Article Text

Abstract
Objective To evaluate the effect of oral Lactobacillus reuteri (L reuteri) first on the incidence and severity of Necrotising enterocolitis (NEC) and second on sepsis.
Design Prospective randomised controlled study.
Setting Tertiary neonatal intensive care unit.
Patients and interventions Preterm infants with a gestational age of ≤32 weeks and a birth weight of ≤1500 g were included (n=400). Infants in the first group were given 100 million CFU/day (5 drops) of lyophilised L reuteri (DSM 17938) mixed in breast milk or formula, starting from first feeding until discharge. Participants in the control group were given a placebo.
Main outcome measures To determine and compare the frequency of NEC and/or death after 7 days, frequency of proven sepsis, rates of feeding intolerance and duration of hospital stay.
Results There was no statistically significant difference between groups in terms of frequency of NEC stage ≥2 (4% vs 5%; p=0.63) or overall NEC or mortality rates (10% vs 13.5%; p=0.27). Frequency of proven sepsis was significantly lower in the probiotic group compared to the control group (6.5% vs 12.5%; p=0.041). A significant difference was also observed with regard to rates of feeding intolerance (28% vs 39.5%; p=0.015) and duration of hospital stay (38 (10–131) vs 46 (10–180) days; p=0.022).
Conclusions Our results show that oral L reuteri does not seem to affect the overall rates of NEC and/or death in preterm infants followed up in the neonatal intensive care unit, and significant reductions were observed in the frequency of proven sepsis, rates of feeding intolerance and duration of hospital stay.
Trial registration number NCT01531179.
- Feeding intolerance
- lactobacillus reuteri
- necrotizing enterocolitis
- preterm infant
Statistics from Altmetric.com
What is already known
-
Necrotising enterocolitis (NEC) is an important cause of morbidity and mortality in preterm infants. Results on the benefits of probiotics in reducing the frequency of NEC are conflicting.
What this study adds
-
Lactobacillus reuteri reduces rates of proven sepsis, feeding intolerance and duration of hospital stay.
-
L reuteri does not seem to affect the overall rates of NEC and/or death.
Introduction
Necrotising enterocolitis (NEC) is the most frequently encountered acquired intra-abdominal emergency in preterm infants, the risk of which is inversely related to gestational age and birth weight.1 More than 85% of all NEC cases occur in very low birthweight (VLBW) infants. The estimated prevalence of NEC among VLBW infants based on the results of multicentre and large population-based studies is between 7% and 11%.2 ,3 Key contributors to NEC include intestinal immaturity and formula feeding, while an exaggerated inflammatory response within the intestinal epithelial barrier to luminal microbes has also been implicated.4 Despite recent advances in neonatal care, NEC remains a leading cause of morbidity and mortality in neonatal intensive care units (NICU).1 ,5
Probiotics, which are live microorganisms that colonise the gut, have been shown to have a protective effect against NEC via upregulation of local and systemic immunity leading to an increase in anti-inflammatory cytokines. They have also been reported to provide barrier to bacterial migration along with their products across the mucosa, competitive exclusion of potential pathogens, modification of host response to microbial products, augmentation of IgA mucosal responses, enhancement of enteral nutrition that inhibit the growth of pathogens and upregulation of immune responses.6–11 Conflicting reports regarding the effects of probiotics on the incidence of NEC may be encountered in the literature. While some studies have demonstrated a significant reduction in the frequency of NEC in VLBW infants with the use of probiotics containing Bifidobacterium and Lactobacillus species,12 ,13 a similar benefit was not observed in other studies.14 Probiotics have been also shown to be associated with significant reduction in feeding intolerance and duration of hospital stay.5 The recent Cochrane meta-analysis showed that there was no evidence of significant reduction in nosocomial sepsis by probiotic use in the NICU.5
The aim of this study was to evaluate the effect of prophylactic administration of Lactobacillus reuteri (L reuteri) to preterm infants. Primary endpoints were development of NEC or death, whereas secondary endpoints included sepsis, feeding intolerance, full feeding day and duration of hospital stay. L reuteri, which is naturally found in humans, was preferred for the purposes of this study, taking into account the evidence supporting its role as a protective microorganism with immunomodulatory and bactericidal properties.15–17 Although Cochrane meta-analysis has conclusion on probiotic use in prevention of NEC and sepsis, there has been still lack of data on this specific species.
