Article Text

Abstract
Objectives To prospectively determine the nature and rate of adverse drug reactions (ADRs) in children on antiepileptic drugs (AEDs) and to prospectively evaluate the effect of AEDs on behaviour.
Setting A single centre prospective observational study.
Participants Children (<18 years old) receiving one or more AEDs for epilepsy, at each clinically determined follow-up visit.
Primary and secondary outcomes Primary outcome was adverse reactions of AEDs. Behavioural and cognitive functions were secondary outcomes.
Results 180 children were recruited. Sodium valproate and carbamazepine were the most frequently used AEDs. A total of 114 ADRs were recorded in 56 of these children (31%). 135 children (75%) were on monotherapy. 27 of the 45 children (60%) on polytherapy had ADRs; while 29 (21%) of those on monotherapy had ADRs. The risk of ADRs was significantly lower in patients receiving monotherapy than polytherapy (RR: 0.61, 95% CI 0.47 to 0.79, p<0.0001). Behavioural problems and somnolence were the most common ADRs. 23 children had to discontinue their AED due to an ADR.
Conclusions Behavioural problems and somnolence were the most common ADRs. Polytherapy significantly increases the likelihood of ADRs in children.
Trail registration number EudraCT (2007-000565-37).
- CLINICAL PHARMACOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A prospective study of adverse drug reactions to all antiepileptic drugs used in a single centre.
Cognition and behaviour were assessed using standardised tools.
The planned sample size was not reached.
Both monotherapy and polytherapy were assessed for drug toxicity.
Introduction
Adverse drug reactions (ADRs) are a major clinical problem in both paediatric and adult medicine. Systematic reviews and meta-analyses of prospective studies of drug surveillance in children have showed that one in 10 children in hospital will experience an ADR.1 ,2 Studies in the community suggest that at least one in every 500 children will experience an ADR each year.3 The actual number is likely to be greater than this as the majority of ADRs are unrecognised and unreported.
In 1988, it was identified that the majority of children who receive an antiepileptic drug (AED) as an outpatient will experience an ADR.4 Since then, however, a significant number of newer AEDs have been introduced, each with their own new ADR profile. In a large study of fatal suspected ADRs in the UK, AEDs were the group of medicines most likely to be associated with a fatality.5 Studies in the USA have also suggested that AEDs are associated with a significant number of ADRs.6 There are significant ADRs in association with the newer AEDs.7 Additionally, the reporting of drug toxicity in clinical trials of AEDs is poor.8
Children with epilepsy have a higher incidence of behavioural problems than other children.9 Moreover, both old and new generation AEDs have cognitive and behavioural effects, which can be positive or negative. The cognitive and behavioural effects of AEDs have been previously described.10–12 However, these psychotropic effects are difficult to ascertain because the presence of seizure itself could alter mood and behaviour.13
The aims of the study were to prospectively determine the nature and rate of ADRs in children on AEDs and to prospectively evaluate the effect of AEDs on behaviour and cognitive function in children with epilepsy prior to, during and after treatment with AEDs.
Methods
Study design and patient recruitment
This was a prospective observational study conducted between 2008 and 2011 at Derbyshire Children's Hospital. Children aged <18 years, attending outpatient clinics, and who were receiving one or more AEDs for any type of epilepsy were considered suitable for the study. Parents of the children were approached for consent, either at an outpatient appointment or during an inpatient stay.
Patients eligible for the study were considered for three possible groups. Children who were already receiving AEDs were recruited to group A—prospective surveillance only. At each clinically determined follow-up appointment, parents and the child were asked about any possible side effects. Details of the AED treatment, doses, seizures, etc. were recorded at each visit. Patients starting AED therapy for the first time (group B) had measurements of behaviour and cognitive function performed prior to starting treatment and 12 months after starting treatment (table 1). Patients who had been seizure free for a period of 12 months (group C) had measurements of behaviour and cognitive function performed while receiving AED therapy. Those who remained seizure free for a further period of 12 months and for whom the clinician in charge of the patient had decided to wean off AED therapy had further assessments 3 months after treatment was stopped, that is, at 18 months.
