Article Text

Abstract
Background Europe has experienced a marked increase in the number of children on the move. The evidence on the health risks and needs of migrant children is primarily from North America and Australia.
Objective To summarise the literature and identify the major knowledge gaps on the health risks and needs of asylum seeking, refugee and undocumented children in Europe in the early period after arrival, and the ways in which European health policies respond to these risks and needs.
Design Literature searches were undertaken in PubMed and EMBASE for studies on migrant child health in Europe from 1 January 2007 to 8 August 2017. The database searches were complemented by hand searches for peer-reviewed papers and grey literature reports.
Results The health needs of children on the move in Europe are highly heterogeneous and depend on the conditions before travel, during the journey and after arrival in the country of destination. Although the bulk of the recent evidence from Europe is on communicable diseases, the major health risks for this group are in the domain of mental health, where evidence regarding effective interventions is scarce. Health policies across EU and EES member states vary widely, and children on the move in Europe continue to face structural, financial, language and cultural barriers in access to care that affect child healthcare and outcomes.
Conclusions Asylum seeking, refugee and undocumented children in Europe have significant health risks and needs that differ from children in the local population. Major knowledge gaps were identified regarding interventions and policies to treat and to promote the health and well-being of children on the move.
- children’s rights
- general paediatrics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Europe has experienced a significant increase in migration of displaced people escaping humanitarian crises.
Displaced children are known to be vulnerable to violence, violation of their rights and discrimination.
The existing literature on the health of children on the move in Europe is largely focused on infectious disorders.
The Convention on the Rights of the Child provides children on the move with the right to the conditions that promote optimal health and well-being and with access to healthcare without discrimination.
What this study hopes to add?
Indicates that the main challenges for child health services lie in the domain of mental health and well-being.
Indicates that many children on the move in Europe are insufficiently vaccinated.
Identifies significant gaps in knowledge, particularly with regard to policies and interventions to promote child health and well-being.
Identifies research priorities to promote effective, ethical care and support health policy.
Introduction
Forced displacement is a major child health issue worldwide. More than 13 million children live as refugees or asylum seekers outside their country of birth.2 Conservative estimates suggest that nearly 1 80 000 children on the move are unaccompanied or separated from their caregivers.2 The majority of these children live in Asia, the Middle East and Africa.3
Europe has experienced a marked increase in the number of irregular migrants since 2011, with a peak in arrivals during 2015.4 Children have accounted for a large proportion of people making the journey, either with family or on their own, in search of safety, stability and a better future. Between 2015 and 2017, more than 1 million asylum applications were made for children in Europe.4 The majority of these children originated from Syria, Iraq and Afghanistan.3 In 2017, 70% of the 210 000 asylum claims made for children in Europe were filed in Germany, France, Greece and Italy.5
The phenomenon of migration to Europe has been characterised by continual evolution, with frequent changes in the most common migration routes, modes of travel and the length of stay in transit countries. Children making these dangerous and often prolonged journeys are exposed to considerable health risks. The health of children on the move is related to their health status before the journey, conditions in transit and after arrival and is influenced by experience of trauma, the health of their caregivers and their ability to access healthcare.6
Much of the literature on the health of children on the move comes from North America and Australia. In light of the marked increase in the number of children arriving in Europe and the need for improved understanding of the situation for these children in the European context, this paper reviews the health risks and needs of children on the move in Europe and how European health policies respond to these risks and needs. It is important to note that children may live for months or years in one or several countries before settling, being repatriated or going underground. In the longer term, factors such as the social determinants of health, ethnicity and issues relating to legal status and prolonged periods of transit begin to take precedence.
The Convention on the Rights of the Child (CRC) affords all children with the right to healthcare without discrimination.7 Articles 2, 9, 20, 22, 30 and 39 devote specific attention to the rights of displaced and unaccompanied children.7 As such, the CRC provides a useful framework to address the health of children on the move.
Terms such as migrants, refugees and asylum seekers are often used interchangeably and may shift the focus away from people towards political discourse. In this paper, we focus on asylum seeking, refugee and undocumented children (table 1). Undocumented children are included because they are known to be a mobile and highly marginalised group, with particular barriers in access to services. We use the term ‘children on the move’ for these three groups of children in order to maintain a rights-based focus.