Methods
Patient selection
This prospective, double-blinded, randomised, placebo-controlled trial was conducted in the NICU of Zekai Tahir Burak Maternity Teaching Hospital, Ankara, Turkey between February 2012 and February 2013. This unit has 150 incubators and serves as a referral Level III NICU, with approximately 4000 newborn admissions per year. This trial was approved by the local ethics committee, and infants were enrolled in the study after written parental consent was obtained. The trial was registered to ClinicalTrials.gov under identifier NCT01531179 (http://clinicaltrials.gov/ct2/show/NCT01531179).
Preterm infants with a gestational age ≤32 weeks and birth weight ≤1500 g, which survived to feed enterally, were eligible for the study. Criteria for exclusion were major congenital malformations and lack of parental consent.
Randomisation
Study infants were randomly assigned to probiotic or placebo by using sequential numbers generated at the computer centre of the NICU by 1:1 allocation ratio. The allocations were contained in opaque, sequentially numbered sealed envelopes. The pharmacist followed instructions from the sealed envelopes. Both probiotic and placebo doses were prepared in the pharmacy in sterile conditions, packaged in identical vials of an oil-based suspension labelled with an individual number indicating the randomisation sequence and refrigerated until administration.
Product preparation
Probiotic or placebo administration was started with the first feed of the infants. Infants in the probiotic group received five drops of oil-based suspension containing 1×108 colony-forming units of L reuteri DSM 17938 (Biogaia AB, Stockholm, Sweden) once a day, until death or discharge from the hospital. For infants on oral feeds, after suctioning oral secretions, five drops were placed in the posterior oropharynx of the infants. For infants without per oral feeds, five drops were administered through a gastric tube followed by a flash of 0.5 mL of sterile water. For the infants in the placebo group, five drops from an identical vial containing only oil base were administered following the same protocol as the probiotic group.
Primary and secondary outcomes
Primary outcome of present study was death beyond the 7th day of life and/or NEC stage ≥2. Secondary outcomes were culture-proven sepsis, feeding intolerance, time to reach full enteral feeding and duration of hospitalisation. Adverse effects, including culture-proven sepsis attributable to L reuteri, flatulence and diarrhoea were also recorded.
Follow-up
Enteral feeding was started when the infant had stable vital signs, had active bowel sound without abdominal distention and had no bile or blood from the orogastric tube. Feeding consisted of breast milk or premature infant formula (for the infants with insufficient production of mother breast milk) was started at 10–20 mL/kg depending on the gestational age of the infant. The amount of feeding was advanced if tolerated with no more than a 20 mL/kg per day. If there were ≥2 signs of feeding intolerance (gastric residuals in the amount that was more than half of the previous feeding, abdominal distention or heme-positive stools), feeding was stopped and was withheld as long as the signs of feeding intolerance continued. When feeding intolerance recovered, the feeding was restarted according to attending neonatologist’s decision. Infants who weighed <1000 g received total parenteral nutrition (TPN) until half of the calories were supplied by the oral route. Whenever an infant was suspected to have NEC, the infant was evaluated by two senior-attending neonatologists who did not know the group assignment of the infant. Clinical signs and abdominal radiographs were reviewed and NEC was categorised by modified Bell's classification.18 The cases of NEC that had reached Bell's stage 2 or higher were considered. If enteric feeds were stopped because of feeding intolerance or NEC during the hospitalisation, the administration of the probiotic or placebo was also stopped and restarted only when the neonatologist reinstated the enteric feeds. Flatulence was diagnosed as the presence of abdominal distention without tenderness by confirming the distention of bowel loops by the radiographic examination. Diarrhoea was defined as the passage of three or more loose or watery stools per day.
If the infants died within the first week of life, as it was determined that these infants would not have had opportunity to benefit from the probiotic intervention, they were excluded from the analysis.
The main action of Lactobacillus sp. seems to consist in stimulating and in regulating the intestine's host-defence mechanisms which may not occur immediately.19 Therefore, only the cases of NEC or deaths occurring after 7 days of L reuteri supplementation have been taken into account in this study.
Demographic and clinical variables that are risk factors for NEC, including prenatal steroid use, small for gestational age, prolonged rupture of amniotic membranes, chorioamnionitis, asphyxia, ibuprofen use and late-onset (after 3 days postnatal age) sepsis were prospectively recorded. Patients with culture positivity were accepted as having proven sepsis. Two-blood culture positivity was required to confirm Staphylococcus epidermidis sepsis. Routinely, all of the infants received antifungal prophylaxis as nystatin (Micostatin; Bristol-Myers Squibb, Montreal Quebec, Canada) suspension (100 000 U/mL) every 8 h in our NICU according to our antifungal prophylaxis protocol. Duration of mechanical ventilation, antibiotic treatment, parenteral nutrition and hospitalisation (up to discharge to home), umbilical venous catheterisation, type of feeding and age at the beginning of feeding were also recorded.
