Article Text

Abstract
Although a great deal of paediatric consultations are not urgent, doctors in training spend so much time providing service for acute conditions that they spend little time focusing on outpatient work before they become a consultant. Engaging clinicians in the managerial aspects of providing clinical care is a key to improving outcomes, and this article addresses these aspects of the outpatient consultation from referral to discharge. We aim to provide doctors in training with a tool to use during their training and their first few years as a consultant, to think about how outpatient work is organised and how it can be improved to maximise patient experience. The non-urgent consultation varies across the world; this article is aimed to be relevant to an international audience.
- outpatients
- management
- Health Economics
- Paediatric Practice
- Patient perspective
Statistics from Altmetric.com
Introduction
Paediatric consultants spend more time seeing patients in non-urgent consultations and ambulatory settings than in acute and emergency settings; this will only increase as inpatient stays are reduced.1
Acute service needs are often prioritised over time in clinics for those in training. A survey in 2014 showed that less than half of trainees attended the recommended 20 clinics per year.2 In addition, new consultants often feel underprepared in dealing with the organisational and managerial challenges that consultancy brings (Sen C, Fertleman C. Feedback from STARTing to be a Consultant, July 2016, private communication) and may lack the confidence to function effectively in the outpatient setting, acquiring these skills later on. We feel that it is essential for those in training to understand not only the clinical aspects of care but also the managerial aspects of outpatient work.
Outpatients—the non-urgent consultation
In the UK, the term ‘outpatients’ is used to refer to clinical time spent seeing children during non-urgent consultations, which are generally preplanned. In the USA, this is usually described as a consultation, or a consult. The terms will be used interchangeably in this article.
In low-income settings, the remit of outpatients may be different. Children can often present directly to outpatient clinics, with a wide spectrum of clinical conditions. Some children will be acutely unwell and will be managed appropriately, but this situation will not be explored further.3
