware of the extent of their mask leak.10 Another cause of inadequate PPV is airway obstruction. Finer et al4 recently reported airway obstruction during PPV using a colorimetric carbon dioxide (CO2) detector. They found airway obstruction in 75% of infants receiving PPV in the DR.4 A CO2 detector is a very useful device to assess effective ventilation; however, it cannot differentiate between an inadequate tidal volume and airway obstruction.11 In comparison, a respiratory function monitor (RFM) displays flow and tidal volume signals allowing the characteristic pattern associated with mask leak and airway obstruction to be identified.12 The contribution of an ineffective technique to failure of neonatal resuscitation is unknown. We reviewed recordings of neonatal resuscitation in order to determine the frequency of face-mask leak and obstruction.
Patients and methods
This study was carried out between February 2006 and March 2009 at The Royal Women's Hospital, Melbourne, a tertiary perinatal centre admitting more than 100 infants with a birth weight of <1000 g to the neonatal nursery annually. During this period, if the research team were available, they attended deliveries in addition to the resuscitation team (usually a nurse, paediatric resident, fellow and consultant). The research team were not involved in the clinical care of the infants. The study was approved by The Royal Women's Hospital Research, and Ethics Committees and parental consent to use the recordings was obtained.
Infants who clinicians judged to have inadequate breathing were given PPV with either a T-piece device (Neopuff Infant Resuscitator, Fisher & Paykel Healthcare, Auckland, New Zealand) or a 240 ml self-inflating bag and attached gas reservoir (Laerdal, Stavanger, Norway). The Neopuff is a continuous flow, pressure-limited device with a manometer and a positive end-expiratory pressure (PEEP) valve. The default settings were a gas flow of 8 l/min, peak inflation pressure of 30 cm H2O and PEEP of 5 cm H2O. The self-inflating bag was used with 8 l/min gas flow and without a manometer or a PEEP valve.
Infants reviewed between February 2007 and February 2009 were included in a randomised control trial comparing PEEP with no PEEP during PPV in the first 5 min after birth. These infants were randomised to receive PPV with either a Neopuff or a Laerdal bag.
Staff members attending deliveries were trained to use both devices. A size 00 round silicone face mask (Laerdal, Stavanger, Norway) was used with both devices. Resuscitation was started with air for all infants. Clinicians could change to 100% oxygen if they felt the infant was not responding to initial resuscitation.
A Florian RFM (Acutronic Medical Systems AG, Zug, Switzerland) was used to measure airway pressures and gas flow. Airway pressure was measured directly from the circuit. A hot-wire anemometer flow sensor placed between the ventilation device and the face mask measured gas flow. The RFM automatically calculated the tidal volume passing through the sensor by integrating the flow signal. The gas flow, tidal volumes and airway pressure were recorded at 200 Hz using a dedicated computer with Spectra software (Grove Medical, London), a program specifically designed for recording neonatal physiological data. In the DR, neither the RFM nor the computer screen was visible to the resuscitators, and the monitor's alarm was disabled. However, mask leak and airway obstruction were communicated to the clinical team. A webcam recorded the resuscitation at 5 frames/s. A Masimo Radical pulse oximeter (Masimo Corporation, Irvine, California) probe set at maximum sensitivity and 2 s averaging was placed around the infant's right wrist to measure oxygen saturation (Spo2) and HR.13 14 A decrease of >15% for Spo2 or >15 bpm for HR was considered to be clinically important.
Two researchers (JAD and GMS) reviewed RFM and video recordings to identify infants who received PPV in the DR. Each RFM recording was analysed for 2 min from the first inflation. The videos were used to identify when the mask was repositioned.