The event rate for sample size calculation was based on the prestudy incidence of death or NEC (stage ≥2) for VLBW infants in NICU of Zekai Tahir Burak Maternity Teaching Hospital. Our recent event rate for death or NEC (stage ≥2) for VLBW was 15% in our NICU. With the α-error set at 0.05 and the β-error set at 0.2, and a relative reduction in the incidence of NEC or death of 50%, the number needed to verify our hypothesis was 190 infants for each arm.
Statistical analysis
Statistical analyses were performed using the statistical package SPSS for Windows V.17.0 (SPSS Inc, Chicago, Illinois, USA). Independent samples t test were used for continuous variables. The χ2 test was used for categorical variables. In post hoc subgroup analysis, patients were stratified according to birth weight (<1000 g and 1000–1500 g) for the evaluation of primary and secondary outcomes. Continuous variables are presented as the means±SD, while categorical variables are given as frequencies and percentages. In addition to the p value of the primary outcomes, results were given as relative risk (RR) and 95% CIs. A p value of <0.05 was considered statistically significant.
Results
Study participants
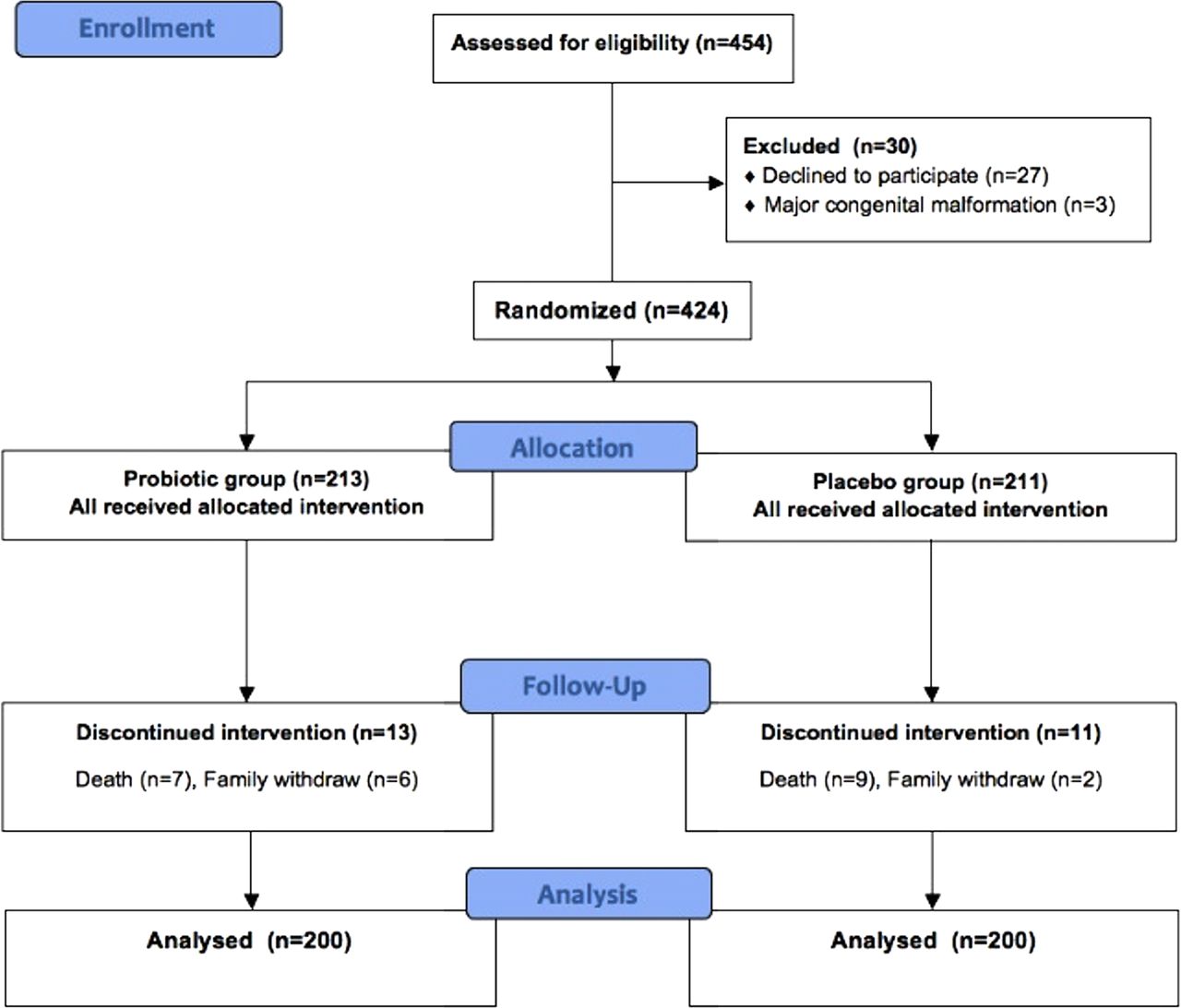
There were 454 VLBW infants admitted to our NICU during the study period. Among these infants, 30 were excluded because of major congenital malformations (n=3) and lack of parental consent (n=27). A total of 424 infants enrolled in the study; 6 infants in probiotic group and 2 infants in placebo group dropped out of the programme because of parent's wish to withdraw the infants from the trial. Seven infants in probiotic group and nine infants in placebo group died because of immaturity, pulmonary and intraventricular haemorrhage within the first week of life and were excluded from the analysis. A total of 400 infants completed the study protocol. There were 200 infants in probiotic group and 200 infants in placebo group. Figure 1 shows the flowchart of the study infants. No significant differences were observed in demographic and clinical characteristics of the study infants (table 1).