Definitions
Methods
The findings presented in this review are based on a comprehensive literature search of studies on the health of children on the move in Europe from 1 January 2007 to 8 August 2017. Searches were run in PubMed and EMBASE on 8 August 2017. Search terms included combinations of terms for children such as ‘child’, ‘youth’ and ‘adolescent’ with terms for migrant, such as ‘migrant’, ‘asylum seeker’, ‘refugee’ and ‘undocumented migrant’ and with terms for countries in the European Union as well as five countries that are major origin and transit countries for children travelling to Europe, including Afghanistan, Jordan, Lebanon, Syria and Turkey. The database searches were limited to papers providing data on children (birth–18 years) in the English language. Papers were included if they addressed physical and mental health of children on the move, health examinations of these children, the effect of caregiver mental health, access to care or disparities in care between children on the move and the local population. Multiregional reviews that provided data on children in Europe were also included. Papers on adult populations (defined as a study population ≥18 years) that did not provide disaggregated data on children were excluded. However, papers including UASC with a stated age ≤19 years were included, as well as longitudinal cohort studies that followed migrant children into early adulthood (<24 years old). Additional exclusion criteria included special populations, small single-facility studies, lack of migrant and/or health focus, intervention studies that did not provide data on child health outcomes and papers from non-European host countries. Commentaries and conference abstracts were excluded. For further information on specific child health and policy topics, hand searches were also undertaken to identify relevant peer-reviewed papers and grey literature reports.
Patient and public involvement
No patients were involved in this study.
Results
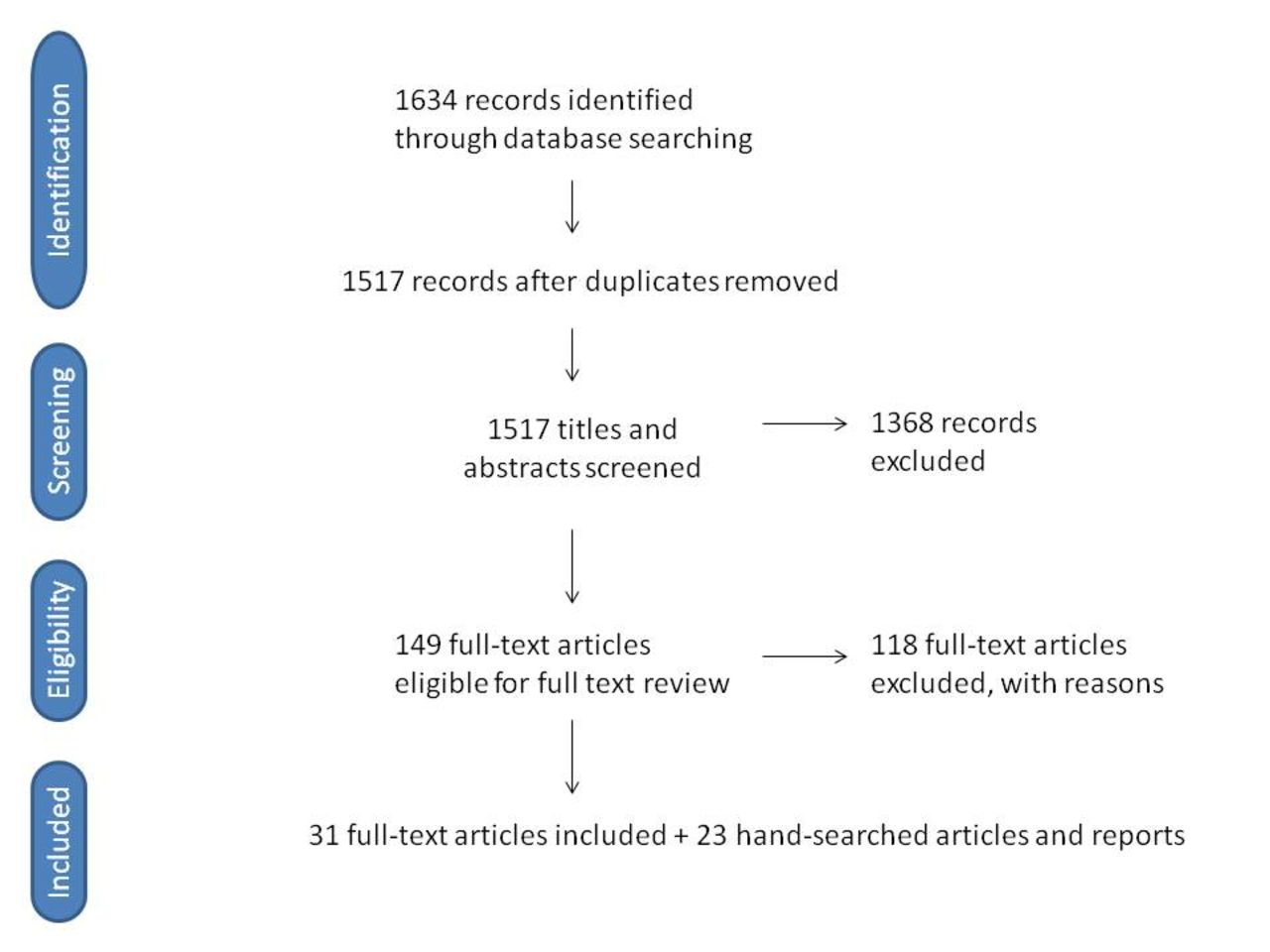
The searches identified 1634 records. After removing 117 duplicates, 1517 titles were screened. A total of 149 papers were reviewed in full text review, of which 118 papers were excluded. Our final sample included 31 papers. An additional 23 articles and reports were identified by the hand searches (figure 1: Flow diagram). Tables 2 and 3 provide an overview of the 45 original research studies and review papers that are included in this review.

{kind=link}
Flow diagram.
Original research articles
Review articles
Overall, the papers indicate that the health needs of children on the move are highly heterogeneous, depending on the conditions in the country of origin, during the journey and after arrival in the countries of destination. Children separated or travelling unaccompanied (UASC) are particularly vulnerable to various forms of exploitation at all phases of their journey and after arrival. Structural, financial, language and cultural barriers in access to healthcare affect care-seeking behaviours as well as diagnostic evaluation, treatment and health outcomes (table 4).6 8 9