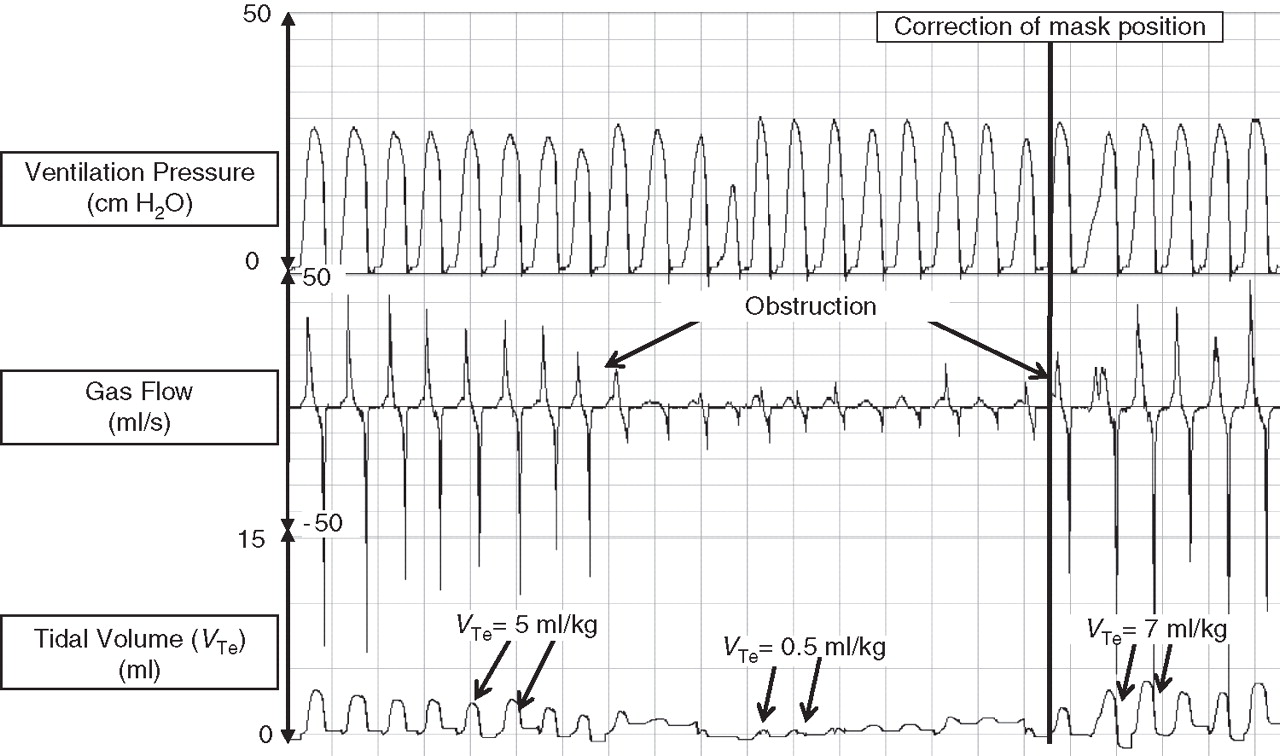
Airway obstruction
Clinically significant airway obstruction was arbitrarily defined as either a 75% reduction in expired tidal volume (VTe) compared with the baseline of 10 inflations prior to the obstructed inflation (see figure 1) or a 75% increase in VTe after correction for obstruction. Obstruction was characterised by a similar reduction in both inspired and expired tidal volumes.
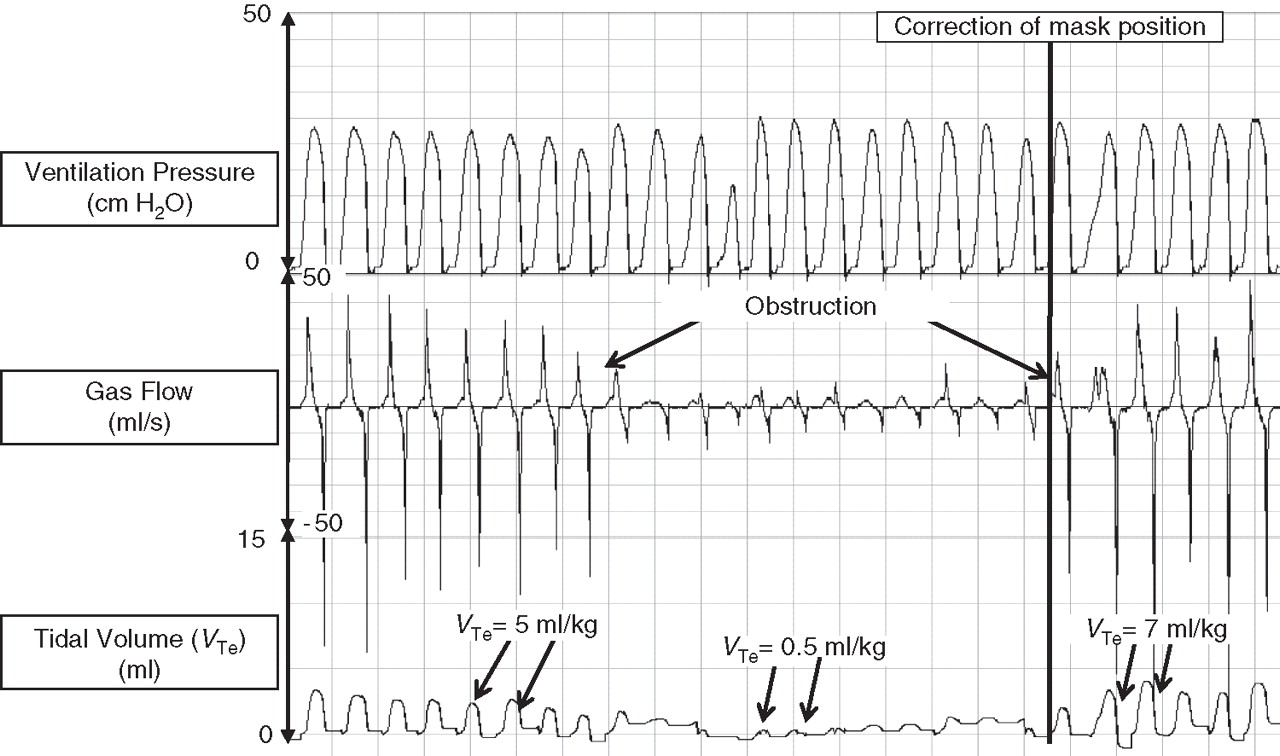
Airway obstruction during mask positive pressure ventilation (PPV) in a very preterm infant with a self-inflating bag. Initially, PPV delivered an expired tidal volume (VTe) of 5 ml/kg. Both inflation and expiratory flow waves rapidly reduced in size. This is reflected in the VT curve, which displays a 90% reduction in VTe. By correcting the face-mask position, the tidal volume is restored. Throughout PPV, the peak inflation pressure is achieved.