Categories of patients recruited into the study
Behaviour and cognitive function monitoring
Assessments of behaviour and cognitive function were performed by a clinical psychologist in subgroups B and C. Behavioural problems were quantified by using the Child Behaviour Checklist (CBCL); the Teacher Report Form (TRF), for children aged 5 years and over; and the Youth Self-Report Form (YSRF), for young people aged 11 years and older. Permission was obtained from the copyright holder to use the CBCL, TRF and YSRF for this study. Child Behaviour Checklists were available for the two age groups: 1.5–5 years and 6–18 years. If the child crossed between these age groups during the course of the study (ie, from 5 to 6 years), the same age-specific CBCL which was used during the first visit was then used for subsequent visits. The CBCL, TRF and YSRF have been used extensively in studies of behavioural problems in children.14–16 Concern, however, was raised that some of the items measured in the CBCL were ambiguous in relation to children treated with epilepsy.15 In view of this ambiguity, the CBCL was corrected for epilepsy-related item ambiguity as illustrated by workers in the Netherlands.16
Children were asked to complete an assessment of cognitive functioning. The Wechsler Intelligence Scale for Children (WISC-IV) was used to assess children aged 6–16 years. Children of age 4–6 years were tested using the Wechsler Preschool and Primary Scale of Intelligence Third Edition (WPPSI-III). The tests were performed at study entry and at 12 months for group B, and at study entry and 18 months for group C (table 1).
Definition of terms and causality assessment
Causal relationship between ADR and treatment was assessed by a researcher, with the Naranjo Algorithm17 and by a paediatric clinical pharmacologist based on clinical judgement. This ensured standardised assessment of suspected ADRs in relation to severity and likelihood. On the Naranjo algorithm, a score of >9 suggests a definite attribution to the drug; 5 to 8 indicates a probable cause, 1 to 4 for possible relationship and doubtful association if the score is <0. Using clinical judgement, all suspected ADRs were also classified as: Definite—directly attributable to a drug by having a clear temporal relationship to drug administration and confirmed by laboratory investigation, for example, abnormal blood values; Probable—occurring with a clear temporal relationship to drug administration and improving on withdrawal of treatment; Possible—some temporal relationship to drug administration but the effects could have been due to the basic or intercurrent illness or doubtful, if there was no relationship with the drug. These methods have previously been used in paediatric ADR surveillance studies.3 ,18–21
The severity of ADRs was classified as: Severe—fatal or potentially life threatening; Moderate—requiring treatment or prolonging the length of stay in hospital; Mild—no treatment required and no effect on length of stay in hospital.3 ,18
Sample size and statistical analysis
The planned sample size was 300–400 children with epilepsy, with at least 50 children in groups B and C to observe 7 IQ points difference from baseline (100 IQ Points) to follow-up, with statistical power 80% and significant level of 0.05. Statistical analysis was mainly descriptive. Fisher's Exact Test was used to compare the relative risk of ADRs in patients on monotherapy or polytherapy. Cognitive and behavioural scores for children in groups B and C were compared during and after treatment using Wilcoxon Signed Rank Test. Statistical analysis was performed using SPSS v21 at significant level of 0.05.
Results
Study characteristics
A total of 180 children were recruited into this study. A total of 141 children made up group A, 27 children were in group B and 12 children group C. The targeted sample size could not be reached over the course of the study. The median age of the patients was 11.2 years (IQR: 6.9–14.0).
A total of 135 children were on monotherapy and 45 on polytherapy. Over half of the children received either valproic acid or carbamazepine as monotherapy. Seventy-four per cent of all AED prescriptions were old generation drugs. The most frequently prescribed drugs were sodium valproate (33%), carbamazepine (25%), lamotrigine (13%) and levetiracetam (7%; table 2).