Barriers in access to care for children on the move
Communicable diseases
During travel and after arrival in Europe, children may be housed in overcrowded facilities with inadequate hygiene and sanitation conditions that place them at risk of communicable diseases. The most common infection sites include the respiratory tract, gastrointestinal tract and skin, with a concerning prevalence of parasitic and wound infections.10–13
Children originating from low-income and middle-income countries may have been exposed to infectious agents that are rare in high income countries in Europe.14–16 Furthermore, exposure to armed conflict may increase their risk of exposure to infections.17 Notable infections among populations on the move include latent or active tuberculosis (TB),15 18 malaria,17 Hepatitis B and C,15 17 Syphilis,15 Human T-lymphotropic virus type 1 or 2,15 louse-born relapsing fever,17 19 shigella17 and leishmaniasis.17 There is a notable lack of studies with age-disaggregated data on HIV prevalence among migrant children in Europe. A Spanish study which screened 358 children did not find any cases.15 While children on the move are at risk for a number of different infections, the prevalence of communicable diseases varies markedly between groups and is thought to be heavily related to the conditions during travel and after migration.17
The treatment of children on the move with infectious diseases may require different regimens than those recommended by national protocols, as these children may be at higher risk of colonisation and infection with drug-resistant organisms. In Germany, routine screening practices at hospital admission have found that children on the move have higher rates of multiple drug-resistant (MDR) bacterial strains than the local population.20 MDR Infections may be more difficult to treat and carry higher morbidity and mortality risks.
Children on the move may need catch-up immunisations to match the vaccination schedule of the country of destination.17 Several studies of children on the move in Europe have identified low vaccination coverage against hepatitis B, measles, mumps, rubella and varicella and low immunity to vaccine preventable diseases including tetanus and diphtheria: this is coupled with a higher prevalence of previous exposure to vaccine-preventable diseases.21 Since 2015, cases of cutaneous diphtheria17 and outbreaks of measles in the EU22 have been attributed to insufficient vaccination coverage in migrant populations. Further, Hepatitis A cases have been reported in children living in camps and centres in Greece and Germany, with particularly high rates among children under 15 years.23 24 There is no evidence of increased transmission of communicable diseases from migrants to host populations.25
Non-communicable diseases and injuries
Displacement places children at risk for a broad variety of non-communicable diseases and injuries that may be exacerbated by limited and irregular access to paediatric and neonatal healthcare. Paediatric groups that are particularly vulnerable include unaccompanied minors, pregnant adolescents and infants.