Demographic and clinical characteristics of the study infants
{kind=link}
Flow chart of the study.
Primary outcomes
The frequency of death or NEC was similar between the groups (RR 1.4; 95% CI 0.76 to 2.59; p=0.27), as were the frequencies of each of these considered individually (death, RR 1.37; 95% CI 0.68 to 2.76; NEC, RR 1.26; 95% CI 0.48 to 3.27)(tables 2 and 3). In addition, there was no difference between the probiotic and placebo group in the incidence of death attributable to NEC (3 of 200 infants vs 4 of 200 infants; p=0.50). Addition of deaths in first 7 days for intention to treat analysis provided the same results. The primary outcomes did not show any significant difference when were evaluated both for infants with birth weight <1000 g or between 1000 and 1500 g.
Primary outcomes of the study
Primary outcomes according to birth weight
Although the median age at diagnosis of NEC was younger in placebo group compared to probiotic group, there was no significant difference between the groups (19 (14–48) vs 25 (14–41) days, respectively; p=0.47).
Secondary outcomes
The frequency of culture-proven sepsis was significantly lower in probiotic group when compared to placebo group (RR 2.05; 95% CI 1.01 to 4.14; p=0.041) (table 4). The aetiology in culture-positive septic infants were Gram-positive pathogens in 53% (n=20) of cases (probiotic group (n=6, 46.1%) vs placebo group (n=14, 56%)), Gram-negative pathogens in 37% (n=14) of cases (probiotic group (n=6, 46.1%) vs placebo group (n=8, 32%)) and fungi in 10% (n=4) of cases (probiotic group (n=1, 7.7%) vs placebo group (n=3, 12%)). There were no significant differences for pathogen distribution between probiotic and placebo groups. None of the positive blood cultures grew L reuteri. No other adverse events attributed to L reuteri administration were noted in any of the infants included in the analysis.
Secondary outcomes of the study
Feeding intolerance was significantly lower in infants exposed to probiotic when compared to placebo-exposed infants (28% vs 39.5%; p=0.015). Feeding intolerance periods of the infants in both groups were less than 72 h, and only 16 (8%) infants in probiotics group and 22 (11%) infants in the placebo group had more than two episodes of feeding intolerance. Time to reach full enteral feeding was also significantly decreased in probiotic group when compared with placebo group (9.1±3.2 vs 10.1±4.3; p=0.006, respectively).
Duration of hospitalisation was significantly lower in infants exposed to probiotic when compared to placebo-exposed infants (38 (10–131) vs 46 (10–180) days; p=0.022). When the secondary outcomes were evaluated according to defined birthweight groups, all of them showed significant differences in infants with birth weight <1000 g. However, only significant difference observed in infants with birth weight between 1000 and 1500 g was in duration of hospitalisation.
Discussion
Our present study was a randomised controlled study investigating the efficacy of orally administered L reuteri in reducing the incidence and severity of NEC in VLBW infants. Our results showed that supplementation with L reuteri resulted in significant reductions in the frequency of proven sepsis, rates of feeding intolerance and duration of hospital stay, but no significant difference was observed in terms of overall rate of NEC/death.