Face-mask leak
The leak from the mask was calculated by expressing the volume of gas that did not return through the flow sensor at the end of inflation as a percentage of the volume that passed through the flow sensor during inflation (leak (%)=((inspired tidal volume–VTe)/inspired tidal volume)×100) (see figure 2).6 We considered a mask leak of >75% as clinically important.

{kind=link}
{kind=link}
Large leak at the mask in a very preterm infant ventilated with a self-inflating bag. After inflation 4, for about 4 s the inspiratory flow curve suddenly shows just the gas flow towards the face mask and no expiratory flow. This demonstrates a very large leak around the face mask. The tidal volume curve shows a large flow of gas out of the face mask but little gas returning, indicating about a leak of about 80–100%. After correcting the face-mask position, there is a reduction in the face-mask leak to 15%, with adequate gas flow entering and leaving the lung. VTe, expired tidal volume; VTi, inspired tidal volume.
Statistical analysis
A breath by breath analysis of pressure, flow and tidal volume was performed and the tidal volume and mask leak for each inflation were measured. The face-mask leak was corrected for body temperature, pressure and water vapour saturation using a standardised equation.15 Results are presented as mean (SD) for normally distributed continuous variables and median (IQR) or range for variables with a skewed distribution. Data were analysed using STATA version 10 (Stata Corp, College Station, Texas, US).
Results
Of the 106 resuscitations recorded, 56 (53%) infants received PPV while 50 (47%) infants received CPAP only. Twenty-five (45%) were ventilated with a T-piece-device and 31 (55%) with a self-inflating bag. Infant demographics are shown in table 1. A total of 4048 inflations were analysed, with a median (IQR) of 76 (53–98) per infant. PPV started at a median (range) of 82 (33–125) s after birth.
Infant demographics (n = 56)
Inflations showing airway obstruction and mask leak were identified in 14/56 (25%) and 27/56 (48%) of the recordings respectively. In 8/56 resuscitations both obstruction and mask leak occurred and in 15/56 neither occurred. None of the infants received cardiac compressions or epinephrine.
Airway obstruction
In 14 (25%) infants (six with a T-piece and 8 with a self-inflating bag) airway obstruction was identified. The median (IQR) time of obstruction was 48 (24–60) s after start of PPV. In two infants airway obstruction occurred from the first inflation. A median (range) of 22 (3–83) consecutive obstructed inflations were identified. The median (IQR) delivered VTe during airway obstruction was 0.6 (0.2–1.2) ml/kg compared with 7.2 (4.9–8.9) ml/kg during unobstructed PPV. To improve ventilation the resuscitator either repositioned face mask (n=8), changed mask hold (n=3), repositioned the head (n=2) or was replaced by another resuscitator (n=1). Airway obstruction reoccurred after initial correction in three cases, where changing mask hold (n=1), replaced by another resuscitator (n=1) or increased airway pressure (n=1) was used. In seven cases (50%) the inspired oxygen was increased from 21% to 100% during obstruction. Six of these seven infants were intubated because of poor response to ventilation.
During five resuscitations, obstruction occurred before Spo2 or HR was recorded. In one recording only three obstructed inflations were delivered and no changes in Spo2 and HR were observed. In three recordings Spo2 decreased by >15% and in six recordings HR decreased by >15 beats per minute (bpm) during obstruction.