In 2017, more than half of the children arriving in Europe were registered in Greece, and the largest age group were infants and small children (0–4 years old).26 Infants born during the journey may be born without adequate access to prenatal, intrapartum or postnatal care, resulting in increased birth complications, stillbirth and infant mortality.27 Further, these newborns may have lacked access to screening for congenital disorders that is routinely offered in European countries. Infant nutrition may suffer, particularly as breastfeeding is a challenge for mothers during their journey.28 The evidence regarding the risk of birth complications in children born to mothers after arrival in the destination country is mixed. Some studies in Europe have shown that these infants have higher rates of birth complications, including hypothermia, infections, low birth weight, preterm birth and perinatal mortality when compared with the native population,13 29 while other studies have found that outcomes in certain countries are similar to the national populations.30 These patterns suggest that the cause of altered risks may be related to society-specific factors such as integration policies, socioeconomic disadvantage among different migrant groups and barriers in access to care.30
Traumatic events such as torture, sexual violence or kidnapping may have long‐lasting physical and psychological effects on a child. Physical trauma related to the journey and attempts at illegal border crossings may include skin lacerations, tendon lacerations, fractures and muscle contusions. If left untreated and/or in unhygienic conditions, injuries may become infected, with severe and potentially life-threatening consequences.12 People arriving by sea are particularly susceptible to injury and illness; a recent survey of rescue ships found that dehydration and dermatological conditions associated with poor hygiene and crowded conditions were common, as well as new and old traumatic injuries from both violence and accidents.31 The risk of female genital mutilation is high in girls from certain regions and is a recognised reason for seeking asylum.32
Nutritional deficiencies and dental problems are more common in children on the move, with reported prevalence of iron deficiency anaemia ranging from 4% to 18% among children living in Germany and Greece.11 33 Dental problems are perhaps the most prevalent health issue in children on the move, and indeed caries prevalence has been reported as high as 65% among migrant and refugee children in the UK.34
While the prevalence of non-communicable chronic diseases in children on the move in the EU is not thought to differ significantly from host populations, there is little evidence to support this thinking. Further, the barriers in access to care and different health beliefs pose challenges to diagnosing and managing children on the move with chronic diseases (tables 2 and 3).
Psychosocial and mental health issues
Children on the move are at high risk for psychosocial and mental health problems, with separated and unaccompanied children at highest risk. Direct and indirect exposure to traumatic events are associated with post-traumatic stress disorder (PTSD), anxiety, depression, sleep disturbances and a broad range of internalising and externalising behaviours in refugee children.35
The mental health of caregivers, especially mothers, plays an important role in their children’s mental and physical health. Maternal PTSD and depression are correlated with increased risk of PTSD, PTS symptoms, behavioural problems and somatic complaints in their children.36 Conversely, good caregiver mental health is a protective factor for the mental and behavioural health of refugee children.35
Transit and host country reception policies also impact the mental health outcomes of children on the move. Numerous studies have documented that postmigration detention increases psychological symptoms and the prevalence of psychiatric illness in children on the move.35 Detention, multiple relocations, prolonged asylum processes and lack of child-friendly immigration procedures are associated with poor mental health outcomes in refugee children and have been described in some studies as having placed the children in greater adverse situations than those which the children endured before migration.35 A longitudinal study of refugee children from the Middle East living in Denmark found that psychological symptoms improved over time, with risk factors related to war and persecution being important during the early years after arrival in Denmark.37 In the longer term, social factors in the country of resettlement were more important predictors of mental health.37
Racism and xenophobia play an important role in the psychological health and well-being of children on the move. Studies in Sweden and Denmark have found that the experience of discrimination is common among youth on the move and is associated with lower rates of social acceptance, poorer peer relations and mental health problems.38 39 In a national survey of Swedish 9th graders, rates of bullying experienced by children on the move were associated with migrant density in schools, whereby children attending schools with low migrant density reported three times the rate of bullying compared with those attending schools with high migrant density.39
Unaccompanied minors
The numbers of unaccompanied and separated children seeking asylum in Europe have increased in recent years. During 2015, 95 205, and in 2016, 63 245 UASC applied for asylum in the 28 EU member states, with Germany receiving about a third of these children.40