How are outpatients different?
Paediatric outpatients are unique; more patients are seen once, as a ‘new’ patient, than in adult medicine, where most outpatient work is repeat consultations with patients with chronic disease. Non-urgent consultations offer a perfect setting for innovation, using modern ways of communication, developing a clinic model around the needs of children, young people and their families. Paediatrics in the outpatient setting provides both a challenge and opportunity for senior paediatric trainees.
How are clinics structured?
Throughout Europe, children are referred by their general practitioner or primary care paediatrician to a general paediatric clinic. Children can also be referred from secondary care providers, typically following an emergency department attendance. Referrals to a specialist clinic usually come from secondary care. In health systems such as the USA, family physicians can refer for more specialist input and patients can also self-refer. In low-income countries, self-referrals are also common because of limited access to primary care.4 Children are also referred from lower level health facilities or dispensaries if they have signs of serious illness or cannot be managed locally.5
Referrers will also consider how quickly they would like a child to be seen (figure 1). Each clinic will see new patients and ‘follow-ups’; those who have attended previously. Different consultants will have diverse clinic templates to deal with the different types of patient they see. There is flexibility to alter the clinic template and the ratio of new to follow-up patients.
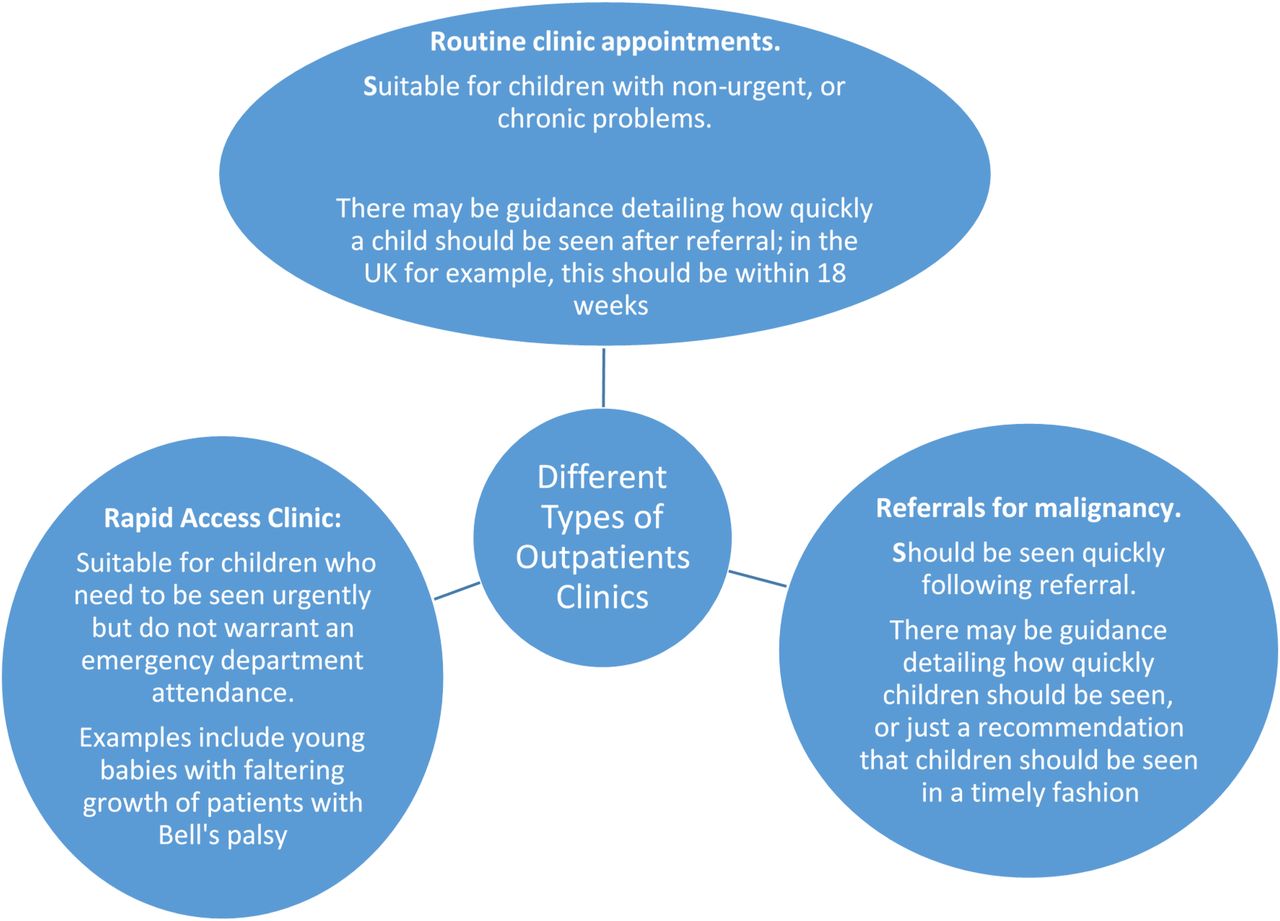
Different types of outpatient clinics based on length of wait to be seen.
For example, new patients may be seen first and allocated more time than follow-up patients. Conversely, new and follow-up appointments can be interspersed and there is flexibility to alter the ratio of new patients to follow-ups seen. Early clinic slots may work well for parents with young children, when parking is easier. Not all follow-up appointments need to be face to face; innovative options using telephone or email can give more flexibility.