Number (%) of patients receiving different AED regimen
Adverse drug reactions
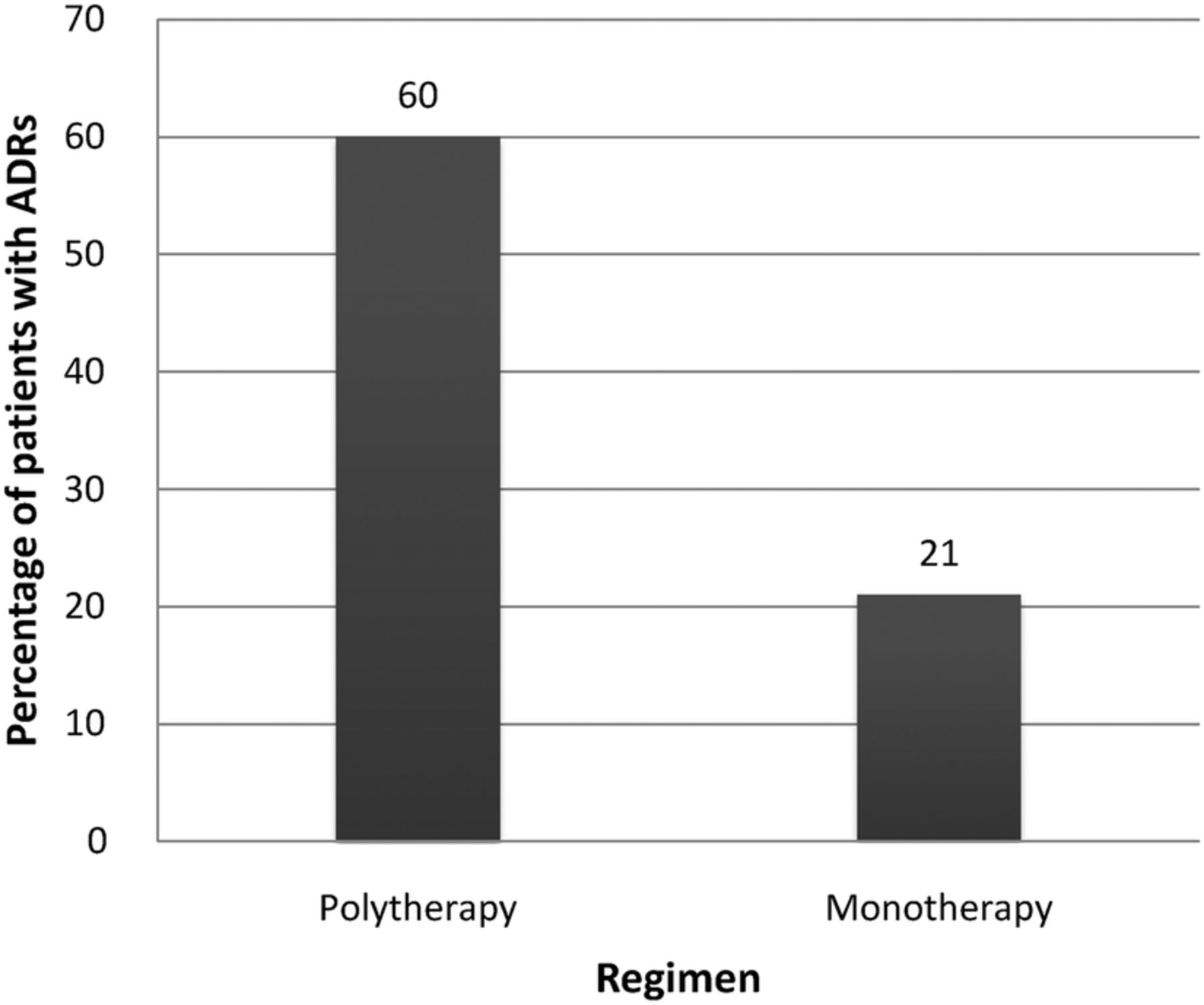
A total of 114 ADRs were recorded in 56 of the 180 patients (31%). Twenty-seven of the 45 patients (60%) on polytherapy experienced ADRs. In contrast, 29 of the 135 children (21%) on monotherapy experienced ADRs. The risk of ADRs was significantly lower in patients receiving monotherapy than those in polytherapy (RR: 0.61, 95% CI 0.47 to 0.79, p<0.0001; figure 1). The majority of the ADRs occurred with the two most widely used AEDs—valproic acid and carbamazepine. The most common ADRs were behavioural problems and somnolence (table 3). These accounted for approximately one-third of all ADRs. Rash was the third most common ADR, and was most common with carbamazepine and lamotrigine.
Adverse reactions to antiepileptic drugs
{kind=link}
Percentage of patients on antiepileptic drugs monotherapy and polytherapy experiencing adverse drug reactions (ADRs).
AEDs were discontinued in 23 children (table 4). Dose was reduced in 20 patients. Approximately one in 10 children receiving valproic acid, carbamazepine and lamotrigine had to stop treatment due to toxicity. Behavioural problems were the most frequent reason cited for valproic acid, and rash for both carbamazepine and lamotrigine. All three children receiving phenytoin had to stop treatment for a variety of ADRs.