Conflicting results have been reported in previous studies regarding the effects of probiotics on these outcomes.12–14 ,20 ,21 A recent Cochrane meta-analysis by Alfaleh et al,5 published in 2011, supported a favourable effect of probiotics on NEC. Probiotics were associated with a reduced frequency of stage II and III NEC with a RR of 0.35 (95% CI 0.24 to 052). The RR in a subgroup of infants with a birth weight <1500 g was (95% CI 0.23 to 0.50), while data on patients weighing <1000 g were deemed insufficient for analysis. Based on the results of 10 studies evaluating the effect of probiotics on mortality rates of premature infants, authors reported a RR of 0.40 (95% CI 0.27 to 0.60). A significant reduction was also observed in terms of NEC-related mortality (RR 0.31, 95% CI 0.10 to 0.94), although no difference was reported with regard to frequency of sepsis (RR 0.90, 95% CI 0.76 to 1.07). Duration of TPN was significantly shorter in two studies, while the time to enteral feeding was also significantly reduced in three studies.5
Cochrane meta-analysis included all probiotic species used in the literature, which may be thought as the major limitation to conclude on specific species. When L reuteri is discussed, only Rojas et al22 have evaluated the effect of its (DSM 17938) supplementation, in comparison with a placebo, in a cohort of 750 infants with a birth weight <2000 g. Rate of nosocomial infections was lower, albeit insignificantly, in the probiotic group compared to the control group (2.4% vs 5.0%; p=0.06). No significant reduction in the frequency of NEC or mortality rate was reported, although fewer rates of feeding intolerance and shorter durations of hospital stay were observed in the probiotic group, particularly in infants with a birth weight <1500 g.
Our study focused on patients with birth weight below 1500 g. However, we could not find significant difference in NEC and/or death between the probiotic and placebo groups. The use of a single probiotics agent rather than two agents as used in the literature and utility of a relatively low dose of L reuteri may explain, at least in part, the lower treatment effect in our study. Furthermore, similar to the study by Rojas et al,22 we observed fewer episodes of feeding intolerance and duration of hospital stay in the probiotic group compared to the control group. It is suggested that the mechanisms of improved feeding tolerance may be the regulation of intestinal motility, stimulation of intestinal mucosal lactase activity and lowering the intestinal pH.23 We think that L reuteri might shorten the duration of hospital stay by improving gastrointestinal motility and feeding intolerance. Additionally, the main effect of orally administered L reuteri is in the gastrointestinal tract and changing the intestinal microflora by L reuteri could also play role in the prevention of sepsis in our study.
Little is known about use and efficiency of probiotics in infants with a birth weight <1000 g. In a randomised controlled study by Al-Hosni et al,24 50 infants who received probiotics (L. rhamnosus GG and Bifidobacterium infantis) and 51 control infants with a birth weight <1000 g were compared, and they reported that incidences of NEC, death and sepsis were similar between the two groups. In a retrospective cohort study by Hunter et al,25 who reviewed medical records of 311 neonates (79 on L reuteri prohylaxis) with a birth weight <1000 g, reported that the incidence of NEC was significantly lower in the neonates who received L reuteri (15.1% vs 2.5%, p=0.0475). Rate of late-onset sepsis was not statistically different between treated and untreated groups. Limitations of this study were to have a retrospective design and a small group who received L reuteri. A subgroup analysis in our study on infants weighing <1000 g (probiotic, n=93 vs placebo, n=103) failed to demonstrate a significant benefit of L reuteri in terms of frequency of NEC, mortality or deaths attributable to NEC. However, we observed a significant reduction in the rate of proven sepsis with probiotic use, particularly in the <1000 g group. Similar to the Cochrane report,5 we also managed to demonstrate statistically significant reductions in TPN duration, time to enteral feeding and duration of hospital stay.
Our study has a few limitations. First, our study was conducted in a single-centre study. Second, we could not do separate randomisation for subgroup in <1000 g, so the number of patients in the subgroup analysis were not equal. Also, the study was not powered to evaluate NEC/death in this subgroup. Third, we could not perform random stool testing to confirm the presence of colonisation.
Conclusions
This study is the largest one to evaluate the efficacy of L reuteri in preventing NEC in preterm infants with a birth weight <1500 g. Although our results show that oral L reuteri does not seem to affect the overall rates of NEC and/or death in preterm infants followed up in the NICU, significant reductions were observed in the frequency of proven sepsis, rates of feeding intolerance and duration of hospital stay.
Acknowledgments
We are grateful to Sevilay Karahan, PhD, Department of Biostatistics, Hacettepe University for her help in the statistical analysis.
References
Footnotes
-
Contributors MYO and OE: designed research; MYO, FNS, SA, NG, NU and SSO: conducted research and followed by patients. MYO and OE: wrote the paper. UD: had primary responsibility for final content. All authors designed, supervised and analysed the study, and prepared the manuscript. All authors read and approved the final manuscript.
-
Competing interests None.
-
Ethics approval Zekai Tahir Burak Local Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms