Article Text

Abstract
Background: Knowledge about assent or dissent of children to non-therapeutic research is poor.
Objectives: To assess sociodemographic characteristics in healthy children and adolescents who were invited to participate in non-therapeutic research, to evaluate their motives for assent or dissent and their understanding of the information given.
Methods: A total of 1281 healthy children and adolescents six to sixteen years of age were invited to participate in a non-therapeutic study and a questionnaire.
Results: Assenting children were motivated by a desire to help sick children (n = 638, 98%) and to gain experience with participating in a research study (n = 503, 82%). Dissenting children made their decision because of worries about having a blood (n = 193, 46%) or a urine sample (n = 94, 26%) taken or because of worries about a doctor’s examination (n = 136, 33%). Fewer children in the assent group (n = 166, 25%) than in the dissent group (136, 33%) worried about the doctor’s examination (p = 0.01). In the assent and dissent group, 568 (86%) and 343 (85%) children, respectively, said they were able to understand some or all of the written information (p = 0.42), and 650 (97%) and 330 (98%), respectively, were able to understand some or all of the verbal information (p = 0.07).
Conclusions: Sociodemographic characteristics may not influence healthy children’s decision to volunteer for non-therapeutic research. Assenting children have altruistic and educational motives, whereas worries about procedures may cause children to dissent. A great majority of school children and adolescents feel capable of understanding and giving assent or dissent to non-therapeutic research.
- ethics
- informed consent
- clinical research
- healthy volunteers
- research subjects
Statistics from Altmetric.com
Non-therapeutic research is needed in many areas of paediatrics. There is a continuous need for studies to establish normative age references of physiological and biochemical parameters as part of the diagnosis and clinical assessment of various diseases. In most countries children younger than 16 years of age cannot legally consent to participate in research: their consent being delegated to their parents or legal guardian.1–3 Generally, the informed consent is understood as informed parental permission and assent of the child.1,4 The capability of children to give assent depends on age and relates to their cognitive, emotional, and social development; however, it has been suggested that factors such as general health status and anxiety about invasive procedures might play a role as well.5–7 The few available evaluations of children’s understanding of the information given in clinical studies have shown poor results.8 Therefore, attention has been increasingly focused on the need to provide verbal and written information in a form that the child can understand to potential study participants. It has been recommended that the content, the language, and the mode of communication should be adapted to assist the child to make an independent decision.2 Assessment of possible effects of differentiated information procedures, however, has not been performed and little information, if any, on factors that may influence decision making in healthy children who are asked to participate in non-therapeutic research has been provided. The aims of the present study were to assess sociodemographic characteristics in healthy school children and adolescents who are invited to participate in non-therapeutic research, and to evaluate their motives for assent or dissent, and their understanding of age differentiated information.
SUBJECTS AND METHODS
A total of 1281 healthy Danish speaking children six to sixteen years of age, all pupils in first to tenth grade in three public schools, were invited to participate in a non-therapeutic study, which aimed at providing normal reference data for serum and urine markers of the insulin-like growth factor axis and collagen turnover. Participation in the study involved a one-time fasting blood draw in the morning taken at school; a one-time fasting morning urine void collected at home; a clinical examination, which included assessment of pubertal development and measurement of weight and height, and the completion of a questionnaire. To reduce the discomfort of venipuncture an anaesthetic aqueous aerosol (Xylocain®) was used. No reward for participation was offered or given. The children gave consent to the non-therapeutic research and the questionnaire separately. The study protocol and the questionnaire were approved by the local ethics committee.