Specialty clinics also run slightly differently. For example, clinics for children with cystic fibrosis require a patient and their parent/carer to remain in one room and the health professionals to move between. This is also an example of a multidisciplinary clinic, as a minimum involving a doctor, a physiotherapist and a dietitian.
How are referrals received and prioritised?
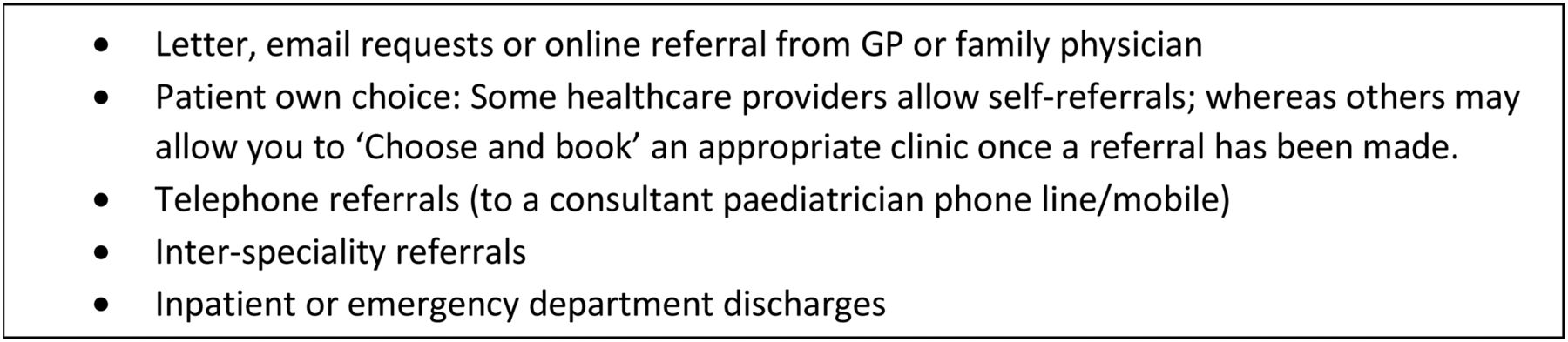
Referrals for non-urgent consultations are received through multiple routes (figure 2). Normally, a consultant triages referrals into different clinics, each with different waiting times. This may be the ‘consultant of the week’, or a consultant who understands which of their colleagues would be best to see a particular patient. Some care providers accepting referrals in the USA will ask for a minimum set of investigations to be done by the referrer before the referral is accepted.6
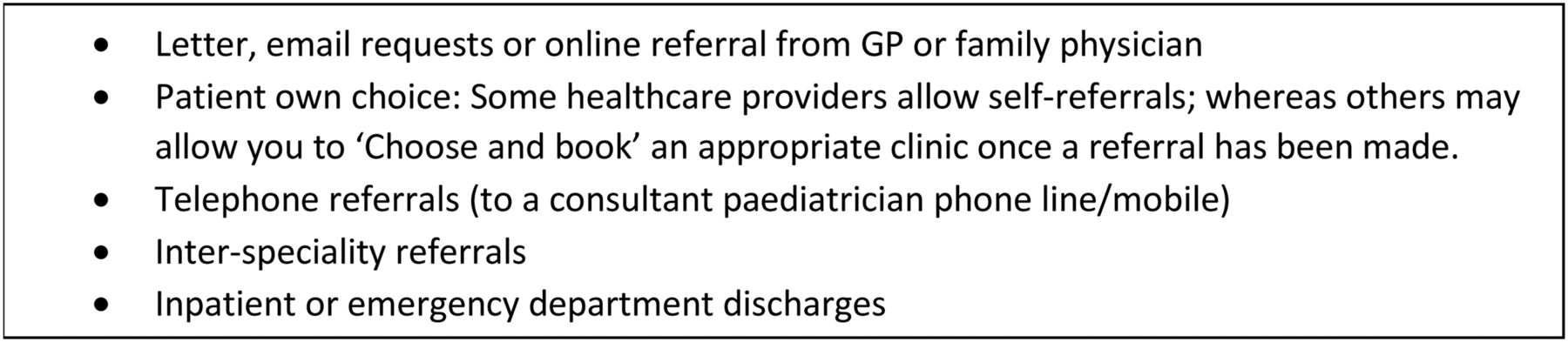
Routes of referral.
Some children referred through the outpatient route may be more appropriately seen in the emergency department or at an emergency clinic. This would be the case for a referral suggestive of raised intracranial pressure, or a non-reducible hernia. Sometimes extra information may be required before deciding the most appropriate setting for review; it is reasonable to contact the referrer for more details.
During clinic
In higher income settings, clinics are run based on the patient list. In low-income settings, many facilities operate a queue system, whereby people turn up and wait to see a specialist without a referral.4 A designated doctor would normally manage this group of patients. In any setting, a patient can come as planned but present an unexpected challenge, for example, being acutely unwell, or raising a significant safeguarding issue. It is important in these situations to involve appropriate team members to keep other patients updated while they wait.
Making best use of time in clinic
It is important to think about capacity to ensure that a clinic functions well. Are patients seen in a timely fashion? Are the allocated time slots appropriate? Are there adequate personnel to staff the clinic and enough rooms to see patients? Does the number of patients being discharged from clinic match the number of new referrals? Although this may not always be possible, especially in a clinic for chronic disease, having an overview of the clinical need versus the resources available is crucial. Clinics should run to time whenever possible (figure 3).
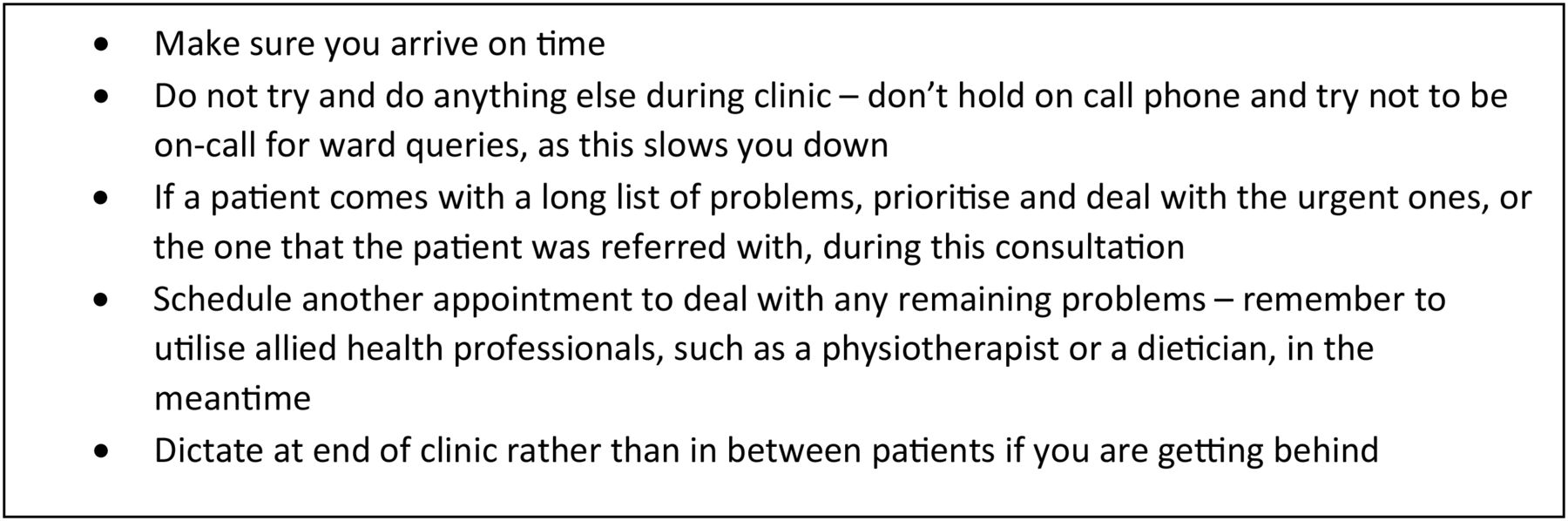
Strategies to help with time management in the outpatient setting.
What is best practice for using an interpreter?
With over 7000 registered languages spoken worldwide,7 it is not surprising that the clinicians and their patients often speak different first languages. Using an interpreter is important to improving consultations and outcomes.8 If no interpreter is available, a telephone interpreting service can be invaluable.9 Some simple tips can improve communication with families when using an interpreter (figure 4).⇓ ⇓

Working with an interpreter.

Options for ongoing care.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Top tips from a new consultant: What a new consultant wishes they had known during their final years as a doctor in training.
What is the best way of prescribing for clinic patients?
Medications can be prescribed directly from the specialist in clinic or the referrer can be asked to prescribe them. This depends on whether the medicine is urgent and who is taking responsibility for ongoing care. Clear communication in the clinic letter, and to the family so they understand how to get repeat scripts, is vital. If the medicine is on the specialist prescribing register, it should be started by a specialist (such as a hospital paediatrician or specialty doctor), but the referrer should be contacted to ensure they are happy to continue prescribing it. Some medications are available over the counter, such as paracetamol, and should generally not be prescribed. Certain medications have different formulations, some of which taste better than others.
Prescribing practice will vary depending on the healthcare system and the method of payment for the medicine prescribed. The cost of medicines is generally subsidised by the government, but the amount of subsidy varies.10 Patients then have to make a ‘copayment’ for the rest of the medication, which is either a fixed amount or a percentage of the cost. In some healthcare systems, particular patient groups, such as pregnant women or children, get these medicines without charge.
How to decide who to follow-up?
At the end of a clinic appointment, the doctor must decide on an outcome and follow-up plan. Recording this ensures that the care provider is paid for the consultation and provides an easy method to monitor activity.
How does payment for outpatients work?
Different specialty clinics will have different tariffs for outpatient appointments. In the UK, this will be based on the expected level of activity negotiated with the local clinical commissioning group and NHS England. This will be tracked and monitored to ensure that trusts are paid correctly. Overperformance and underperformance will have a different effect on a trust depending on whether they are on a block or on an activity-based contract. A block contract means that trusts have pre-agreed target numbers. They will be paid the same amount irrespective of whether they see more patients than expected. A contract based on activity will reward a trust by paying them more for overperformance. Trusts will be financially penalised for underperforming if on an activity-based contract. Understanding how your care provider is paid for outpatient work will help you understand some of the different pressures placed on consultants about following up patients, and ultimately help you to work with commissioners to improve a service.
After clinic
How to manage children who ‘do not attend’ or ‘are not brought’?