The mental health of unaccompanied refugee adolescents during the first years of exile has been studied in several European epidemiological studies in recent years.41–50 In the largest of these studies, a comparison was made between three groups2: (1) newly arrived, unaccompanied children aged 12–18 years in the Netherlands,3 (2) young refugees of the same age who had arrived with their parents and4 (3) an age-matched Dutch group.45 The unaccompanied youths had much higher levels of depressive symptoms than the accompanied refugee children (47% vs 27%), and this was partly explained by a higher burden of traumatic stress. Follow-up interviews 12 months later showed no indication of improvement. The level of externalising symptoms and behaviour problems were, however, lower among the unaccompanied refugees than in the Dutch comparison population. A similar picture of high levels of traumatic stress and introverted symptoms was noted in a Norwegian study of 414 unaccompanied youth; of note, this study was carried out at an average of 3.5 years after their arrival in the country.46
Age assessment
Having an assumed chronological age above or below 18 years determines the support provided for young asylum seekers in most European countries, despite the fact that many lack documents with an exact birth date.6 This has led to the use of many different methods to assess age in Europe. In the UK, social workers independent of the migration authorities undertake age assessment interviews which consider any documents or evidence indicating likely age, along with an assessment of appearance and demeanour.51 Many other European countries rely on medical examinations, primarily in the form of radiographs of the hand/wrist (23 countries), collar bone (15 countries) and/or teeth (17 countries).52 The individual variation in age-specific maturity in the later teens with these methods, and the unknown variation between high-income and low-income countries, make them unsuitable for assessing whether a young person is below or above 18 years of age.53 54
The use of these imprecise methods raise serious ethical and human rights concerns and is often experienced as unfair and stressful by the young asylum seekers.55 The European Academy of Paediatrics and several national medical associations have therefore recommended their members not to participate in age assessment procedures of asylum applicants on behalf of the state.56
Health policies and child rights
Identification of the health needs of an individual child on the move, and subsequent timely investigation and management may be suboptimal in the arrival countries for a plethora of reasons associated with legal status, healthcare system efficiencies and individual factors. A recent survey identified 12 EU/EEA countries with significant inequities in healthcare entitlements for children on the move (compared with locally born children) according to their legal status.57 In a number of countries, undocumented children only have access to emergency healthcare services.58 Worryingly, in Sweden, a recent Human Rights Watch report found that children spend months without receiving health screening.59
In an analysis of healthcare policies for children on the move, Hjern et al 60 compared entitlements for asylum seeking and undocumented children in 31 EU member and EES states in 2016 with those of resident children. Only seven countries (Belgium, France, Italy, Norway, Portugal, Spain and Sweden) have met the obligations of non-discrimination in the CRC and entitled both these categories of migrants, irrespective of legal status, to receive equal healthcare to that of its nationals. Twelve European countries have limited entitlements to healthcare for asylum seeking children. Germany and Slovakia stand out as the EU countries with the most restrictive healthcare policies for refugee children.
In all but four countries in the EU/EEA, there are systematic health examinations of newly settled migrants of some kind.58 In most eastern European countries and Germany, this health examination is mandatory, while in the rest of western and northern Europe it is voluntary. All countries that have a policy of health examination aim to identify communicable diseases, so as to protect the host population. Almost all countries with a voluntary policy also aim to identify the child’s individual healthcare needs, but this is rarely the case in countries that have a mandatory policy.
Discussion
Our review of the available evidence indicates that children on the move in Europe have particular health risks and needs that differ from both the local population as well as between migrant groups. The body of evidence from Europe remains limited; however, as it is based primarily on observational studies from individual countries, with few multicountry or intervention studies. It is important to note that our searches were limited to studies published in English and listed in the PubMed and EMBASE databases. As such, our searches may have missed relevant studies published in other languages, in the grey literature and studies listed in other databases.
A large body of evidence exists on the health needs and risks of children on the move outside of Europe, most notably in North America and Australia.34 61–64 The evidence from these areas indicates that the health determinants and patterns of risk are similar across settings; the specific health risks and needs of children are heavily dependent on the conditions before and during travel and after arrival. There are also patterns that are shared across high-income, middle-income and low-income settings, such as children’s risk of exposure to violence, risk of exploitation and a high risk of mental health problems related to these two factors.65 The similarities across regions suggest that, although context plays an important role for the individual child, there are certain health risks and needs shared by children on the move across the globe.