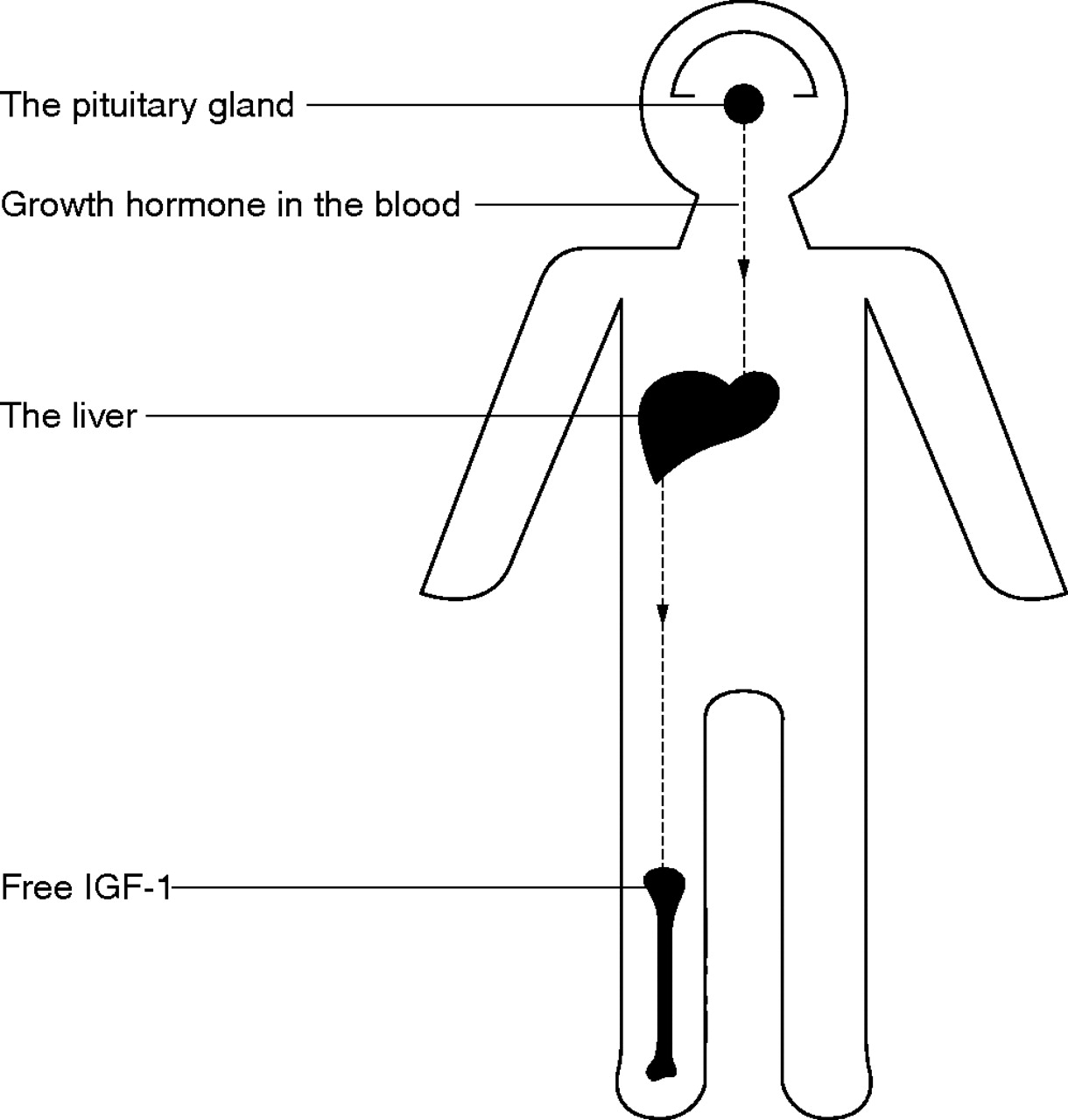
The headmasters of the schools were approached individually and were given verbal information based on a schematic diagram of the anatomy of a child in the shape of a puppet. In the diagram the basics of the relation between the pituitary secretion of growth hormone, the liver’s synthesis of growth factors, and effects of growth factors on bones were shown (fig 1). Furthermore, the written information, which consisted of a single sheet of paper with 24 lines of text (305 words), (table 1), and the questionnaire were presented to the headmasters.
Information to participants and parents
{kind=link}
A diagram showing the relation between the pituitary secretion of growth hormone, circulating growth hormone, and the liver’s synthesis of growth factors, one of which is free insulin-like growth factor-1 (IGF-1), which stimulates the growth plates in bones.
After this initial approach, separate meetings with the teachers at each school were arranged, which, again, were followed by meetings with the parents of each class over a period of two months. At the meetings the study was presented in accordance with the information given to the headmasters. Teachers and parents were asked to come up with as many questions as possible to better elucidate all aspects of the study. Verbal approval from the parents was obtained to approach their children in class. Furthermore, consent forms were handed out to the parents. However, parents, as well as teachers, were asked not to talk to the children about the study before we had been in contact with them.