Treatment discontinuation due to adverse reactions
All but four ADRs were considered either probable or possible by both the Naranjo algorithm and the paediatric clinical pharmacologist. The majority were considered probable (57% Naranjo and 79% by the paediatric clinical pharmacologist). Most ADRs were moderate (61%) with three severe. The three severe ADRs were Steven Johnson syndrome (2) and respiratory arrest.
Cognitive and behaviour functioning assessment
On the Wechsler IQ scale, the median IQ score when on treatment was not significantly different from the score off treatment (p=0.411). Although there was a marginal increase in median score on the behaviour checklist and impact of epilepsy scale, these differences were not significant (p=0.354 and 0.550, respectively). Similarly, there was no significant difference in the score during treatment and post-treatment on the youth report form (p=0.838; table 5).
Cognitive and behavioural scores for children in groups B and C during and after treatment
Discussion
About one-third of patients receiving AEDs in this study developed at least one ADR during treatment. Carbamazepine, valproic acid and lamotrigine were the most frequently prescribed AEDs. A similar AED prevalence pattern has been reported in other studies.22–24 These were also the most common causes of ADRs. The risk of treatment discontinuation was 1 in 10 patients for these three AEDs, with rash being the most common cause for carbamazepine and lamotrigine discontinuation. Others have shown similar discontinuation rates due to toxicity in children from carbamazepine and valproic acid;25 and carbamazepine and phenobarbital.26 Most AEDs are similar in efficacy but differ in safety.27 A large Chinese study had reported that similar proportions of children on carbamazepine, topiramate and valproic acid had adequate seizure control, while significantly more carbamazepine-treated children had treatment discontinuation due to ADRs, mainly rash.27 Han Chinese population, however, have a genetic predisposition to carbamazepine-induced rash.28 Carbamazepine is therefore not recommended as first-line treatment in Han Chinese without genotyping.
Most children in this study received monotherapy, with only 25% receiving polytherapy. Monotherapy for epilepsy became standard management in the 1970s as it was recognised that polytherapy was more likely to be associated with drug toxicity.29 AED used as monotherapy is effective in 60–70% of children.25 ,27 ,30 Additional drugs in refractory patients have been shown to be only marginally beneficial.31 ,32 Polytherapy is associated with a greater risk of drug toxicity in paediatric patients in general,18 ,33 especially those receiving AEDs.34 More children receiving polytherapy in this study developed ADRs, with up to a threefold higher incidence of ADRs compared to monotherapy. Unfortunately, most new AEDs are tested by the pharmaceutical companies as add-on therapy and drug toxicity is poorly described in these studies.8 This encourages clinicians to use polytherapy in epilepsy.
Since several of the AEDs share similar pharmacokinetic pathways, enzyme induction or inhibition may be a major problem with some drug combinations.35 One such combination is valproic acid and lamotrigine. Valproic acid inhibits lamotrigine glucuronidation, thereby increasing its plasma concentration and toxicity.36 ,37 AEDs also share similar pharmacodynamic mechanisms, which may have additive effects and increase the likelihood of ADRs. The use of AED combinations with different mechanisms of action has been advocated.35
There have been few pharmacovigilance studies of AEDs in children.4 ,38–40 The main ADRs identified in this study were behavioural problems (12%) and somnolence/sleep problems (10%). These were also the two most common ADRs in a previous study more than 20 years ago.4 Another study in India with a different AED utilisation pattern reported a lower incidence of behavioural effects (5.7%).38 While valproic acid and carbamazepine were the most commonly prescribed AEDs in this study, about two-third of the patients in the Indian study received phenytoin. We have reported no significant differences in cognitive and behavioural functions during and after AED treatment. A limitation of this study is the insufficient number of patients recruited. Much larger studies are required to adequately determine behavioural effects of AEDs. In addition, causality was assessed using the Naranjo algorithm, which is not paediatric specific. There is no paediatric specific tool to assess causality.
In conclusion, polytherapy increases the possibility of ADRs in children. Physicians should give AED polytherapy only when the maximum therapeutic doses of monotherapy are ineffective. Both clinicians and parents should monitor AED treated children for adverse reactions, especially behavioural problems and somnolence.
References
Footnotes
Contributors IC conceived the idea for the study. MA, JC and CM all contributed to the study design. MA, JC, IC and CM all collected data. OE, MA, JC, AF, CM and IC analysed the data and contributed to the manuscript.
Competing interests None declared.
Ethics approval Trent Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.