Deciding how to follow-up children who did not attend is a challenge. Some care providers offer new appointments for children who are not brought, and others will discharge patients back to the referrer. Before discharging a patient, it is important to consider if safeguarding concerns have been raised by the referrer, or whether the non-attendance itself raises any queries. If children are subject to a child protection plan, their named social worker should be informed. If the referral was for an urgent problem, this should be followed up. If the child is discharged, the referrer should be informed. Irrespective of local policy, if there are concerns, a follow-up appointment can be rescheduled.
How to communicate the outcome of a consultation?
It is vital to communicate a plan to the family during the consultation and this must also be followed up in writing. Usually, this will be in the form of a letter to the referrer, but there may be times where more urgent communication is warranted, either by phone or by email.
While addressing a letter to the referrer, unless there is sensitive information being shared between care providers, which is not to be shared with the family, the family should be copied in. However, it is becoming accepted practice to address a letter to the patient or family. There is evidence to suggest that this improves compliance with a management plan and improves patient satisfaction, with families feeling more involved in their care.11 ,12 Email is being increasingly used; there is evidence to show clear financial benefits, that it is not abused and that it improves the satisfaction of both patient and doctor.13 ,14 Any email communication should be done via a secure email provider, such as NHS mail. If sending to a non-NHS mail account, this can be made secure by writing [SECURE] in the subject line.
There is no right or wrong structure for letter writing, but the Royal College of Paediatrics and Child Health gives guidance.15 Letters should be structured with the salient points of consultation including any actions for the ongoing care provider easily visible at the start. Assessment of letters written in clinic is part of the competencies of any doctor in training.
Some clinicians dictate their letters after each patient, some at the end of clinic and some wait until later. Alongside the move towards electronic patient records, some clinicians will use the uploaded consultation letter as their documentation. While this avoids duplication, this does not allow for notes to be made about details not mentioned in the letter. If you are writing contemporaneous notes, they should be sufficiently detailed so as to fully remember each patient, especially if dictation occurs at a later point.
Unless there is good reason, letters should be copied to all professionals involved in childcare. For complex patients, it may be worth listing the professionals involved in the body of the letter.
Following up results
It is vital to have a fool proof method of following up results for patients seen in outpatients. Options include a notebook, keeping copies of the clinic list or creating a spreadsheet. There is no correct option, but whichever option is chosen must allow for timely and accurate record keeping. These results should then be communicated to parents. It may be appropriate to wait until the next clinic appointment, but sometimes it is better to contact the parents/child before this, perhaps with a phone call, separate letter or an email.
New innovations to improve patient experience
One challenge of working in paediatrics is the variation in the paediatric population: the needs of adolescents are very different from the needs of toddlers. Clinic templates and methods of consultation can be modified to maximise patient experience. For example, evening or weekend consultation for teenagers with chronic diseases, such as diabetes, has been shown to improve patient experience and adherence to treatment plans.16 Some families may prefer consultations in school holidays, others in term time. Other avenues for development include virtual consultations, telemedicine and using Skype. Particularly for families with children with chronic disease, a virtual consultation will have significantly less impact on their life than a face-to-face consultation, especially with a specialist some distance away.17 ,18
It is now required for consultants to get individual feedback from their patients. There are many ways to collect this—paper forms can be handed out in clinic, patients can be sent texts or letters to ask for feedback or doctors could even include a link when communicating with patients via email.19 This could be used by doctors in training too.
Seeing children in outpatients also offers a valuable opportunity to screen for other health problems (such as obesity or missed vaccinations), to take a psychosocial history from adolescents and to offer targeted health promotion.20
In low-income settings, the WHO has developed the ‘Integrated Management of Childhood Illness’ programme for use in outpatient settings. It focuses on the overall well-being of a child and incorporates both preventative and curative aspects.21 With the global epidemic of obesity, high-income countries could learn from models, which innovatively bring together public health and clinical medicine in the outpatient setting.
Visualising the future
As healthcare systems develop, it is becoming increasingly common for health professionals other than doctors to see children in the outpatient setting. Physician's associates are widely used in the outpatient setting in paediatrics in America22 and the roles of advanced nurse practitioners and clinical nurse specialists are also set to increase. Using other healthcare professionals in the outpatient setting can reduce waiting times, improve patient satisfaction and increase cost effectiveness.23 The WHO has advocated this as a strategy to expand the health workforce in low-income settings, and increase access to services. There is growing evidence that other healthcare workers can provide care comparable to medical professionals, with adequate training and supervision.24
Conclusions
Outpatients offer a variety of challenges for the paediatric practitioner. Careful planning and awareness of the logistical and organisational challenges of the non-urgent consultation can allow both trainees and consultants to optimise the pathway for patients and their families.
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.