Verbal information was given to the children in their classrooms. In all age groups we presented the diagram of a puppet to explain the rationale of the study, and the equipment used for blood and urine sampling was shown to each child so that he or she could become acquainted with it. For the six to ten year old group we created an interactive play using the puppet and ourselves as players to illustrate urine sampling at home, venipuncture at school, weight and height measurements, and a doctor’s clinical examination. Furthermore, within a few days of our information sessions a story about a boy who underwent venipuncture for assessment of a growth problem was read to the children by one of their teachers.9 In the children 11 to 14 years of age the puppet was used to illustrate urine and blood sampling, weight and height measurements, and a clinical examination; the puppet was not used when giving verbal information to the 15 to 16 year olds. At completion of the verbal information sessions the written information and consent forms were handed out to the children. The children were asked to read the information themselves before asking their parents for help, if needed. Furthermore, they were asked to make up their own mind about giving assent or dissent, if possible, before presenting the information and consent form to their parents. Written consent was given by the parents to the study and/or to participation in the questionnaire.
The questionnaires were handed out to the children in their classes within a week after the children who had assented to the study had completed this study. Members of our research group had talked to the teachers about the questionnaire, so the teachers were fully informed about the meaning of the questions. The questions were read out loud to the children in class by a member of our research group, and the meaning of the questions were explained to them. All children were offered the opportunity to answer the questionnaire in class with access to assistance from a teacher. However, children six to ten years of age were asked to complete the questionnaire at home with their parents, and all children were urged to ask parents for information regarding any question if in doubt.
The questionnaire was semistructured, with 28 questions for the children who dissented and 34 questions for the children who assented to the study. Four questions were open, 24 were in multiple choice and “fill in the blank” format, and six questions were combinations of open and multiple choice format.
DATA ANALYSIS
The questionnaires were coded and the data were entered into a computer spreadsheet. For validation purposes, data were entered twice into the database. Statistical analysis of individual categorical responses was conducted by Pearson’s χ2 test using the 5% significance level. All analyses were performed using SPSS 9.0 statistical software (SPSS Inc, Chicago, IL, USA).
RESULTS
A total of 1084 children (85%), 501 boys (46%) and 583 girls (54%), returned the questionnaire. Five hundred and forty eight (50%) completed the questionnaire themselves; 482 (44%) were assisted by their parents. Six hundred and sixty seven of the children (62%) had and 417 (39%) had not assented to the study. Of 197 children (15%) who did not complete the questionnaire, 92 (47%) of them had and 105 (53%) had not given assent to the study. There were no differences with respect to age or sex between completers and non-completers except that in the 16 year olds there were more non-completers (n = 18 (26%)) in the group that had not assented to the study than in the group that had assented (n = 1 (0.01%)).
Sociodemographic characteristics
Table 2 summarises the sociodemographic characteristics of parents of children who assented or dissented to the study. No significant intergroup differences were found in parental educational or occupational characteristics.
Sociodemographic characteristics of parents of children who gave assent or dissent to a non-therapeutic study
Reasons for assent and dissent
A number of questions aimed to assess whether personal experiences with chronic disease, hospitals, or invasive procedures were associated with assent rate. The children were asked about the presence of chronic disease in parents and siblings; if they had ever been admitted to hospital; if they had ever had a blood sample taken, and if they had had a blood sample taken within the previous year. Two hundred and seven children (31%) in the assent group and 60 (15%) in the dissent group had had a blood sample taken within the previous year (Pearson’s χ2 test 37.2; df 1; p<0.01). Otherwise, there were no statistically significant differences between the two groups with respect to answers to these questions.
The children who gave assent to the study were asked about reasons for their decision. They almost all stated that they wanted to help sick children (n = 638, 98%). Many wanted to gain experience by participating in a research study (n = 503, 82%), and a majority of them said that their parents (n = 310, 55%), their classmates, (n = 310, 55%) and their teachers (n = 402, 68%) thought participation was a good idea.
The children were asked if during the decision making process they had worried about the prospect of having a blood sample or a urine sample taken and if they had worried about undergoing a doctor’s examination (table 3).