In light of these similarities, findings from the literature in other parts of the world may help to fill in some of the existing gaps in the evidence in Europe. For example, there is little good quality evidence from Europe on the risk of injury during the early period after arrival to the country of destination. However, a large Canadian study found that refugee children have an increased risk of injury after resettlement. The study reported a 20% higher rate of unintentional injury in refugee youth compared with non-refugee immigrant youth for most causes of injury, with notably higher rates of motor vehicle injuries, poisonings, suffocation and scald burns.66 However, to our knowledge, there are no studies that provide data on the prevalence of disability or its effect on the health and development of children on the move.
There are important contextual factors that are likely to affect the health of children on the move differently across the world. Basic needs such as clean water, sanitation and food security may more profoundly influence child health and well-being in refugee camps in developing countries as compared with Europe. Other contextual factors may include the nature of rights violations, such as the large-scale detention and separation of children on the move from their caregivers in the USA.67 68 Studies in Finnish children separated from their parents for a period during World War II found that these children exhibited altered stress physiology, earlier menarche and lower scores on intelligence testing.69–71 The detention of children together with their families was demonstrated to cause significant, quantifiable harm to children in a comparison study from Australia.72 The interplay between common or widespread health risks, contextual factors, access to care and health promotion activities is likely to play a major role in the ultimate health outcomes of children on the move in a given geographical area.
Newly settled children have greater health needs than the average European child; however, access to healthcare remains a major obstacle for them. Although there have been very few studies assessing access to healthcare by migrant families, it has been proposed that unfamiliar healthcare systems and financial costs of over the counter medications pose specific challenges to the migrant family.8 In the UK, UASC have their specific health needs identified as part of statutory health assessments, where the state has assumed the role of the corporate parent and undertakes the responsibility for the needs of the child. However, accompanied children (those children who arrive with and remain in the care of their migrant, refugee or asylum-seeking parent/s), depend on their newly arrived parent(s) to negotiate unfamiliar healthcare systems.
Other important barriers to care in Europe are similar to those found in other settings, including language barriers, lack of professional medical interpreters and variable cultural competence of health personnel. Health workers may lack knowledge or experience in caring for children on the move, may be unaware of their health rights and may lack guidance on the health needs and risks of the newly arrived population. The International Society for Social Pediatrics and Child Health released a position paper characterising these barriers and providing recommendations for health policy, healthcare, research and advocacy.6 These recommendations are grounded in child rights and can serve as a guide for individuals, groups and organisations seeking to improve the health and well-being of children on the move.
The main health risks and the main challenge for health services for children on the move in Europe are in the domain of mental health. A small prospective longitudinal study from Australia identified modifiable protective factors for refugee children’s social and emotional well-being that related to resettlement practices, family factors and community support.73 This review highlights an important knowledge gap in the evidence in Europe for programmes and policies that address early recognition and intervention, access to care and the development of effective preventive services for mental health. There is an urgent need for research on the effect of interventions and policies intended to promote and protect the health, well-being and positive development of children on the move in Europe.
The remarkable resilience observed among displaced children has been a topic of significant discourse and study.6 Healthy and positive adaptive processes have been associated with social inclusion, supportive family environments, good caregiver mental health and positive school experiences.35 74 Although the evidence base for interventions remains limited, research and experience suggest that the most effective way to protect and promote refugee child mental health is through comprehensive psychosocial interventions that address psychological suffering in the context of the child’s family and environment; such interventions necessarily include family, education and community needs and caregiver mental health.75
Conclusion
Asylum seeking, refugee and undocumented children in Europe have significant health risks and needs that differ between groups and from children in the local population. Health policies across EU and EES member states vary widely, and children on the move in Europe face a broad range of barriers in access to care. The CRC provides children with the right to access to healthcare without discrimination and to the conditions that promote optimal health and well-being. With children increasingly on the move, it is imperative that individuals and sectors that meet and work with these children are aware of their health risks and needs and are equipped to respond to them.
Acknowledgments
The authors would like to thank the ISSOP Migration Working Group, whose work inspired this review paper.
References
Footnotes
Contributors The authors collectively identified the need for the paper. AK designed and carried out the database searches. NS, AH and AK screened titles and abstracts, and all authors screened full text papers. AK, AB and AH wrote sections of the first draft. AK led development and compilation of the first draft and carried out subsequent revisions. All authors contributed to critical review of the drafts and to the development of the supporting tables and figures.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.