Face-mask leak
A T-piece was used in 13 and the self-inflating bag in 14 infants where a mask leak >75% was identified. This occurred in 19 (70%) infants as soon as PPV was started. In the remaining eight (30%) infants, a mask leak occurred later, at a median (range) time of 30 (13–69) s after the start of PPV. A median (range) of 10 (3–117) consecutive inflations with a large mask leak were delivered. The median (IQR) expiratory tidal volume during large face-mask leaks was 5.6 (2.4–11.5) ml/kg. Different measures were taken to improve ventilation: repositioned face mask (n=23), changed mask hold (n=7), repositioned the head (n=2) or replacement by another resuscitator (n=1). In some cases, several measures were taken. In no case was the inflating pressure increased. Three infants were intubated. In six cases, a mask leak reoccurred after initial correction, and in three of them a face-mask leak reoccurred after the second correction. In three cases, the inspired oxygen was increased from 21% to 100% during PPV.
During six resuscitations, a mask leak occurred before Spo2 or HR was recorded. In 15 infants, no changes in Spo2 or HR were observed. In one infant, a mask leak was followed by obstruction, and so Spo2 and HR were not analysed. In five, either Spo2 decreased by >15% or HR decreased by >15 bpm during a mask leak.
Discussion
We recently reported that an RFM can be used to guide clinicians during PPV in the DR.12 Several factors prevent effective ventilation, including obstruction (pressing the mask onto the infant's face too tightly, flexing or overextending the neck) or leak resulting from holding the mask incorrectly.4 6 8 11 16
In this study, we have shown that both significant airway obstruction and face-mask leaks occur during the first 2 min in about half of the very preterm infants who received PPV in the DR. Although we observed both obstruction and leak in eight (15%) recordings, in general, a large mask leak was observed in twice as many recordings as airway obstruction. In about a third, neither obstruction nor a face-mask leak occurred. A mask leak was more likely to occur at the start of PPV, while airway obstruction occurred more often later on. A recent manikin study by Schilleman et al16 showed that operators had frequent airway obstruction once they had adjusted mask hold to correct for a leak. However, we did not find this in our observations.
Assessment of the infant may distract the resuscitators' focus from the mask position and mask-holding techniques during the initial phase of PPV. We observed that procedures such as fitting a hat or putting the infant in a plastic bag contributed to a large face-mask leak. Once PPV was established, a leak was less likely to be observed. In the current study, a round silicone face-mask, size 00 (Laerdal, Stavanger, Norway), was used. These results might vary with different face masks. The rate of intubation was four times higher in infants with an airway obstruction (43%) than those with a mask leak (11%). This suggests that airway obstruction is more likely to cause major clinical deterioration.
Conventional resuscitation training states that airway obstruction may be due to manual compression of the soft tissues of the neck and thus the trachea, or hyperextension or flexion of the head.17 However, after examining many recordings, we think most obstruction is due to the face mask being held on the face so tightly that it obstructs the mouth and nose. We believe this was the case, because the obstruction was resolved by reapplying the face mask, rather than altering the head position. However, we cannot be sure that neck obstruction is not occurring in some infants.
Both, manikin and observational studies in the DR have shown that mask leaks are common.6 8 10 16 However, none have reported a close relationship between percentage mask leak and delivered tidal volume. Arbitrarily defining a mask leak of >75% clinical significant is one limitation of this study. We chose this because we hypothesised that such a large leak might lead to a failure in tidal volume delivery and an increase in adverse events. However, we noted that in spite of a large mask leak, adequate tidal volumes continued to be delivered. Only a minority of infants with a large leak experienced a clinical deterioration.
Possible role of a respiratory function monitor in the delivery room
Reports suggest that an RFM may be useful in the DR to measure and carefully adjust respiratory support.10 18,–,22 In particular, an RFM may help avoid volutrauma and over-ventilation by enabling clinicians to achieve a desired target tidal volume.18 In addition, we have shown that it can be used to detect inadequate ventilation by observing tidal volume waves.12
Limitations
There are several limitations of this technology. Inexperience and lack of knowledge about the displayed waveforms may lead to misinterpretation of the signals. Therefore, anyone using an RFM must be trained to interpret pressure, flow and tidal volume signals. In addition, the attention of an inexperienced user may be diverted from the infant to the monitor.12
Conclusion
During DR mask ventilation in very preterm infants, significant airway obstruction or a large mask leak frequently occurred during the first 2 min of PPV. An RFM can help identify both causes of failure of PPV by displaying gas flow, and tidal volume and pressure waves.
References
Footnotes
-
Funding JAD, COFK, CPFOD and GMS are recipients of a Royal Women's Hospital Postgraduate Research Degree Scholarship. GMS is supported in part by a Monash International Postgraduate Research Scholarship. PGD is supported in part by an Australian National Health and Medical Research Council Practitioner Fellowship. PGD and CJM hold an Australian National Health and Medical Research Council Program Grant No 384100.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by The Royal Women's Hospital.
-
Patient consent Obtained from the parents.