Distribution of worries in 667 children who assented and in 417 who dissented to a non-therapeutic study
In the assent group more girls (n = 196, 58%) than boys (n = 109, 37%) (Pearson’s χ2 test 27.5; df 1; p<0.01) worried about having a blood sample taken. Similar results were found in the dissent group (girls: n = 128, 64%; boys: n = 65, 40%) (Pearson’s χ2 test 20.5; df 1; p<0.01)). Otherwise, there were no sex related differences in any of the worries.
The children who dissented to the study were asked four further questions, which aimed to elucidate why they chose not to volunteer. A substantial proportion of them said they had thought their participation was not needed for the study to be accomplished (n = 95, 28%). A few children gave other reasons. Some said they did not understand the purpose of the study (n = 25, 7%), and some said they did not understand the verbal (n = 12, 4%) or the written information (n = 9, 3%). Significantly more boys (n = 66, 42%) than girls (n = 29, 16%) (Pearson’s χ2 test 30.1; df 1; p<0.01) thought their participation had not been needed; otherwise, there were no sex related differences between the answers.
Understanding
Tables 4 and 5 show the responses of the children to questions aimed at elucidating their understanding of the verbal and written information.
Distribution of affirmative answers (percentages) by age to questions aimed at evaluating information procedures in children invited to participate in a non-therapeutic study (n = 1067)
Distribution of answers to questions aimed at evaluating information procedures in 662 children who assented, and in 406 children who dissented, to a non-therapeutic study
Ninety one (14%) of the children who gave assent to the study and 62 (15%) of the children in the dissent group were not able to read the written information. One hundred and thirty eight (90%) of these children were six to eight year olds. Having had the written information explained by a parent, only 24 children (4%) in the assent group and 21 (5%) children in the dissent group did not understand any of the written information. Twenty one (47%) of these children were six to eight year olds. Only six children (1%) in the assent and nine children (2%) in the dissent group said they did not understand any of the verbal information. Children who gave assent to the study were more likely than children who gave dissent to feel they had understood the written information and they were more sympathetic toward the way in which the verbal information was given (table 5).
DISCUSSION
Previous assessments of sociodemographic characteristics of parents volunteering their children for therapeutic trials have shown conflicting results.10–12 One study found non-volunteering fathers to be better educated, with a greater proportion of prestigious and skilled occupations than volunteering fathers.10 Similarly, non-volunteering mothers were over-represented in the professional and administrative occupational categories. This was thought to be a reflection of families of lower socioeconomic status perhaps having less access to the healthcare system and wanting to increase their access and social contact by volunteering.10 Another study found no negative correlation with parent’s education level—which, however, tended to be high as a whole—in a group of children participating in a trial of asthma medication.11 The discrepant results may have been influenced by national differences in socioeconomic characteristics and in health service provision between Australia and the United States, which influenced families’ access to the healthcare system. To some extent these studies may have been biased by insufficient, or even the complete absence of, comparative groups. In the present study, which applied an adequate comparative group of children who chose not to assent to the study of growth factors, no variations in sociodemographic characteristics could be detected between families who consented and families who did not. The finding suggests that socioeconomic status related factors such as social vulnerability, health seeking behaviour, and poor economy, which may be of some importance to parents of children with chronic diseases consenting to therapeutic trials, do not affect recruitment of children to non-therapeutic research.10 Whether that holds true in countries with sociodemographic distributions that are different from those in Denmark remains to be investigated.
A few studies have evaluated parent’s motives for volunteering their children for therapeutic research; however, children’s motives for participating in therapeutic or non-therapeutic research have not been assessed. Parents may be motivated by a desire to help others and to contribute to medical science and/or by a desire to learn more about their child’s illness, and thereby help to make their child better.10–12 In line with the parental motives, the children in the present study volunteered for the non-therapeutic research project for two significant reasons. They wanted to be of help to children with illnesses and they wanted to gain experience by participating in a study. In a majority of the children the altruistic and educational motives were supported by teachers, parents, and classmates. Remarkably, however, 13–20% of six to eleven year olds and 33–53% of twelve to sixteen year olds had not discussed their decision to assent with their parents. The findings in the oldest age group are in accordance with the results of a questionnaire in which adolescents were asked about their view as to the need for parental consent for adolescents to take part in studies involving blood or urine testing. A total of 42% of the adolescents felt that parental consent was not needed for these procedures.13 It was therefore, perhaps, more surprising that so many of the young children in the present study reported that they did not discuss their participation with their parents. We believe, however, that this was a consequence of us informing parents separately and specifically asking them to allow their children to decide about participation on their own if they felt they were able to do so. It must be remembered also that we encouraged the children to make up their own minds about giving assent or dissent before presenting the information and consent form to their parents, which probably helped to explain the fact that assent to the study did not depend on whether or not the children had discussed their participation with parents or classmates.
Though 19–46% of the children had worried about blood sampling, urine collection, or the doctor’s examination, only the latter came out as a statistically significant difference between assenters and dissenters. Worries about the doctor’s examination were associated with a higher dissent rate. In spite of the worries about these procedures, however, a great majority of children who were worried chose to assent. This suggests that there may be inherent differences between assenters’ and dissenters’ ability to cope with worries about invasive procedures. To some extent, not being able to cope with worries about having a blood sample taken was probably related to lack of experience of this procedure, since having had a blood sample taken recently was associated with a statistically significantly increase in assent rate.
Studies using objective methods for assessment of parent’s and children’s consent or assent have found an apparent discrepancy between parent’s subjective perception of adequate information and objective assessments of understanding in parents and children.14–16 In an interview study in 102 seven to seventeen year old children and adolescents who participated in anaesthetic or surgery research, the subject’s perceived understanding of the core elements of consent was significantly greater than their objectively measured understanding, which varied from 30–90%.15 In the present study we were interested in assessing whether the perceived understanding of written and verbal information in children who were invited to participate in non-therapeutic research influenced assent and dissent rates. We agree with the perception that whether or not a child is able to achieve complete understanding of informed consent may be different from whether he or she has the capacity to meaningfully assent or dissent to a study.17 Therefore, we used the subjective method of asking the children to judge themselves whether they felt they could understand the information given. It was evident that the perception of understanding and the feeling of grasping the information given were associated with increased assent rate. From the age of nine approximately 95% of the children felt they were able to read some or all of the written information, and in the six to eight year old group more than 85% felt that they were able to understand it when they were assisted by a parent. Furthermore, approximately half of the six year olds and more than two thirds in the seven to sixteen year old group felt they understood the verbal information completely; very few felt they did not understand it at all. The findings indicate that when focused one-page written information is used in combination with age differentiated verbal information, and given in the setting of a school, very few children are left without understanding, and in fact the great majority of them are able to meaningfully assent or dissent to non-therapeutic research. The low percentage of children who felt they did not understand any of the verbal information could probably have been reduced by giving the children verbal information individually, in addition to the verbal information they were given in class.
The present study has provided evidence that sociodemographic characteristics do not influence healthy children’s decisions to volunteer for non-therapeutic research. A majority of children give assent for altruistic reasons and because they want to gain experience by participating in a research project. Worries about procedures such as venipuncture, urine collection, and a doctor’s examination cause a minority of children to dissent. When age differentiated information procedures are used a great majority of school children and adolescents are capable of understanding and of giving meaningful assent or dissent to non-therapeutic research.
Acknowledgments
Thanks to Mrs Anne Karina Kjaer, study nurse, Mrs Charlotte Gradmann, study nurse, and to Dr Carsten Heuck, research fellow, for helping with the verbal information. Thanks to headmasters, teachers, and students at Randers Realskole, Hadsundvejens Skole and Hobrovejens Skole, Randers, for providing fine working conditions. The study was supported by a grant from Konventualinde Emilie De Lancy’s Foundation.
REFERENCES
Other content recommended for you
- Are positive experiences of children in non-therapeutic research justifiable research benefits?
- Children’s consent and paediatric research: is it appropriate for healthy children to be the decision-makers in clinical research?
- The child's perspective on discomfort during medical research procedures: a descriptive study
- The problem of informed consent in emergency medicine research
- Assessment and management of children aged 1–59 months presenting with wheeze, fast breathing, and/or lower chest indrawing; results of a multicentre descriptive study in Pakistan
- Non-therapeutic research with minors: how do chairpersons of German research ethics committees decide?
- Ethics in studies on children and environmental health
- Why do parents enrol their children in research: a narrative synthesis
- Paediatric HIV infection
- Little in Norway: a prospective longitudinal community-based cohort from pregnancy to child age 18 months